Demonstrate the anomalies of Female Reproductive system.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive information and high-quality images to deliver a thorough answer. Let me compile the complete response.
Anomalies of the Female Reproductive System
Congenital uterine anomalies occur in 1%-15% of the general female population, rising to 5%-10% in women with early pregnancy loss, and up to 25% in those with second or third trimester losses. They result from abnormal development, fusion, or resorption of the paired Müllerian (paramesonephric) ducts, which form the uterus, the upper two-thirds of the vagina, and the fallopian tubes by week 20 of gestation. Because of the anatomical proximity of the paramesonephric ducts to the urinary system, renal anomalies coexist in 30%-50% of cases (especially agenesis and ectopia), and dedicated renal imaging is mandatory when a Müllerian anomaly is diagnosed.
Gold standard imaging: Pelvic MRI (T2-weighted, with coronal and axial oblique planes) - superior to ultrasound (US) or hysterosalpingography (HSG) for classification, especially for rudimentary horns.
Classification: Buttram & Gibbons / American Fertility Society
Class I - Uterine Agenesis or Hypoplasia
Failure of both Müllerian ducts to develop normally. Ovaries are intact and normal, which distinguishes this from androgen insensitivity syndrome and gonadal dysgenesis.
Mayer-Rokitansky-Küster-Hauser (MRKH) Syndrome is the commonest subtype - uterine and vaginal agenesis/hypoplasia with intact ovaries and fallopian tubes. Detection of uterine remnants is difficult on US; sagittal and axial MRI are more reliable.
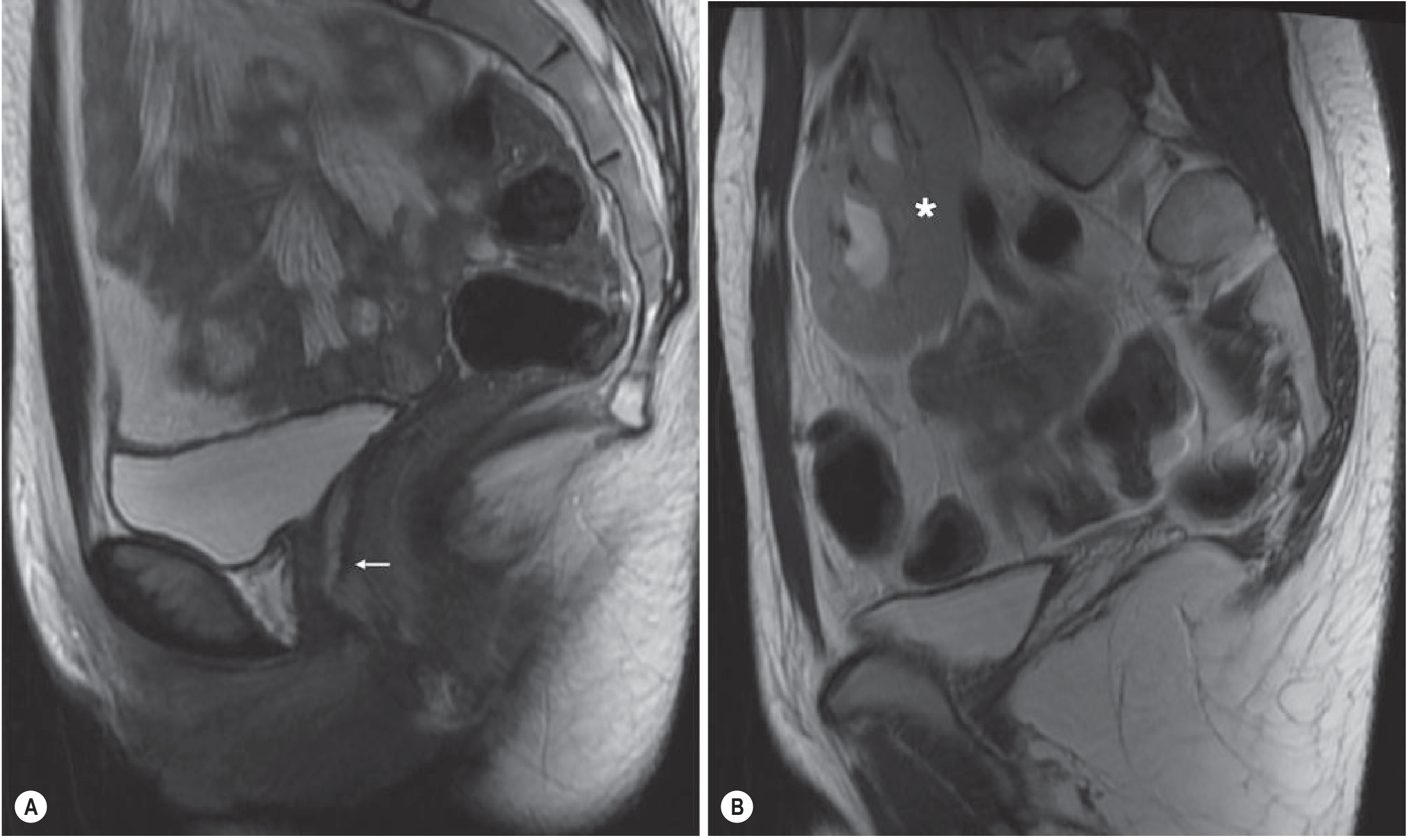
Fig. 35.6 - MRKH Syndrome: Sagittal T2-weighted MRI of the pelvis showing absent uterus and upper vagina (A) (white arrow) and pelvic kidney (B) (asterisk).
- Patients cannot carry a pregnancy; genetically related children are only possible via IVF and a gestational carrier.
