Explain in details the mechanical ventilation and the various ventilator settings and features.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full detailed answer.
Mechanical Ventilation: A Comprehensive Overview
Sources: Harrison's Principles of Internal Medicine 22E, Morgan & Mikhail's Clinical Anesthesiology 7e, Miller's Anesthesia 10e, Fishman's Pulmonary Diseases and Disorders, Rosen's Emergency Medicine, Tintinalli's Emergency Medicine, Murray & Nadel's Textbook of Respiratory Medicine
1. What is Mechanical Ventilation?
Mechanical ventilation is a life-support intervention that uses a machine (ventilator) to assist or fully replace spontaneous breathing in patients who cannot adequately ventilate or oxygenate on their own. It operates on the principle of positive-pressure ventilation - the ventilator periodically creates a pressure gradient between the machine circuit and the alveoli, driving gas into the lungs. Exhalation occurs passively when the airway pressure falls and the elastic recoil of the lungs forces air out.
The two physiological goals are:
- CO2 elimination (ventilation) - adjusting minute ventilation (rate × tidal volume)
- Oxygenation - adjusting FiO2 and PEEP
2. Indications for Mechanical Ventilation
Mechanical ventilation is indicated when the following thresholds are crossed:
| Criterion | Measurement |
|---|---|
| Arterial oxygen tension (PaO2) | < 50 mmHg on room air |
| Arterial CO2 tension (PaCO2) | > 50 mmHg without metabolic alkalosis |
| PaO2/FiO2 ratio | < 300 mmHg |
| Alveolar-arterial O2 gradient | > 350 mmHg |
| Dead space/tidal volume (VD/VT) | > 0.6 |
| Respiratory rate | > 35 breaths/min |
| Tidal volume | < 5 mL/kg |
| Vital capacity | < 15 mL/kg |
| Maximum inspiratory force | > −25 cm H2O (e.g., −15 cm H2O) |
- Morgan & Mikhail's Clinical Anesthesiology 7e, Table 58-4
Clinical indicators also include: coma, altered consciousness, cardiac or respiratory arrest, paradoxical breathing pattern, and refractory hypoxemia despite non-invasive measures.
3. Types of Ventilation
3.1 Positive-Pressure Ventilation (PPV)
The dominant and universally preferred technique. The ventilator applies positive pressure to the airway via:
- Invasive access - endotracheal tube (ETT) or tracheostomy tube
- Non-invasive access - tight-fitting mask (NIV, BiPAP, CPAP)
Advantages: Can overcome high airway resistance and low pulmonary compliance.
Disadvantages: Alters V/Q relationships, reduces cardiac output (impairs venous return from increased intrathoracic pressure), risk of barotrauma and volutrauma.
3.2 Negative-Pressure Ventilation (Iron Lung)
Creates negative pressure around the thorax, drawing air in. Rarely used today - cannot overcome significant increases in airway resistance or decreases in compliance, and limits access to the patient.
