chronic inflammation
Reading File
Finding Sources
Searching PubMed
"chronic inflammation"[MeSH Terms] AND mechanisms
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have everything needed for a thorough, well-illustrated answer on chronic inflammation.
Chronic Inflammation
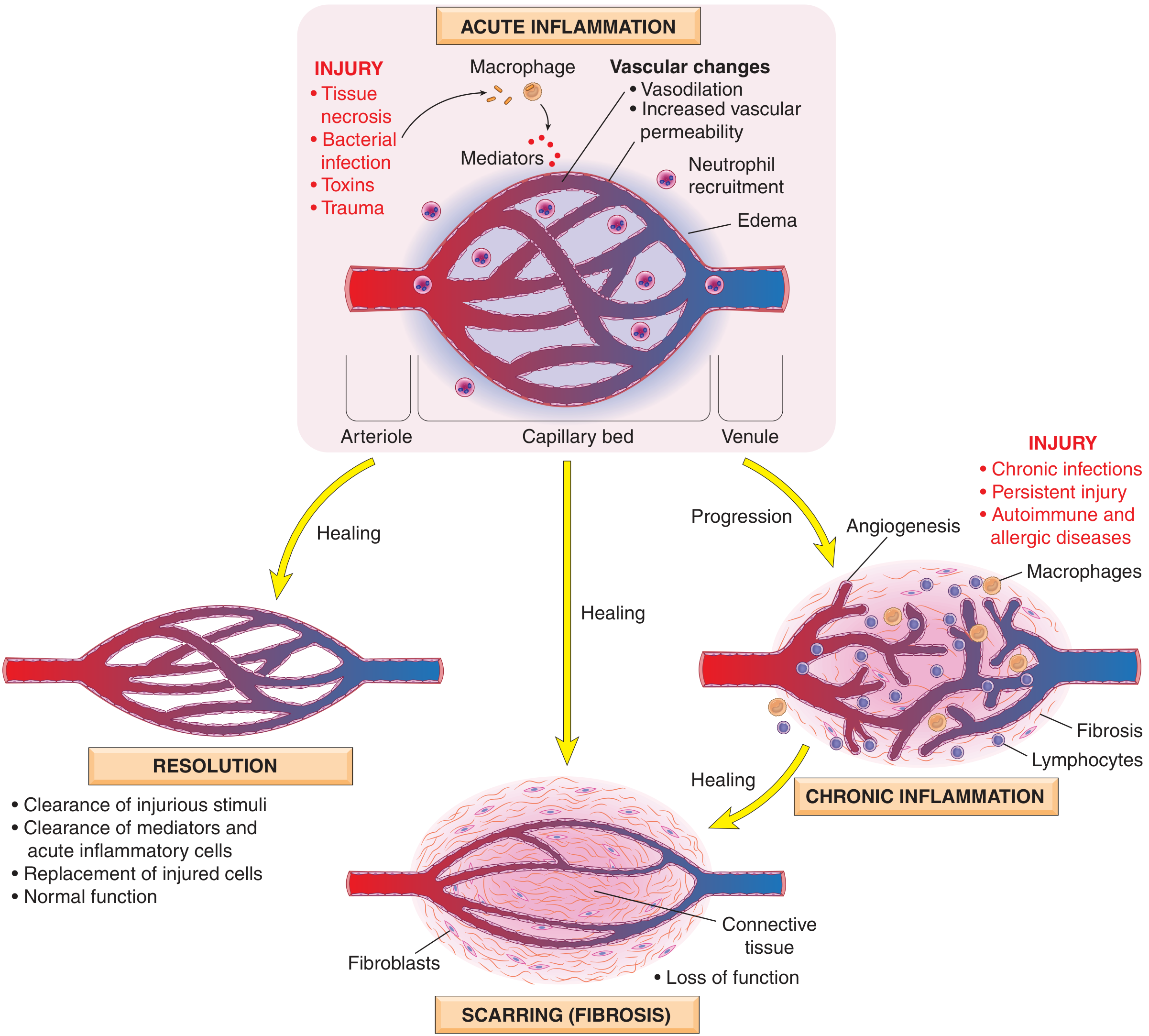
Definition: Chronic inflammation is a response of prolonged duration (weeks to months) in which inflammation, tissue injury, and attempts at repair coexist simultaneously. It may follow unresolved acute inflammation, or arise insidiously without a preceding acute phase - as a smoldering, progressive process. - Robbins & Kumar Basic Pathology, p. 61
Causes
Three main settings trigger chronic inflammation:
-
Persistent infections - Microorganisms that resist eradication: mycobacteria (TB, leprosy), certain viruses, fungi, and parasites. Incompletely resolved acute infection (e.g., bacterial lung abscess) may also evolve into chronicity.