- Associated with primary amenorrhoea, normal female karyotype (46,XX), and normal secondary sexual characteristics.
Class II - Unicornuate Uterus
Failure of one Müllerian duct to develop, resulting in a curved, elongated, banana-shaped uterus with tapering of the fundal segment off midline. Normal uterine zonal anatomy is preserved.
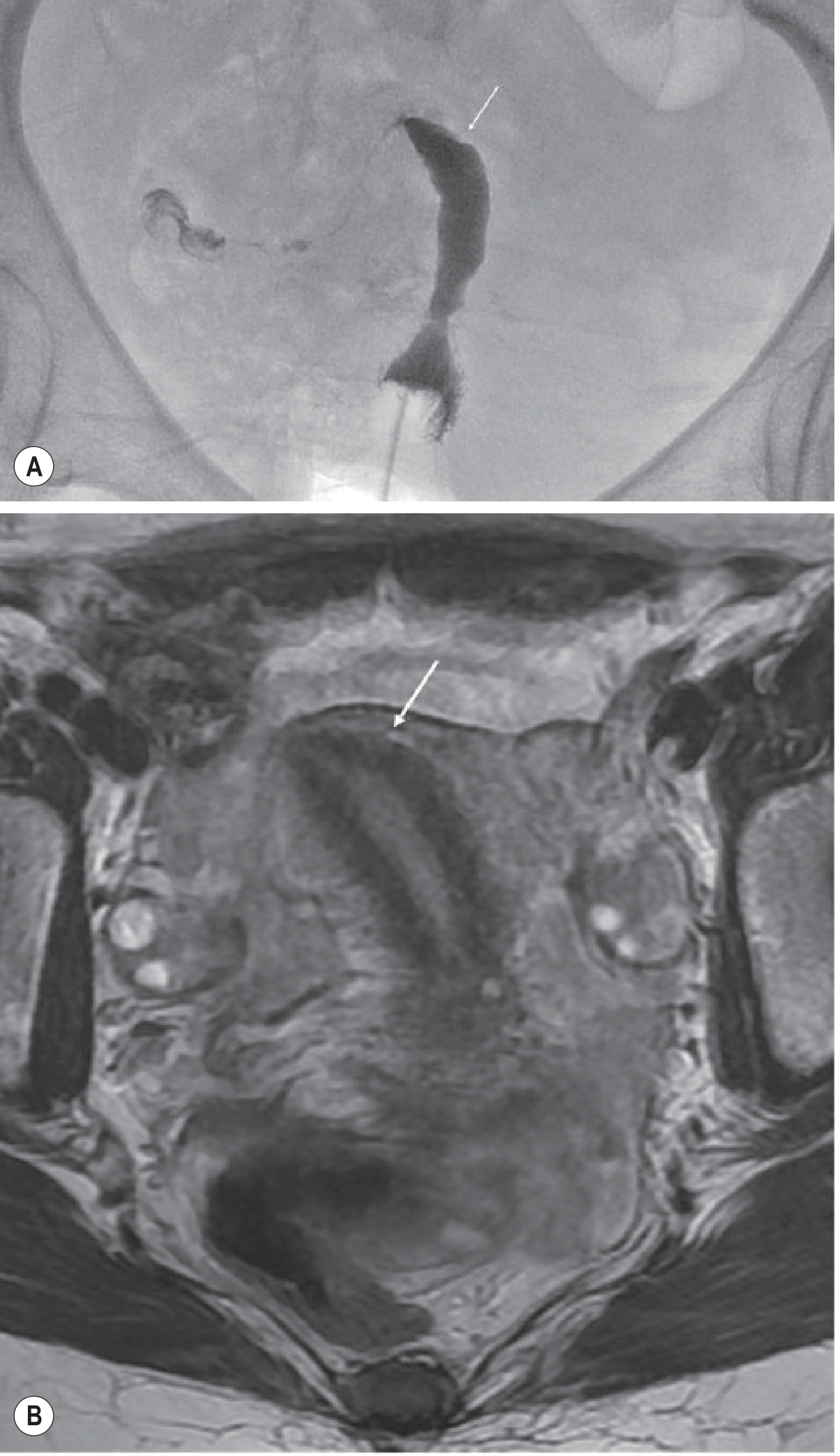
Fig. 35.7 - Unicornuate Uterus: (A) Hysterosalpingogram and (B) T2-weighted axial oblique MRI showing the 'banana-like' configuration (white arrow).
A rudimentary horn may be:
- Functional (non-communicating): accumulates blood → haematometra, increased risk of endometriosis
- Non-functional: no endometrium
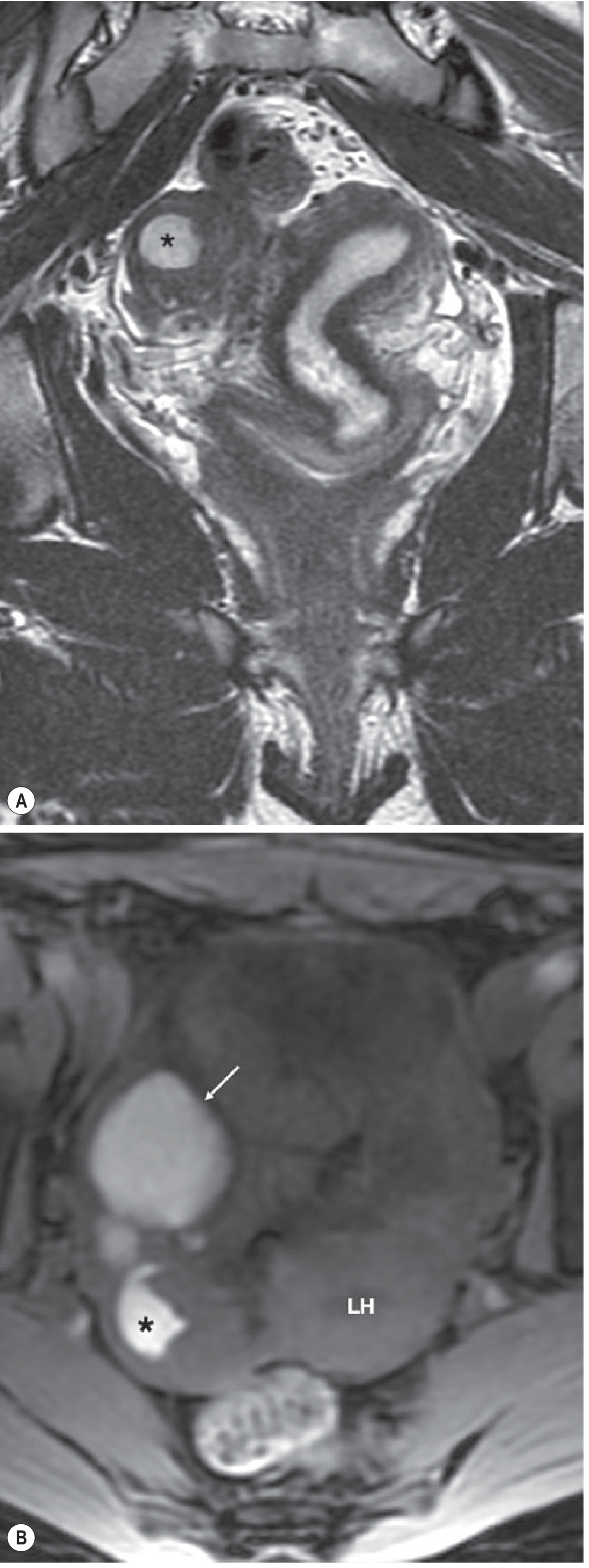
Fig. 35.8 - Unicornuate Uterus with Non-Communicating Functioning Rudimentary Horn: haematometra (asterisk) and right ovary endometrioma (white arrow). High signal on T1 fat-saturated images confirms blood products.