4. The Four Phases of Every Ventilator Breath
All ventilators share four phases that define each breath cycle:
| Phase | Description |
|---|---|
| Trigger (expiration → inspiration) | The variable that starts a breath (time, pressure, flow, or volume) |
| Target (inspiration) | The upper boundary variable maintained during inspiration (pressure or flow) |
| Cycle (inspiration → expiration) | The variable that terminates inspiration (volume, pressure, flow, or time) |
| Expiration | Passive recoil phase |
Trigger types:
- Time trigger - machine-controlled, breath initiated on a fixed frequency regardless of patient effort
- Pressure trigger - initiated when the patient generates a negative inspiratory pressure (typically −1 to −2 cm H2O)
- Flow trigger - initiated when the ventilator detects a baseline flow change (typically 1-3 L/min) caused by patient effort - more responsive, less work
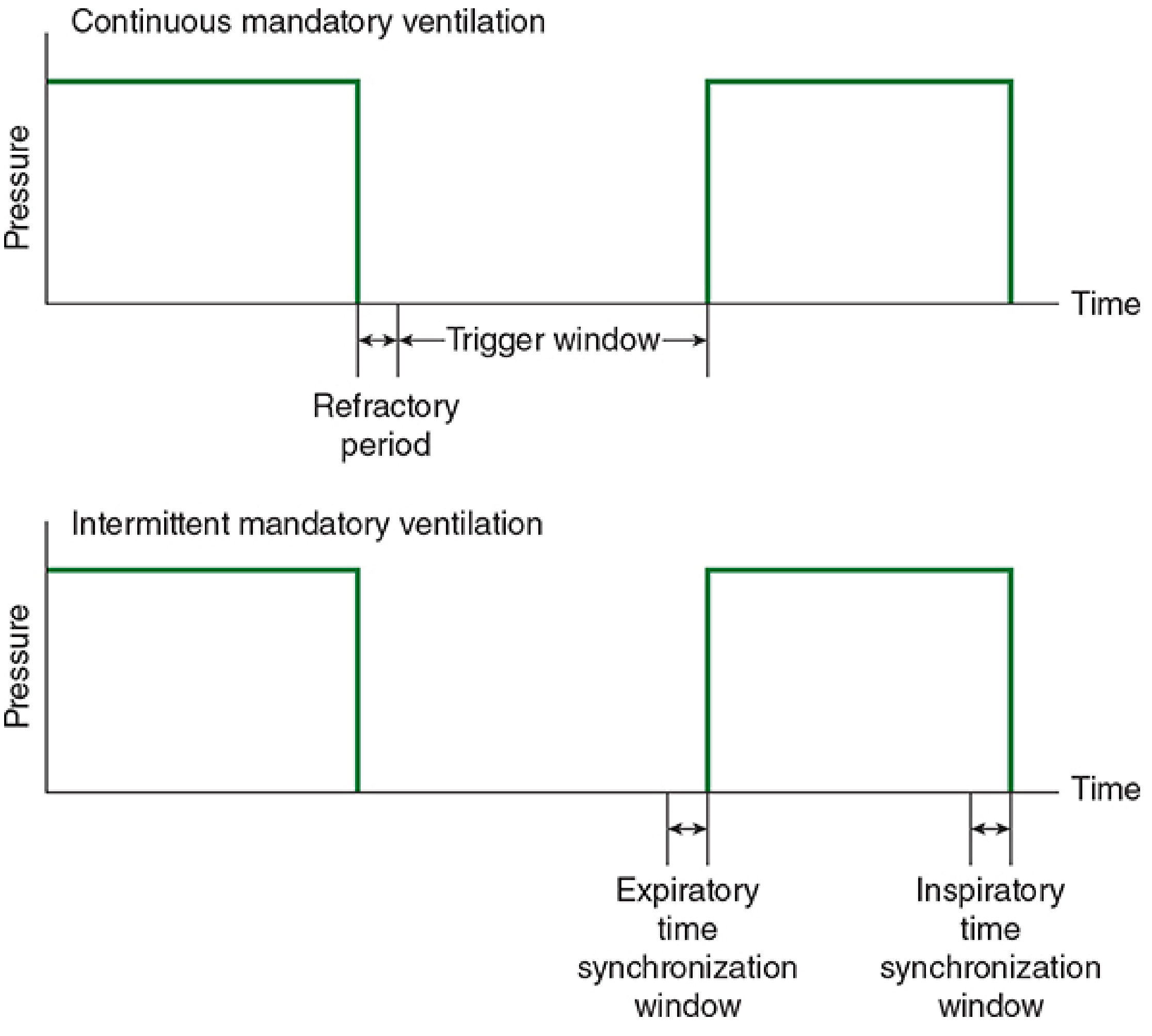
Figure: Trigger window (CMV, top) vs. synchronization window (IMV, bottom). - Morgan & Mikhail's
5. Ventilator Modes
The mode defines: (a) the control variable (pressure vs. volume), and (b) the breath sequence (mandatory, spontaneous, or mixed).
5.1 Assist-Control (AC) - the most common ICU mode
The clinician sets a mandatory respiratory rate and tidal volume (or driving pressure). If the patient makes an inspiratory effort, the ventilator delivers a full, assisted breath at the set parameters. The patient cannot receive less than the set rate.
