Ecg reading from basics
Reading File
Finding Sources
Searching the Web
ECG reading basics systematic approach 2024
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching Images
normal ECG waveform P wave QRS T wave labeled diagram
Loading Image
Loading Image
Loading Image
Reading File
Searching Images
12 lead ECG placement chest leads limb leads diagram
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive material from Goldman-Cecil Medicine and Harrison's to construct a thorough ECG basics guide. Let me compile this into a well-structured answer.
ECG Reading — From Basics
1. What Is an ECG?
An electrocardiogram (ECG) records the electrical activity of the heart from the body surface. Each deflection represents electrical events in cardiac muscle — it does not directly measure mechanical contraction, but the two are tightly coupled.
2. The Cardiac Conduction System (What Generates the ECG)
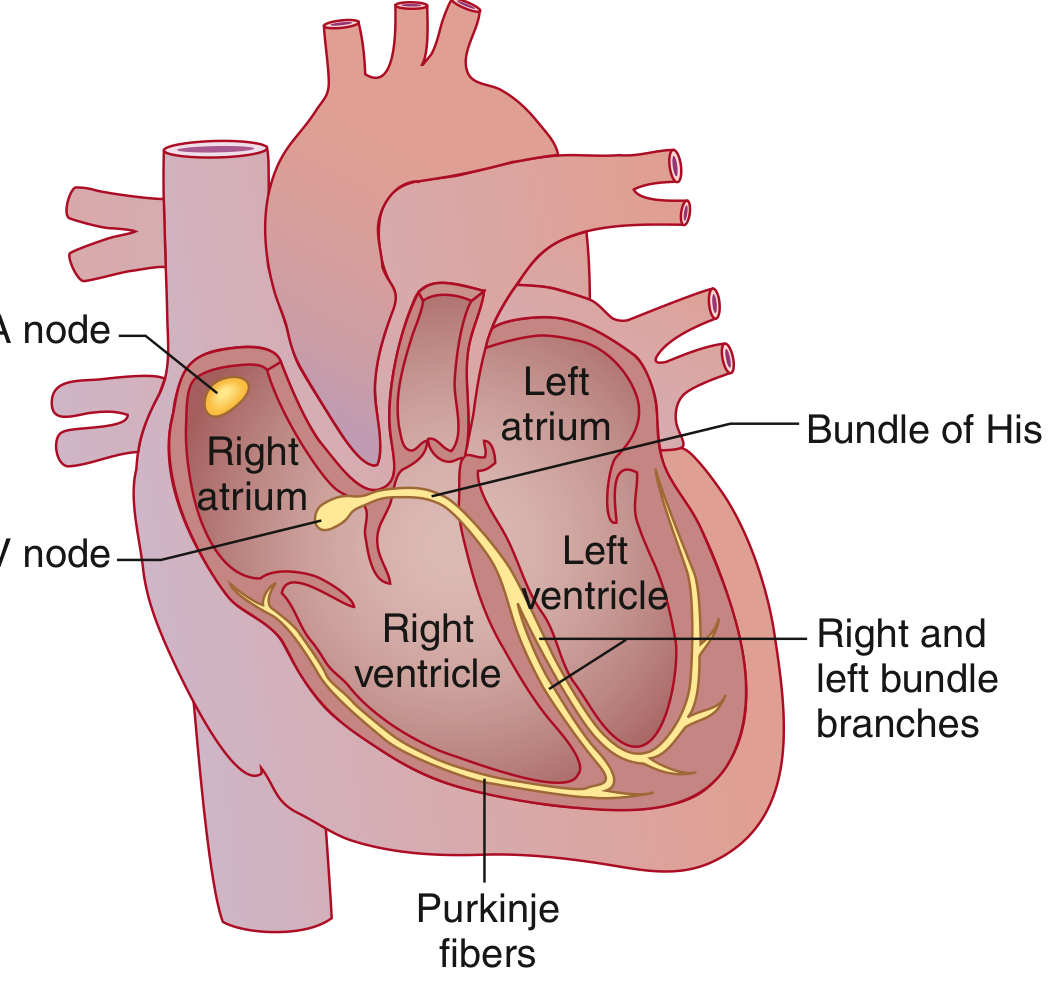
The electrical impulse follows this path:
| Structure | Function |
|---|---|
| SA node | Primary pacemaker; fires at 60–100 bpm spontaneously |
| Atrial muscle | Spreads depolarization through both atria (Bachmann bundle speeds it to left atrium) |
| AV node | Physiologic delay — "gatekeeper" between atria and ventricles |
| Bundle of His | Rapid conduction from AV node downward |
| Right & Left bundle branches | Left splits into anterior and posterior fascicles |
| Purkinje fibers | Spreads impulse rapidly to ventricular muscle |
3. The ECG Waves — What Each Represents
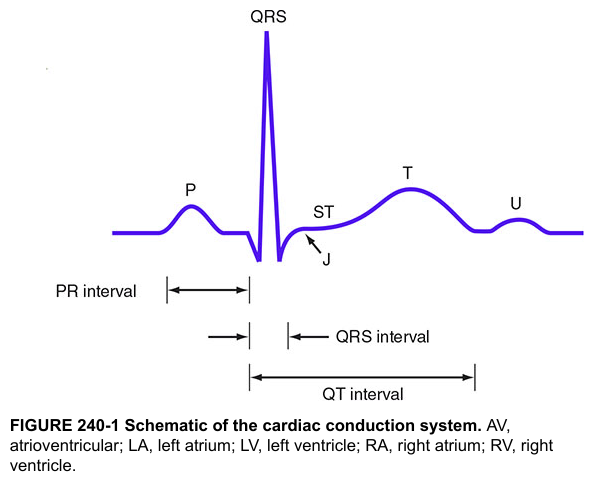
| Wave/Segment | Represents |
|---|---|
| P wave | Atrial muscular depolarization |
| PR segment | Conduction through AV node and His-Purkinje (isoelectric) |
| PR interval | Onset of P → onset of QRS; total atrial + AV nodal + His-Purkinje conduction |
| QRS complex | Ventricular muscular depolarization |
| J point | End of QRS / start of ST segment |
| ST segment | Plateau phase of ventricular action potential (isoelectric normally) |
| T wave | Ventricular repolarization |
| QT interval | Onset of QRS → end of T wave; total ventricular electrical systole |
| U wave | Purkinje fiber repolarization (small, not always visible) |