Clinical significance: Increased spontaneous abortion, obstetric complications, and infertility. Associated renal agenesis in up to 33% of cases. Rudimentary horns require surgical removal on diagnosis.
Class III - Uterus Didelphys
Complete non-fusion of the Müllerian ducts produces two separate, normal-sized uterine horns with two cervices. A longitudinal vaginal septum is present in 75% of cases.
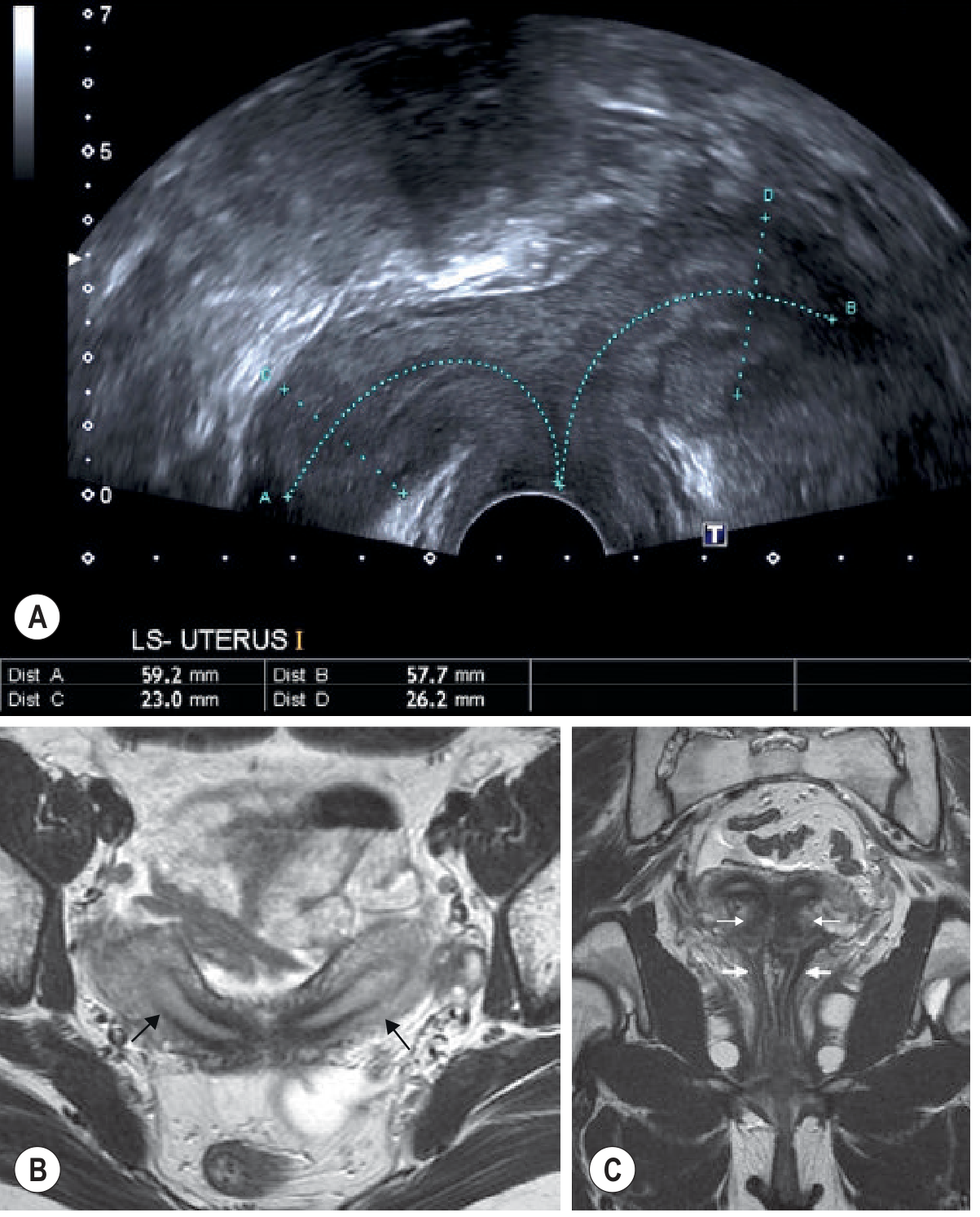
Fig. 35.9 - Uterus Didelphys: (A) Transverse US demonstrating two uterine cavities. (B) T2-weighted axial oblique and (C) coronal MRI demonstrating two separate, normal-sized uterine horns (black arrows), cervices (thin white arrows), and vaginas (thick white arrows).
- On coronal oblique T2, horns are widely separated with preservation of endometrial and myometrial widths
- Obstetric complications relate to the degree of non-fusion
- Key differentiator from septate uterus: requires MRI - didelphys shows two completely separate uterine structures
Class IV - Bicornuate Uterus
Incomplete fusion of the cephalad extent of the uterovaginal horns with resorption of the septum. The external fundal contour shows a myometrial cleft ≥1 cm, which differentiates it from the septate uterus.
On T2-weighted coronal images: two communicating uterine horns with a concave fundus, the intervening cleft demonstrates normal myometrial signal intensity on all sequences, and normal zonal anatomy is seen in each horn.
Key differentiator from septate uterus: the external uterine contour is concave with a cleft >1 cm (bicornuate) vs. convex/flat (septate).
Class V - Septate Uterus
The most common Müllerian duct abnormality. Results from incomplete resorption of the fibrous septum between the two uterine horns. The septum may be partial or complete (extending to the external cervical os).
This is the anomaly with the worst obstetric outcome of all Müllerian abnormalities, carrying the highest rates of miscarriage and preterm delivery.