Two subtypes:
AC-Volume Control (AC-VC)
- Clinician sets: VT, rate, PEEP, FiO2, inspiratory flow rate
- Monitored: peak and plateau airway pressures, minute ventilation (VE)
- The tidal volume is guaranteed; airway pressure is the dependent variable
- Risk: barotrauma if lung compliance drops (pressure rises uncontrolled)
- Must monitor plateau pressure to keep < 30 cm H2O
AC-Pressure Control (AC-PC / PCV)
- Clinician sets: inspiratory driving pressure, rate, PEEP, FiO2
- Monitored: tidal volume, minute ventilation
- VT varies with lung compliance and resistance - must be monitored closely
- Advantage: flow can vary with patient effort (better synchrony, more comfortable)
- Risk: VT not guaranteed - can be too small (hypoventilation) or too large (volutrauma) if patient is making strong respiratory efforts
Pressure-Regulated Volume Control (PRVC)
- Hybrid mode: clinician sets a target VT; the ventilator uses pressure control but auto-adjusts the driving pressure breath-by-breath to achieve the target VT
- Advantage: guarantees VT while allowing variable flow (improved patient synchrony and comfort)
- Risk: variable patient effort can still lead to VT larger than set; must monitor
5.2 Synchronized Intermittent Mandatory Ventilation (SIMV)
A set number of fully supported mandatory breaths are delivered per minute (at set VT or pressure). Between mandatory breaths, the patient can breathe spontaneously from the circuit, but receives no additional support during those spontaneous efforts (unless PSV is added).
The "synchronized" part means the ventilator times each mandatory breath to coincide with the patient's own inspiratory effort when detected, preventing stacking (one breath on top of another).
SIMV rate options:
- High rate (10-12/min): provides nearly all ventilation
- Low rate (1-2/min): minimal support - used for weaning
- IMV has greatest use as a weaning technique
Limitation: At intermediate SIMV rates, it may actually increase work of breathing compared to PSV alone because unsupported spontaneous breaths work against circuit resistance.
5.3 Pressure Support Ventilation (PSV)
A purely patient-triggered mode. Every breath must be initiated by the patient. The ventilator then applies a preset inspiratory pressure (e.g., 10-20 cm H2O above PEEP) to augment the effort. Inspiration ends when flow falls to ~25% of peak flow (flow-cycled).
- Clinician sets: inspiratory pressure level, PEEP, FiO2
- Patient controls: respiratory rate, inspiratory flow, and VT
- Result: excellent patient-ventilator synchrony and comfort
- Primary use: weaning trials (reducing PS level gradually)
- Risk: apnea if patient respiratory drive is inadequate - must monitor VT and rate closely; backup apnea rate should be set
5.4 Continuous Positive Airway Pressure (CPAP)
A spontaneous-breathing-only mode where positive airway pressure is maintained continuously (both inspiration and expiration). The patient does all the work of breathing; the machine simply maintains a baseline pressure.
Used for:
- Obstructive sleep apnea
- Mild hypoxemia
- Weaning trials (spontaneous breathing trials at low CPAP levels)
- NIV in select patients
5.5 Airway Pressure Release Ventilation (APRV)
Maintains a high continuous pressure (Phigh, typically 20-30 cm H2O) for most of the respiratory cycle, with brief, intermittent releases to a low pressure (Plow, often 0 cm H2O). The release creates a brief expiratory phase, and spontaneous breathing is allowed throughout.
- Achieves alveolar recruitment via sustained high pressure
- Used in ARDS as an alternative open-lung strategy
- Complex to manage; patient must be able to breathe spontaneously
6. Key Ventilator Settings
6.1 Tidal Volume (VT)
The volume delivered with each mechanical breath.
