Perioperative ventricular tachycardia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ventricular tachycardia" AND perioperative
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive material from multiple authoritative sources. Let me compile the full response.
Perioperative Ventricular Tachycardia
Overview
Ventricular tachycardia (VT) in the perioperative period ranges from clinically benign nonsustained runs to immediately life-threatening sustained VT or VF. Management depends on the morphology (monomorphic vs. polymorphic), hemodynamic consequences, and whether the patient has an underlying substrate (structural heart disease, ischemia, channelopathy, or proarrhythmic drug exposure).
Classification
| Type | Key Features |
|---|---|
| Nonsustained VT (NSVT) | <30 s, terminates spontaneously; not independently associated with increased perioperative risk |
| Sustained monomorphic VT | >30 s or requires termination; typically scar-mediated (prior MI, cardiomyopathy) |
| Polymorphic VT | Changing QRS morphology; suggests ischemia, electrolyte disturbance, or drug toxicity |
| Torsades de Pointes (TdP) | Subtype of polymorphic VT; "twisting of the points" pattern; driven by QT prolongation |
| Pulseless VT | No cardiac output; treated identically to VF |
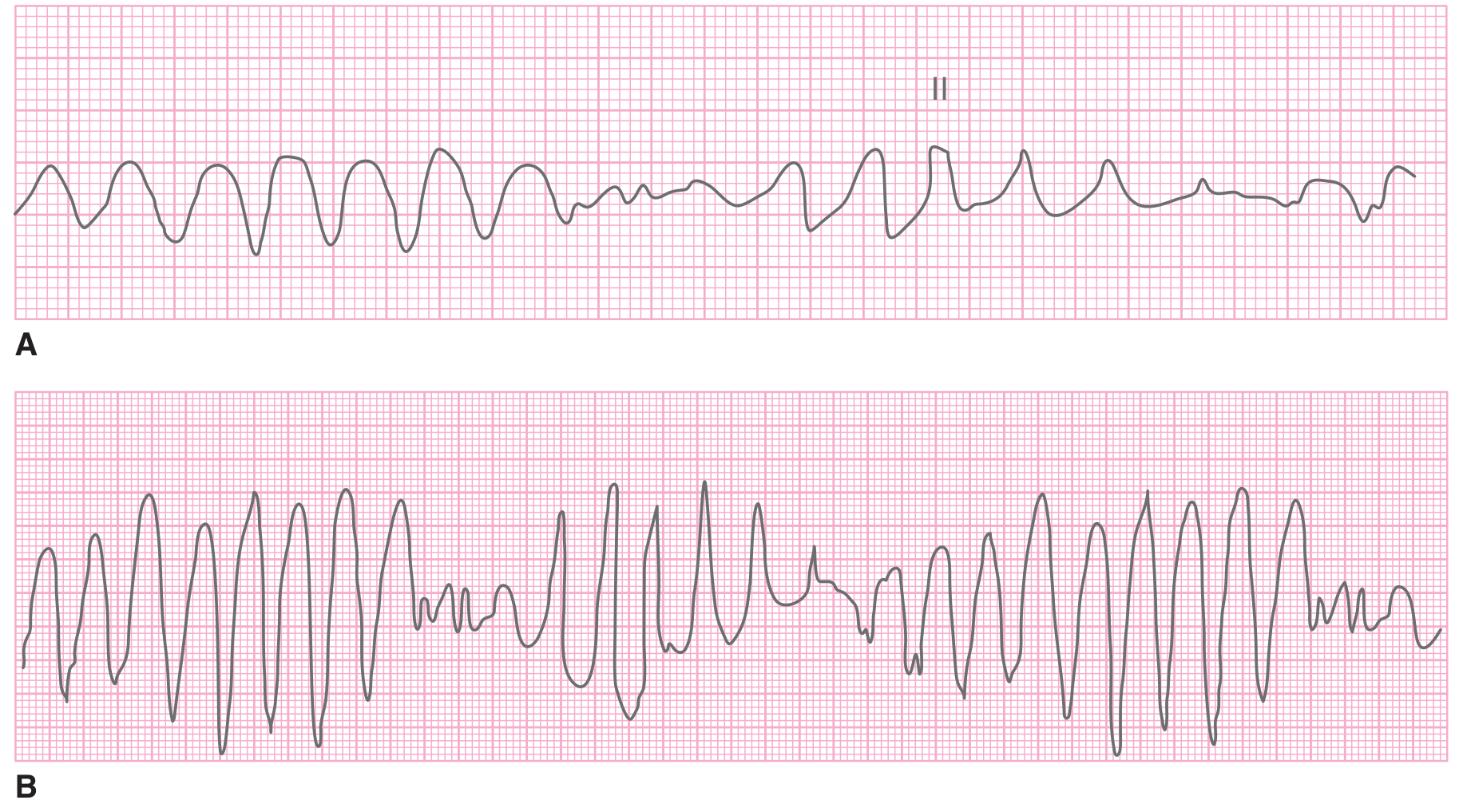
Figure: (A) Polymorphic VT and (B) Torsades de Pointes - note the characteristic progressively changing QRS complex amplitude and direction in TdP. - Tintinalli's Emergency Medicine, p. 157
Preoperative Risk Assessment
- NSVT and PVCs: Not independently associated with increased perioperative risk and do not require further intervention prior to surgery, unless they reflect an underlying reversible cause (ischemia, electrolyte disturbance, drug toxicity). - Maingot's Abdominal Operations, p. 32
- Sustained VT: A life-threatening rhythm that must be terminated (chemically or electrically) before any elective noncardiac surgery. These rhythms have the potential to be life-threatening and prompt stabilization must occur first.