-
Hypersensitivity diseases:
- Autoimmune: Self-perpetuating immune reactions against autoantigens (rheumatoid arthritis, multiple sclerosis, inflammatory bowel disease)
- Allergic: Excessive response to environmental antigens (bronchial asthma)
- These often show mixed acute and chronic patterns due to repeated flares
-
Prolonged exposure to toxic agents:
- Exogenous: inhaled silica particles → silicosis
- Endogenous: excess cholesterol deposition → atherosclerosis
Chronic inflammation is also implicated in diseases not classically thought of as inflammatory, including Alzheimer disease, metabolic syndrome, and type 2 diabetes.
Outcomes of Acute Inflammation
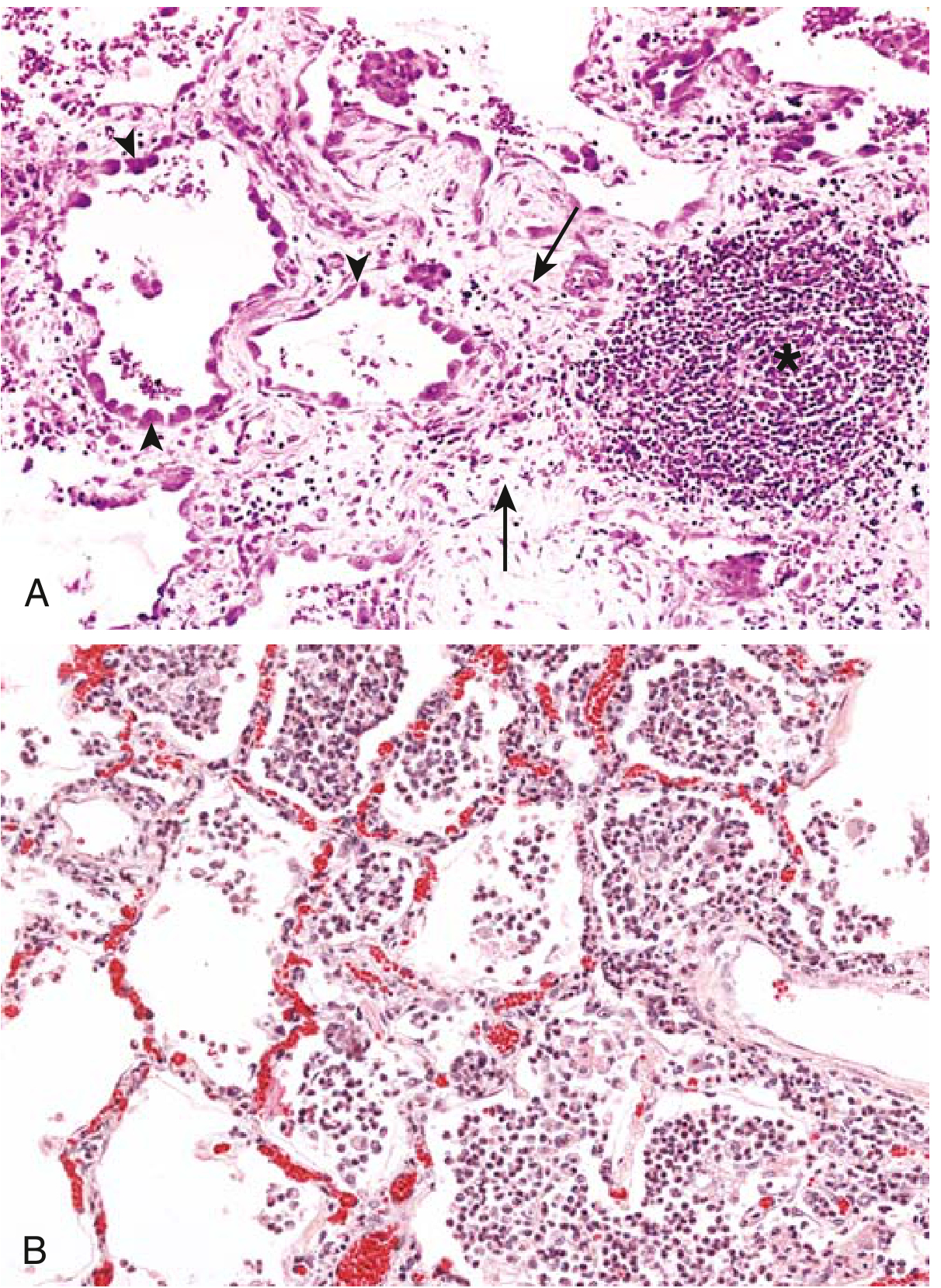
Morphologic Features (Histology)
Chronic inflammation is characterized by three hallmark features (seen together):
| Feature | Details |
|---|---|
| Mononuclear cell infiltration | Macrophages, lymphocytes, plasma cells (not neutrophils) |
| Tissue destruction | Caused by the persistent stimulus and inflammatory cells |
| Repair attempts | Angiogenesis + fibrosis → scar formation |
Cells and Mediators
Macrophages (dominant cell)
Macrophages are the dominant cells in most chronic inflammatory reactions. They are derived from blood monocytes (bone marrow origin) that migrate into tissues. Tissue-resident macrophages include Kupffer cells (liver), microglial cells (CNS), alveolar macrophages (lung), and sinus histiocytes (lymph nodes).