Key concept: Atrial repolarization is buried under the QRS complex and is not visible on the surface ECG.
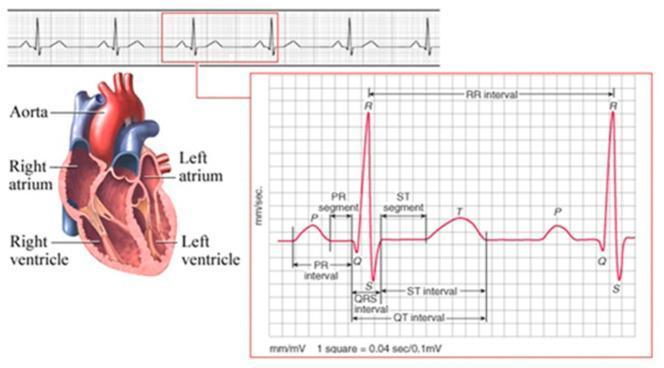
4. The ECG Paper and Calibration
Standard ECG paper runs at 25 mm/sec:
| Box | Time | Voltage |
|---|---|---|
| Small box (1 mm) | 0.04 sec (40 ms) | 0.1 mV |
| Large box (5 mm) | 0.2 sec (200 ms) | 0.5 mV |
| 2 large boxes (10 mm) | 0.4 sec | 1 mV (standard calibration) |
A standard ECG records 10 seconds of data across 12 simultaneous leads. Each lead group occupies 2.5 seconds.
5. Normal Intervals at a Glance
| Parameter | Normal Range |
|---|---|
| Heart rate | 60–100 bpm (some authorities: 50–90 bpm) |
| P wave duration | < 120 ms (< 3 small boxes) |
| PR interval | 90–200 ms (0.09–0.20 sec) |
| QRS duration | 75–110 ms (<3 small boxes) |
| QTc (Bazett) | Males: 390–450 ms; Females: 390–460 ms |
| QRS axis | −30° to +90° |
QTc formula (Bazett): QTc = QT ÷ √RR (RR in seconds)
6. The 12 Leads — What They View
10 electrodes produce 12 leads. The right leg electrode is a ground only.
Limb Leads (Frontal Plane)
| Lead | Comparison | View |
|---|---|---|
| I | Right arm (−) vs Left arm (+) | Lateral |
| II | Right arm (−) vs Left leg (+) | Inferior |
| III | Left arm (−) vs Left leg (+) | Inferior |
| aVR | Right arm vs (LA + LL) | Cavity — normally negative |
| aVL | Left arm vs (RA + LL) | High lateral |
| aVF | Left foot vs (RA + LA) | Inferior |
Precordial (Chest) Leads — Transverse Plane
| Lead | Position |
|---|---|
| V1 | 4th intercostal space, right sternal border |
| V2 | 4th intercostal space, left sternal border |
| V3 | Between V2 and V4 |
| V4 | 5th intercostal space, midclavicular line |
| V5 | Anterior axillary line, same level as V4 |
| V6 | Mid-axillary line, same level as V4 |
7. Heart Rate Calculation
Method 1 (regular rhythm): 300 ÷ number of large boxes between two R waves
| Large boxes between QRS | Heart Rate |
|---|---|
| 1 | 300 bpm |
| 2 | 150 bpm |
| 3 | 100 bpm |
| 4 | 75 bpm |
| 5 | 60 bpm |
| 6 | 50 bpm |
Method 2: Count beats in 10-second strip × 6
Method 3 (exact): HR = 60,000 ÷ RR interval (in ms)
8. QRS Axis
The frontal plane axis is the net direction of ventricular depolarization.