- Normal physiologic VT: ~7 mL/kg ideal body weight (IBW)
- Standard initial setting: 8 mL/kg IBW
- Lung-protective (ARDS): 6 mL/kg predicted body weight (PBW) - the ARDSNet protocol
- Avoid: < 6 or > 10 mL/kg as both extremes increase risk (atelectasis vs. volutrauma)
- Large VT causes volutrauma - repetitive overdistension and collapse of alveoli
- Must always monitor plateau pressure alongside VT
6.2 Respiratory Rate (RR)
- Initial setting: 12-16 breaths/min in most adults
- In ARDS/low VT strategy: may need to increase to 20-30/min to maintain adequate minute ventilation and prevent severe hypercapnia
- In obstructive disease (asthma, COPD): use lower rates (< 10/min) to allow adequate expiratory time and prevent auto-PEEP
- Rate controls CO2 elimination: increasing rate lowers PaCO2; decreasing rate raises PaCO2
6.3 FiO2 (Fraction of Inspired Oxygen)
- Range: 0.21 (room air) to 1.0 (100% oxygen)
- Initial setting: start at 1.0 during intubation, then titrate down
- Target: lowest FiO2 that achieves SpO2 ≥ 92-94% (or PaO2 > 60 mmHg)
- Avoid: prolonged FiO2 > 0.6 due to oxygen toxicity (free radical injury, absorptive atelectasis)
- FiO2 > 0.7 is considered potentially toxic with prolonged use; target nontoxic levels using PEEP to recruit alveoli
6.4 PEEP (Positive End-Expiratory Pressure)
PEEP is the airway pressure maintained at end-expiration by a threshold valve on the expiratory limb. It is the most powerful tool for improving oxygenation.
Mechanism of action:
- Increases FRC (functional residual capacity), keeping alveoli above closing capacity
- Recruits (reopens) partially collapsed alveoli - most effective above the lower inflection point on the P-V curve
- Redistributes pulmonary edema from alveolar to peribronchial spaces, improving gas exchange
- Corrects V/Q mismatch and intrapulmonary shunting
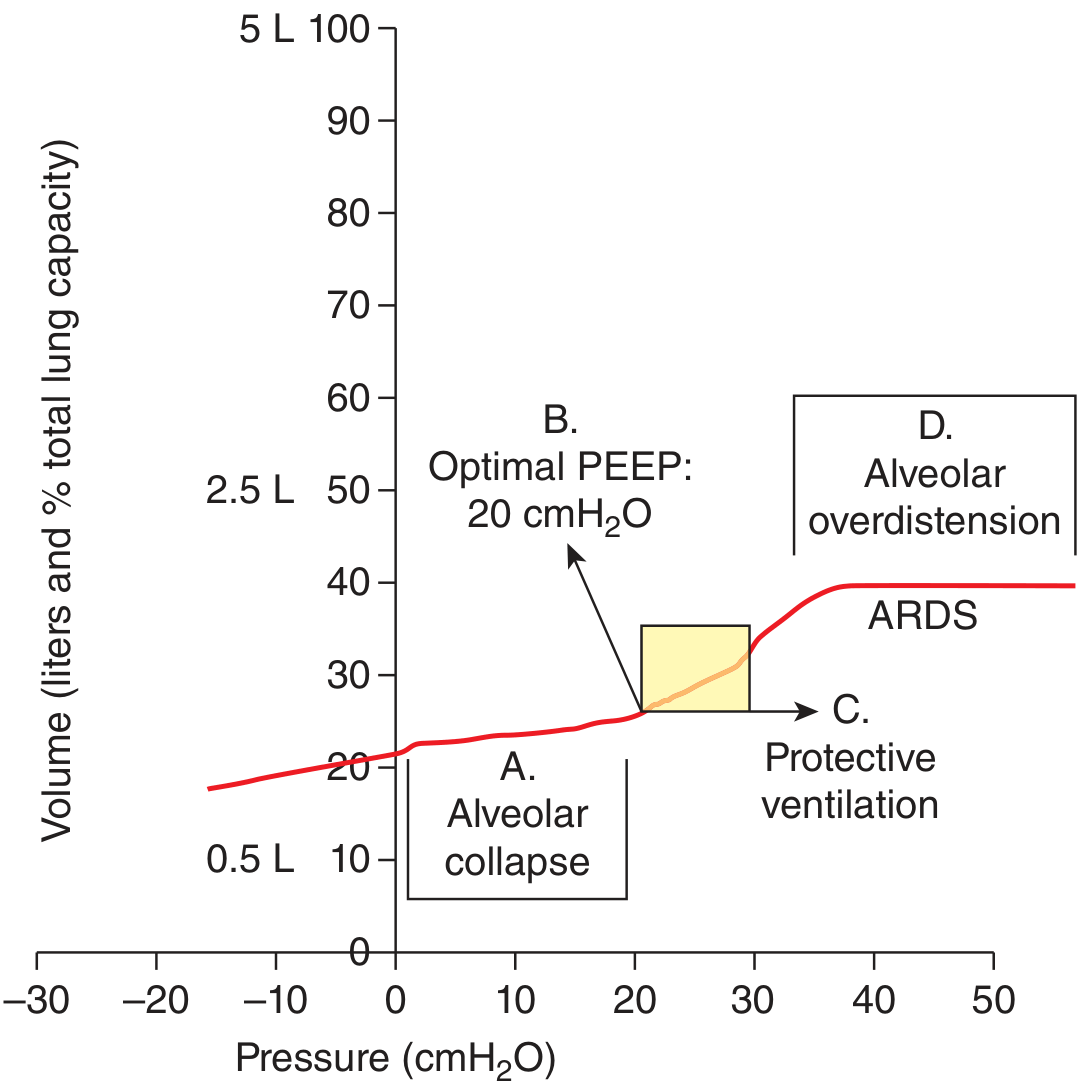
Figure: Pressure-volume curve in ARDS. Optimal PEEP (B, ~20 cmH2O) is set above the lower inflection point (zone A, alveolar collapse) and VT lands in the steep compliant zone (C), staying below the upper deflection point (D, overdistension). - Harrison's Principles of Internal Medicine 22E