- Monomorphic sustained VT is typically scar-mediated (ischemic heart disease, non-ischemic cardiomyopathy).
- Polymorphic VT more likely reflects acute ischemia, metabolic derangement, or an iatrogenic/drug cause.
- Underlying cardiomyopathy (dilated, hypertrophic, arrhythmogenic right ventricular cardiomyopathy) substantially elevates VT risk. - Fuster and Hurst's The Heart, 15th Ed., p. 2097
Intraoperative Triggers / Causes
The surgical and anesthetic environment creates multiple pro-arrhythmic conditions:
- Ischemia - most important cause of new-onset polymorphic VT intraoperatively; must be excluded in any new VT
- Electrolyte abnormalities - hypokalemia and hypomagnesemia lower the VF/VT threshold
- Autonomic surges - laryngoscopy, surgical stimulation, catecholamine release
- Volatile anesthetics - sensitize the myocardium; in congenital long QT syndrome, volatile agents prolong QT and can precipitate TdP (switching to TIVA is part of management)
- QT-prolonging drugs - suxamethonium, haloperidol, many antibiotics (azithromycin, fluoroquinolones), ondansetron, and others can provoke TdP
- Hypothermia - increases risk of VF
- Hypoxia / hypercapnia
- Electrocautery artefact causing ICD misclassification and inappropriate therapy
Acute Management Algorithm
Step 1: Assess hemodynamic stability immediately
Pulseless VT / VF:
- Immediate unsynchronized defibrillation (no delay for medication)
- Begin CPR; continue ACLS protocol
- Effective uninterrupted chest compressions and defibrillation take precedence over medications. - Barash Clinical Anesthesia, 9e, p. 4893
- Epinephrine 1 mg IV every 3-5 minutes
- Amiodarone 300 mg IV bolus (or lidocaine 1-1.5 mg/kg if amiodarone unavailable)
- Concurrently identify and reverse reversible causes (4 H's and 4 T's)
Hemodynamically unstable VT with pulse:
- Immediate synchronized electrical cardioversion
- Sedate with procedural analgesia/sedation if clinical status allows - Tintinalli's Emergency Medicine, p. 157
Hemodynamically stable VT with pulse:
- Pharmacologic therapy first-line (see below)
- Monitor and prepare for cardioversion if patient deteriorates
Step 2: Pharmacologic agents for stable VT
| Drug | Dose | Notes |
|---|---|---|
| Procainamide | 10-17 mg/kg IV at 20-50 mg/min | Superior to amiodarone or lidocaine for conversion of stable VT; monitor for hypotension |
| Amiodarone | 150 mg IV over 10 min, then 1 mg/min infusion | Broadly effective; useful with reduced EF |
| Lidocaine | 1-1.5 mg/kg IV bolus | Rapidly available in OR; useful post-MI VT |
| Magnesium sulfate | 25-50 mg/kg IV over 2-3 min | Drug of choice for TdP and hypomagnesemia-associated VT |
Procainamide is superior to amiodarone or lidocaine for converting stable VT. Its primary disadvantage is the need for slow infusion due to hypotension risk. - Tintinalli's Emergency Medicine, p. 157
Step 3: Polymorphic VT / Torsades de Pointes - specific management
From Miller's Anesthesia (Box 29.7 - Treatment of Polymorphic VT/TdP in LQTS):
| Step | Action |
|---|---|
| Recognize | External defibrillation (or remove magnet from ICD if in place) |
| Stop precipitating cause | Pause surgery; administer analgesia; stop beta-agonists; correct electrolytes (especially hypokalemia); switch volatile anesthetic to TIVA |
| Therapeutic treatment | Magnesium sulfate 25-50 mg/kg IV over 2-3 min; second bolus 2-4 mg/kg after 15 min if recurrence; consider transvenous overdrive pacing at 90-110 bpm |
| Postoperative care | Admit to ICU/cardiac care unit for ECG monitoring |
- Miller's Anesthesia, 10e, p. 4172
Definitive treatment of recurrent TdP is ventricular overdrive pacing to prevent the pause-dependent initiation of polymorphic runs, continued until the QT-prolonging cause is corrected.