| Axis | Degrees | Significance |
|---|---|---|
| Normal | −30° to +90° | |
| Left axis deviation (LAD) | < −30° | LAHB, LVH, inferior MI |
| Right axis deviation (RAD) | > +90° | RVH, LPHB, normal in children |
| Extreme (NW) axis | < −90° or > +180° | Serious pathology |
Quick method: If QRS is predominantly positive in both I and II → normal axis.
To determine axis precisely: find the limb lead with the most isoelectric QRS — the axis is perpendicular to that lead.
9. The Systematic 14-Step Approach (Harrison's)
Harrison's recommends analyzing all 14 parameters in every ECG to avoid errors of omission:
- Standardization/calibration — confirm 1 mV = 10 mm; check paper speed
- Rhythm — sinus? Regular or irregular?
- Heart rate — fast, slow, or normal?
- PR interval — prolonged, short, or absent?
- QRS interval — narrow (<120 ms) or wide (≥120 ms)?
- QT/QTc interval — prolonged?
- QRS axis — normal, LAD, or RAD?
- P wave morphology — upright in I and II? Biphasic in V1?
- QRS voltages — high (LVH/RVH) or low?
- Precordial R-wave progression — R wave should grow V1→V6; transition at V3–V4
- Abnormal Q waves — pathological if ≥40 ms wide or ≥25% of R wave height
- ST segments — elevation or depression?
- T waves — upright in I, II, V3–V6; inverted T in aVR is normal
- U waves — prominent in hypokalemia, bradycardia; inverted U suggests ischemia
10. Key Patterns to Recognize (Basics)
Normal Sinus Rhythm
- Rate 60–100 bpm
- P wave before every QRS, QRS after every P
- PR interval 120–200 ms, consistent
- Narrow QRS (<120 ms)
- Upright P in leads I, II, aVF
P Wave Abnormalities
- P mitrale (broad, notched P, >120 ms): left atrial enlargement
- P pulmonale (tall, peaked P >2.5 mm in II): right atrial enlargement
- No P waves: atrial fibrillation (irregularly irregular QRS)
QRS Abnormalities
- Wide QRS (≥120 ms): bundle branch block, ventricular origin, paced rhythm, hyperkalemia
- RBBB pattern (V1): rSR' (M-shape) with secondary T inversion
- LBBB pattern (V6): broad notched R, absent septal q, T inversion
ST Segment
- Elevation: acute MI (STEMI), pericarditis, vasospasm — measure from J point
- Depression: ischemia, posterior MI, digoxin effect
QT Prolongation
- Risk of Torsades de Pointes (polymorphic VT)
- Causes: drugs (antiarrhythmics, antipsychotics, antibiotics), electrolyte abnormalities (↓K⁺, ↓Mg²⁺, ↓Ca²⁺), congenital channelopathies
11. Quick Reference: Regional Lead Groups
| Territory | Leads | Coronary Artery |
|---|---|---|
| Inferior | II, III, aVF | RCA (85%) |
| Lateral | I, aVL, V5, V6 | LCx |
| Anterior | V1–V4 | LAD |
| Septal | V1–V2 | LAD (septal perforators) |
| Posterior | Reciprocal ↓ST in V1–V3 | RCA or LCx |
12. Common Mistakes to Avoid
- Not checking calibration — if gain is halved, QRS looks small (pseudolowvoltage)
- Skipping leads — each lead views a different wall; check all 12
- Measuring QT in the wrong lead — use II, V5, or V6; take the longest
- Forgetting to compare with previous ECGs — subtle new changes matter
- Accepting the machine's interpretation without review — automated algorithms have significant error rates
Sources: Goldman-Cecil Medicine, 26th Ed. (GOLDMAN-CECIL MEDICINE, block 5); Harrison's Principles of Internal Medicine, 22nd Ed. (2025, block 27–28)
Create a detailed guide to abnormal ECG patterns
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
ST elevation STEMI ECG inferior anterior lateral wall myocardial infarction
Reading File
Searching Images
atrial fibrillation flutter ECG ventricular tachycardia fibrillation rhythm strip
Reading File
Loading Image
Loading Image
Searching Images
left bundle branch block LBBB right bundle branch block RBBB 12 lead ECG
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.