PEEP settings:
- Standard "physiologic" PEEP: 5 cm H2O (maintains FRC, prevents atelectasis)
- Therapeutic PEEP: 5-15 cm H2O in hypoxemia
- High PEEP: > 15 cm H2O in severe ARDS (with caution)
- Best PEEP: the lowest PEEP achieving adequate oxygenation at non-toxic FiO2 without hemodynamic compromise
Adverse effects of PEEP:
- Reduced venous return and decreased cardiac output (especially at high levels or in hypovolemia)
- Barotrauma/pneumothorax if excessive
- Increased dead space (overdistended non-dependent alveoli get ventilation but reduced perfusion)
- Increased intracranial pressure (reduces venous drainage)
CPAP vs. PEEP: In strict terminology, PEEP applies during mechanically assisted breaths; CPAP is positive pressure applied continuously during spontaneous breathing. In clinical practice the terms are often used interchangeably.
6.5 Inspiratory Flow Rate and Pattern
- Typical initial setting: 60 L/min for volume-controlled modes
- In obstructive disease: increase to > 60-80 L/min - allows faster delivery of the breath, shortening inspiratory time and thus prolonging expiratory time (reduces auto-PEEP)
- Flow waveforms available:
- Square (constant): fixed flow throughout inspiration
- Decelerating (ramp): peak flow at onset that tapers - produces lower peak pressures, better gas distribution, preferred in pressure-limited settings
- Sinusoidal: mimics normal breathing effort
6.6 Inspiratory:Expiratory (I:E) Ratio
- Normal spontaneous breathing: approximately 1:2 to 1:3
- Standard ventilator setting: 1:2 (inspiration is shorter than expiration)
- In obstructive disease (asthma/COPD): prolong expiration to 1:3, 1:4 or even 1:5 to allow complete expiration and prevent auto-PEEP
- Inverse ratio ventilation (IRV): I:E of 1:1 to 4:1 (inspiration > expiration), used as a rescue strategy in ARDS to improve oxygenation by prolonging mean airway pressure - requires deep sedation/paralysis
6.7 Plateau Pressure (Pplat)
Not a set value but a monitored variable - measured during an end-inspiratory pause (when flow = zero). Reflects the actual alveolar pressure.