Two functional phenotypes:
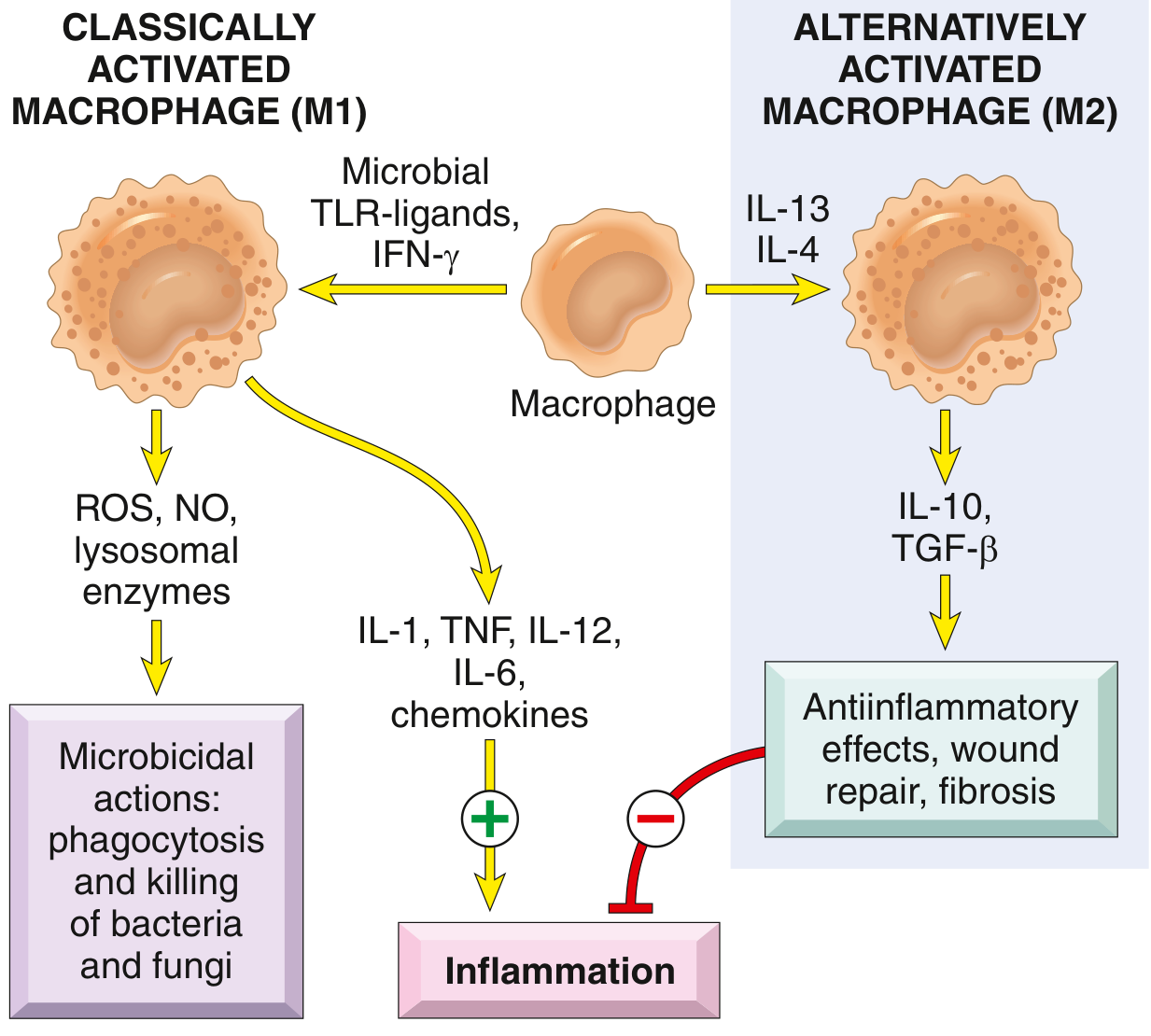
| Type | Trigger | Products | Function |
|---|---|---|---|
| M1 (Classical) | Microbial TLR ligands, IFN-γ | ROS, NO, lysosomal enzymes; IL-1, TNF, IL-12, IL-6, chemokines | Microbicidal, pro-inflammatory |
| M2 (Alternative) | IL-4, IL-13 | IL-10, TGF-β | Anti-inflammatory, wound repair, fibrosis |
Key macrophage functions in chronic inflammation:
- Phagocytosis and killing of microbes / dead tissue
- Secretion of cytokines (TNF, IL-1, chemokines) and eicosanoids - propagating the reaction
- Initiation of tissue repair and fibrosis
- Antigen presentation to T lymphocytes, forming a feedback loop
Lymphocytes
- Activated by microbes and antigens; amplify and perpetuate chronic inflammation
- CD4+ T cell subsets drive different inflammatory patterns:
- Th1 → IFN-γ → classical macrophage activation (M1)
- Th2 → IL-4, IL-5, IL-13 → alternative macrophage activation (M2), eosinophil recruitment
- Th17 → IL-17 → chemokine secretion → neutrophil recruitment
- Th1 and Th17 are involved in chronic autoimmune diseases (e.g., rheumatoid arthritis, IBD)
- Th2 drives allergic inflammation and anti-helminth responses
- B lymphocytes and plasma cells secrete antibodies; present in chronic inflammatory foci
Other Cells
- Eosinophils - characteristic of allergic reactions and parasitic infections; IgE and IL-5 mediated
- Mast cells - release histamine and cytokines; present in connective tissue; participate in both acute and chronic phases
- Neutrophils - typically acute, but can persist in some chronic contexts (e.g., bacterial osteomyelitis, certain autoimmune diseases)
Granulomatous Inflammation
A specialized form of chronic inflammation characterized by aggregates of activated macrophages (epithelioid cells), often surrounded by lymphocytes, and sometimes with multinucleated giant cells and central caseous necrosis.