Patients with ICDs
Patients with an ICD present a special perioperative scenario:
- ICDs detect VT/VF by rate, QRS morphology, and chamber-of-onset criteria; sensitivity and specificity for VT detection by QRS morphology is >90%
- ATP (antitachycardia pacing) terminates slow VT (<188-200 bpm) ~90% of the time
- Electrocautery (monopolar) above the umbilicus poses the highest risk of inappropriate ICD therapy
- Before surgery: turn off ICD tachytherapies by magnet placement or reprogramming; connect patient to external defibrillator as backup until ICD is restored postoperatively
- ICD tachytherapies should be re-enabled immediately after surgery
- Pacemaker-dependent patients: reprogram to DOO or VOO to prevent oversensing and pacing failure - Fuster and Hurst's The Heart, 15th Ed., p. 2097; Miller's Anesthesia, 10e
Perioperative Cardiac Arrest: Survival Context
- In-hospital cardiac arrest survival: ~25%
- Perioperative cardiac arrest survival is substantially better: ~40%, reflecting the monitored environment, immediately available resuscitation equipment, and trained personnel
- Brain ATP is depleted after 4-6 min of no flow; returns to near-normal within 6 min of effective CPR
- ETCO2 is an excellent, immediately available noninvasive monitor of CPR efficacy in the OR - Barash Clinical Anesthesia, 9e, p. 4893
Preoperative Considerations for High-Risk Patients
| Scenario | Recommendation |
|---|---|
| Known sustained VT / prior cardiac arrest | ICD implantation before elective surgery (primary or secondary prevention); optimize underlying disease |
| HCM with VT risk | TOE guidance intraoperatively; avoid arterial dilation and overdiuresis; TIVA preferred over volatile if LQTS concern |
| Congenital LQTS | Preoperative cardiology review; avoid QT-prolonging perioperative drugs; TIVA over volatile; magnesium prophylaxis considered |
| Recent MI with NSVT | Does not independently elevate perioperative risk; optimize ischemic therapy |
| Structural heart disease + NSVT | Investigate for ischemia; ensure optimal medical therapy; may not require delay |
Key Points Summary
- NSVT and PVCs do not independently increase perioperative risk and do not require preoperative intervention.
- Sustained VT must be terminated before elective noncardiac surgery; ischemia must be excluded as the cause.
- Monomorphic VT is usually scar-mediated; polymorphic VT suggests ischemia, electrolytes, or drug effect.
- Pulseless VT = immediate defibrillation, then CPR and ACLS.
- Stable VT: procainamide > amiodarone or lidocaine for pharmacologic conversion.
- TdP: magnesium sulfate, remove precipitant, switch to TIVA, overdrive pacing if recurrent.
- ICD patients: disable tachytherapies before monopolar electrocautery; keep external defibrillator available.
- Perioperative VF/VT cardiac arrest has a ~40% survival - better than other in-hospital settings due to monitored environment.
Sources:
- Fuster and Hurst's The Heart, 15th Ed. - Uncontrolled Arrhythmias and High-Degree Conduction Disease, p. 2097
- Miller's Anesthesia, 10e - Implantable Cardioverter-Defibrillators; Box 29.7 TdP Management
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - Resuscitation in the Operating Room, p. 4893
- Tintinalli's Emergency Medicine - Ventricular Tachycardia Treatment, p. 157
- Maingot's Abdominal Operations - Congestive Heart Failure and Arrhythmia, p. 32
Recent literature note: A 2025 systematic review (PMID 40237657) compared sedation vs. general anesthesia for VT ablation procedures, and a 2026 review (PMID 42366132) addresses VA-ECMO use in high-risk VT ablation - relevant for the expanding perioperative electrophysiology context.
This is a shared conversation. Sign in to Orris to start your own chat.