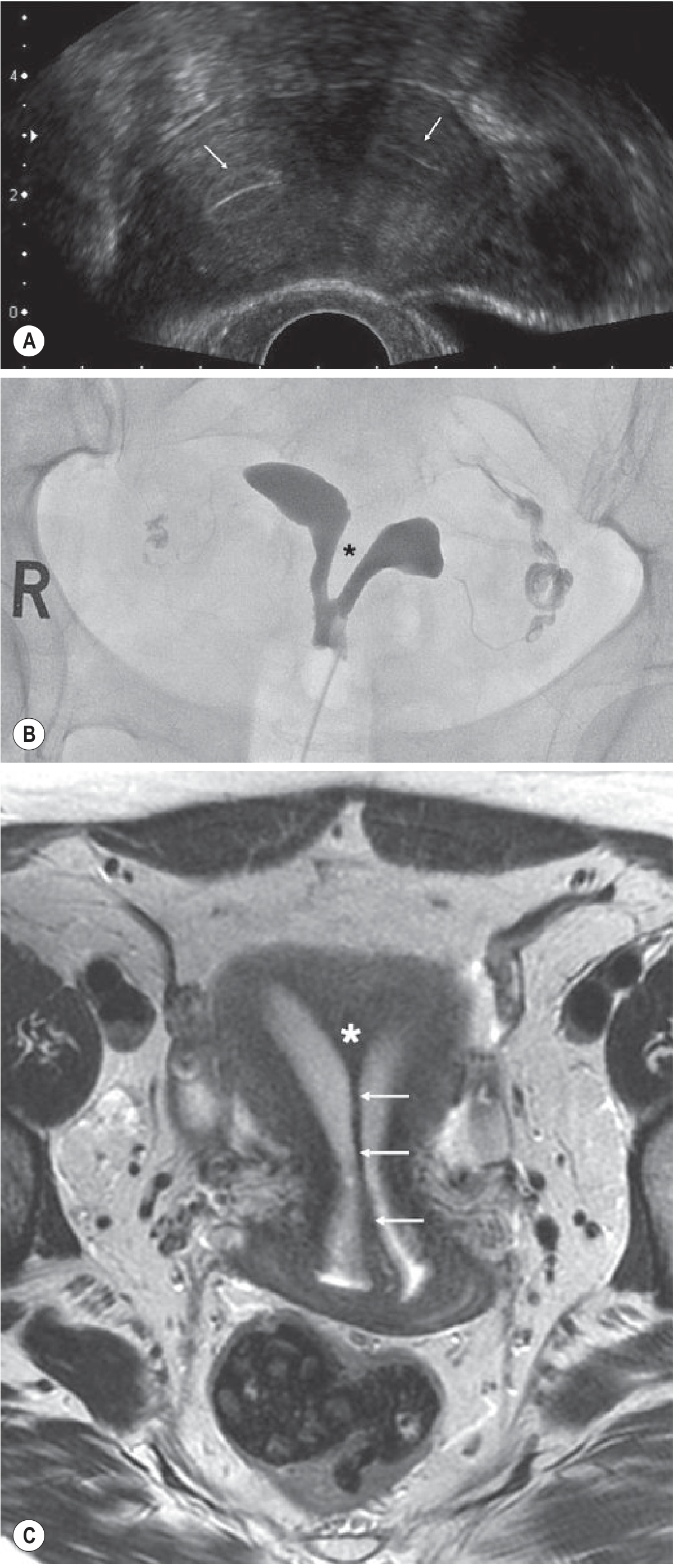
Fig. 35.11 - Septate Uterus: (A) US transverse showing two cavities (white arrows) separated by a thick muscle septum. (B) HSG demonstrating a thick muscle septum (asterisk). (C) Axial oblique T2 MRI clearly demonstrates the fibrous septum (white arrows) and muscular septum (asterisk).
- External contour: convex, flat, or concave (≤1 cm indentation) - unlike bicornuate
- Treatment: Hysteroscopic metroplasty (resection of septum) significantly reduces pregnancy loss rates
Class VI - Arcuate Uterus
The mildest congenital uterine anomaly. A broad, smooth concave indentation of the fundus of the uterine cavity (fundal dimple), with a normal external uterine contour.