Mechanism: Th1 lymphocytes secrete IFN-γ → activates macrophages → epithelioid transformation. When the agent cannot be eliminated, the granuloma persists.
Causes:
| Category | Examples |
|---|---|
| Infectious | Tuberculosis (caseating granulomas), leprosy, syphilis, fungal infections (histoplasma, coccidioides), schistosomiasis |
| Non-infectious | Sarcoidosis, Crohn disease, berylliosis, foreign body reactions |
Systemic Effects (Acute Phase Response)
Chronic (and acute) inflammation triggers systemic effects via cytokines (mainly IL-1, TNF, IL-6):
| Effect | Mechanism |
|---|---|
| Fever | Cytokines (TNF, IL-1) → PGE2 production in hypothalamus |
| Leukocytosis | Bone marrow release of leukocytes; colony-stimulating factors increase production |
| Acute-phase proteins | IL-6 → liver synthesis of CRP, fibrinogen, serum amyloid A |
| Septic shock (severe) | Very high TNF levels → hypotension, DIC, metabolic abnormalities |
Outcomes of Chronic Inflammation
- Resolution - if the cause is eliminated (rare in true chronic disease)
- Fibrosis / Scarring - the most common outcome; TGF-β is the key fibrogenic mediator
- Tissue loss and organ dysfunction - e.g., cirrhosis, pulmonary fibrosis, joint destruction
Key Diseases with Chronic Inflammation as Core Pathology
| Disease | Dominant Mechanism |
|---|---|
| Rheumatoid arthritis | Autoimmune Th1/Th17 synovitis |
| Bronchial asthma | Th2-driven eosinophilic airway inflammation |
| Atherosclerosis | Lipid-driven vascular macrophage activation |
| Tuberculosis | Granulomatous Th1 response to M. tuberculosis |
| Crohn disease | Th1/Th17 transmural bowel inflammation |
| Cirrhosis | Persistent hepatic injury + stellate cell-driven fibrosis |
| Silicosis | Macrophage activation by indigestible silica particles |
Sources: Robbins & Kumar Basic Pathology (Robbins Pathology), pp. 61-65; Robbins, Cotran & Kumar Pathologic Basis of Disease.
This is a shared conversation. Sign in to Orris to start your own chat.