- Target: < 30 cm H2O (lung-protective threshold)
- < 16 cm H2O associated with lowest postoperative pulmonary complications
- Driving pressure = Pplat - PEEP: reflects stress on the lung parenchyma; a driving pressure > 15 cm H2O is independently associated with mortality in ARDS
6.8 Trigger Sensitivity
How easily the ventilator detects a patient's inspiratory effort.
- Pressure trigger: set at −1 to −2 cm H2O below baseline
- Flow trigger: set at 1-3 L/min change from baseline
- Too sensitive: auto-triggering from cardiac oscillations or secretions
- Too insensitive: increases patient work of breathing (patient must generate large effort before ventilator responds)
Flow triggering is generally preferred as it is more sensitive and reduces work of breathing.
7. Cycling Mechanisms (How Inspiration Ends)
| Cycling Type | End of Inspiration Triggered By | Notes |
|---|---|---|
| Volume cycled | Preset volume delivered | Most adult ICU ventilators; secondary pressure limit guards against barotrauma |
| Pressure cycled | Airway pressure reaches preset limit | VT varies with compliance/resistance; a circuit leak prevents cycling |
| Flow cycled | Flow drops to ~25% of peak (used in PSV) | More natural feel; allows variable inspiratory time |
| Time cycled | Preset inspiratory time elapses | Used in HFJV, some neonatal ventilators |
8. Special Modes and Advanced Features
8.1 High-Frequency Ventilation (HFV)
Three subtypes deliver VT at or below anatomic dead space at very high rates:
| Type | Rate | Notes |
|---|---|---|
| HFPPV (High-Freq Positive Pressure) | 60-120/min | Small "conventional" VT |
| HFJV (High-Freq Jet Ventilation) | 120-600/min (2-10 Hz) | Jet cannula in airway; may entrain air (Bernoulli); used for airway surgery |
| HFOV (High-Freq Oscillation) | 180-3000/min (3-50 Hz) | Piston driver creates to-and-fro gas movement; used in severe ARDS |
Gas exchange occurs via convection, asymmetric velocity profiles, molecular diffusion, and the Pendelluft effect. Initial HFJV settings: rate 120-240/min, inspiratory time 33%, drive pressure 15-30 psi.
8.2 Non-Invasive Ventilation (NIV)
Delivered via tight-fitting mask rather than ETT. Modes include:
- CPAP - single pressure level; opens upper airway; used in OSA, mild pulmonary edema
- BiPAP (Bilevel PAP) - separate IPAP (inspiratory positive airway pressure) and EPAP (expiratory positive airway pressure); improves V/Q; used in COPD exacerbation, hypercapnic respiratory failure, CHF
Requires intact airway reflexes and cooperative patient. CPAP masks limited to < 15 cm H2O (lower than lower esophageal sphincter pressure) to reduce risk of gastric distension and aspiration.
8.3 Differential (Independent) Lung Ventilation
Uses a double-lumen ETT to ventilate each lung separately with different settings. Used in:
- Severe unilateral lung disease
- Bronchopleural fistula
- Situations where conventional PPV + PEEP aggravates V/Q mismatch in one lung
9. Lung-Protective Ventilation Strategy
The cornerstone of management in ARDS and is being applied more broadly to all mechanically ventilated patients:
| Parameter | Target |
|---|---|
| Tidal volume | 6 mL/kg predicted body weight |
| Plateau pressure | ≤ 30 cm H2O |
| Driving pressure (Pplat - PEEP) | ≤ 15 cm H2O |
| PEEP | Titrated to maintain oxygenation with FiO2 ≤ 0.6 |
| FiO2 | Lowest achieving SpO2 ≥ 92% |
| RR | Up to 30/min to compensate for low VT if needed |
The landmark ARDSNet trial showed that VT of 6 mL/kg vs 12 mL/kg PBW reduced 28-day mortality in ARDS from ~40% to ~31%.
Permissive hypercapnia - allows PaCO2 to rise (typically up to 50-70 mmHg, accepting pH > 7.20) rather than using large VT to normalize CO2. Generally well tolerated. Avoid if: raised intracranial pressure, severe cardiac dysfunction, or pulmonary hypertension.