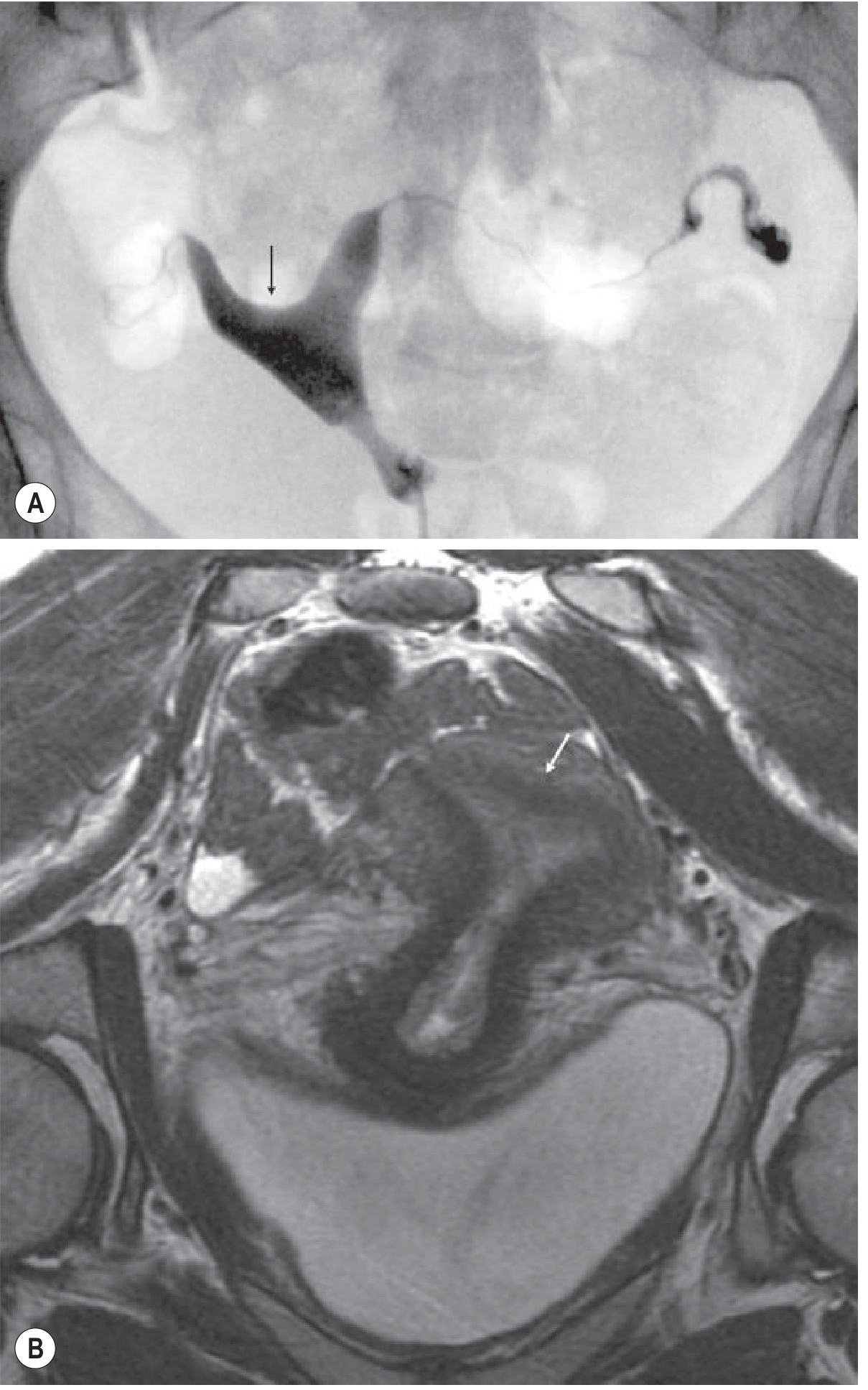
Fig. 35.12 - Arcuate Uterus: (A) Hysterosalpingogram showing the typical smooth, broad indentation of the fundal cavity (black arrow). (B) T2-weighted coronal MRI demonstrating a broad concave indentation of the endometrial cavity at the fundus (white arrow) but normal uterine outline.
- Live birth rates are generally comparable to women with normal uteri
- Typically considered a normal variant by many authorities
Class VII - Diethylstilbestrol (DES)-Related Anomaly
In utero exposure to DES (a synthetic oestrogen, banned 1971) produces characteristic uterine abnormalities:
- T-shaped uterine cavity (most common)
- Uterine hypoplasia
- Irregular constrictions
- Intraluminal filling defects
- Associated with higher rates of obstetric complications
Vaginal Anomalies
Vaginal Agenesis
Occurs in MRKH syndrome and androgen insufficiency syndrome (testicular feminization). The upper vagina is absent along with the uterus in MRKH.
Vaginal Septa (Transverse and Longitudinal)
Defects in vertical and lateral fusion of the Müllerian ducts produce septa that may:
- Cause obstruction of menstrual outflow
- Lead to haematocolpos (blood in vagina) or haematometrocolpos (blood in uterus + vagina)
- Present with cyclical pelvic pain and primary amenorrhoea
Imperforate hymen is the most common vaginal obstruction anomaly (prevalence 0.1%). On clinical exam: thin, bluish membrane that transilluminates - blood products visible behind it. Surgical treatment: excision of the membrane.
Transverse vaginal septum is thicker, appears pink in colour, and does not transilluminate. MRI shows low T2 signal fibrous tissue; vaginal dilatation with intermediate T2/high T1 fluid confirms haematometrocolpos. Treatment involves split skin graft or bowel interposition.
Longitudinal septum occurs in didelphys (75% of cases). In didelphys, one horn may have a perforated hymen with normal menstruation while the other has an imperforate hymen with haematocolpos.
Gartner Duct Cysts
Lateral vaginal wall cysts arising from persistent Wolffian (mesonephric) duct remnants. Usually asymptomatic but may cause pelvic pressure.
Summary Table: Buttram & Gibbons Classification
| Class | Anomaly | Mechanism | Key Feature | Obstetric Risk |
|---|---|---|---|---|
| I | Uterine agenesis/hypoplasia (MRKH) | Both Müllerian ducts fail | Absent uterus + vagina; intact ovaries | Cannot carry pregnancy |
| II | Unicornuate uterus | One duct fails | Banana-shaped, off-midline; rudimentary horn possible | High abortion rate |
| III | Uterus didelphys | Complete non-fusion | Two separate uteri + cervices; vaginal septum in 75% | Moderate |
| IV | Bicornuate uterus | Incomplete fusion (cephalad) | External cleft ≥1 cm; two horns | Moderate |
| V | Septate uterus | Failure of septum resorption | Worst obstetric outcome; normal external contour | Highest miscarriage rate |
| VI | Arcuate uterus | Minimal/mild resorption defect | Broad smooth fundal dimple; normal contour | Minimal/normal |
| VII | DES-related | In utero DES exposure | T-shaped cavity | Moderate |
Associated Conditions
- Renal anomalies (30%-50%): renal agenesis, horseshoe kidney, pelvic kidney - always image kidneys
- Endometriosis: particularly with obstructed functional rudimentary horn
- Haematometra/Haematometrocolpos: with any obstructive lesion
- Infertility: most strongly associated with Müllerian agenesis (Class I); other anomalies more strongly linked to pregnancy wastage than primary infertility
Sources: Grainger & Allison's Diagnostic Radiology, 7th Ed. (Chapter 35); Berek & Novak's Gynecology (Chapter 10); Robbins & Kumar Basic Pathology (Chapter 17)
This is a shared conversation. Sign in to Orris to start your own chat.