10. Ventilator-Induced Lung Injury (VILI)
Mechanical ventilation can itself injure the lungs through several mechanisms:
| Mechanism | Definition |
|---|---|
| Barotrauma | Injury from excessive airway pressure; causes pneumothorax, pneumomediastinum, subcutaneous emphysema |
| Volutrauma | Injury from alveolar overdistension (excessive VT) even without high pressure |
| Atelectrauma | Repetitive collapse and reopening of unstable alveoli at end-expiration; shear stress injures alveolar walls |
| Biotrauma | Release of inflammatory mediators from mechanically stressed lung, contributing to multi-organ failure |
Lung-protective ventilation targets all four by limiting both pressure (Pplat < 30) and volume (VT ≤ 6 mL/kg) and using PEEP to prevent atelectrauma.
11. Adverse Effects of Mechanical Ventilation
- Cardiovascular: increased intrathoracic pressure reduces venous return and cardiac output; worsened by high PEEP and hypovolemia
- Barotrauma: pneumothorax, pneumomediastinum - especially in obstructive disease
- Ventilator-associated pneumonia (VAP): a leading cause of nosocomial infection; prevention bundles are critical
- Auto-PEEP (intrinsic PEEP): incomplete exhalation before next breath starts; air trapping causes dynamic hyperinflation; common in asthma/COPD; measured by expiratory pause maneuver
- Hemodynamic compromise from auto-PEEP: raised intrathoracic pressure reduces cardiac output; treatment is slowing RR and/or briefly disconnecting the circuit
- Oxygen toxicity: prolonged high FiO2 causes direct free-radical lung injury and absorptive atelectasis
12. Weaning and Liberation from Mechanical Ventilation
Weaning should be considered when the underlying cause is resolving and the patient meets readiness criteria:
Readiness criteria:
- Stable hemodynamics (no/low vasopressors)
- FiO2 ≤ 0.4-0.5 and PEEP ≤ 5-8 cm H2O
- PaO2/FiO2 > 150-200
- Awake and following commands
- Adequate cough and airway protection reflexes
Weaning methods:
- Spontaneous Breathing Trial (SBT) - 30-120 min trial on CPAP (5 cm H2O) or T-piece (no support); assess tolerance; failure = increased RR, SpO2 drop, distress, hemodynamic instability
- Pressure Support weaning - progressively reduce PSV level from ~20 cm H2O to ~5-8 cm H2O over hours to days
- SIMV weaning - gradually reduce mandatory rate from full to minimal support (less preferred as it may increase work of breathing at intermediate rates)
The RSBI (Rapid Shallow Breathing Index) = RR/VT (L) is used to predict weaning success:
- RSBI < 80-100 breaths/min/L = favorable for extubation
Summary Table: Common Ventilator Settings at a Glance
| Setting | Typical Range | Key Consideration |
|---|---|---|
| Mode | AC-VC, AC-PC, PSV, SIMV | Choose based on patient stability and breathing effort |
| Tidal Volume (VT) | 6-8 mL/kg IBW | ≤ 6 mL/kg in ARDS |
| Respiratory Rate | 12-20/min | Lower in obstructive disease |
| FiO2 | 0.21-1.0 | Target SpO2 ≥ 92%, minimize over time |
| PEEP | 5-15 cm H2O | "Best PEEP" = adequate O2 at FiO2 ≤ 0.6 |
| Inspiratory Flow | 40-80 L/min | Higher in obstructive disease |
| I:E Ratio | 1:2 standard | 1:3 to 1:5 in obstructive; reversed in ARDS |
| Plateau Pressure | Target < 30 cm H2O | Monitored, not set |
| Trigger Sensitivity | Flow: 1-3 L/min; Pressure: −1 to −2 cm H2O | Flow triggering preferred |
| Pressure Support | 5-20 cm H2O above PEEP | Set to achieve VT 6-8 mL/kg in PSV mode |
Key references:
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Chapter 58
- Harrison's Principles of Internal Medicine 22E - Chapter 313
- Fishman's Pulmonary Diseases and Disorders - Chapter 141
- Rosen's Emergency Medicine - Chapter on Mechanical Ventilation
- Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.