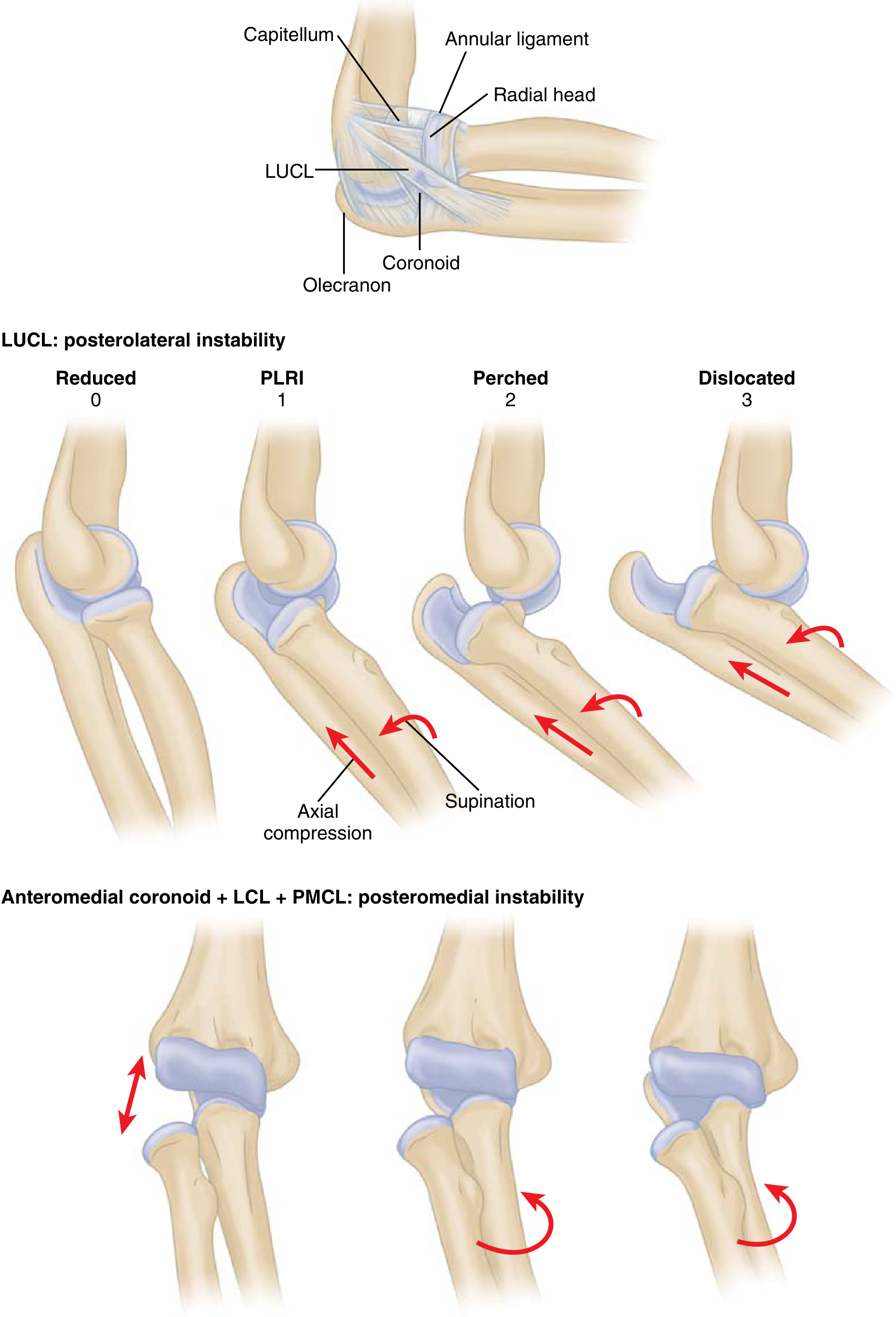
Types of elbow instability
Reading File
Finding Sources
Finding Sources
Searching the Web
types of elbow instability classification orthopedics
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Searching Images
elbow instability types posterolateral rotatory valgus varus diagram
I have comprehensive information from Rockwood & Green and Miller's Review. Here's a complete, well-organized answer:
Types of Elbow Instability
Overview
Elbow instability is most commonly classified by direction of displacement and the ligamentous structures disrupted. 80% of cases are posterolateral rotatory instability (PLRI); the remainder are posterior, anterior, medial, lateral, or divergent. — Miller's Review of Orthopaedics 9th Ed.
Classification by Direction
1. Posterolateral Rotatory Instability (PLRI) — Most Common
- Cause: Incompetence of the lateral ulnar collateral ligament (LUCL), which originates on the posterior lateral epicondyle and inserts on the crista supinatoris
- History: Often follows a previous elbow dislocation treated non-operatively
- Mechanism: The ulna rotates externally on the trochlea, causing posterior radial head subluxation
- Clinical test: Lateral pivot-shift test — reproduces instability with supination + axial compression + valgus loading as elbow is brought from full extension to ~40° flexion; radial head reduces with a palpable clunk as triceps becomes taut
- Note: Patient apprehension is common; examination under general anaesthesia or intra-articular local anaesthetic may be needed
- Imaging: MRI demonstrates LUCL pathology in ~50% of cases; elbow is more stable in forearm pronation
- Treatment: Reconstruction of the LUCL with tendon autograft for chronic instability
2. Varus Posteromedial Rotatory Instability (PMRI)
- Cause: Fracture of the anteromedial coronoid process (combined with LCL injury and posterior band of MCL disruption)
- Description: Increasingly recognized but poorly understood; the coronoid fracture leads to varus posteromedial rotatory instability if untreated
- Treatment: ORIF of coronoid with a buttress plate + assessment of MCL insertion
3. Valgus Instability
- Cause: Acute elbow trauma OR chronic repetitive loading with attenuation of the medial collateral ligament (MCL)
- Population: Classic in overhead-throwing athletes (baseball pitchers — "Tommy John" injury; javelin throwers)
- Biomechanics: Late cocking and acceleration phases of throwing place maximum stress on the MCL; FCU is the primary dynamic stabilizer, FDS secondary
- Clinical note: Surrounding muscle stabilizers can mask valgus instability in up to 50% of cases
- Imaging: MRI evaluates MCL integrity and flexor-pronator mass
- Associated pathology: Ulnar neuritis / cubital tunnel syndrome
- Treatment:
- Acute: Primary ligamentous repair or suture anchor reattachment (especially partial tears or avulsions with a "pop")
- Chronic: MCL reconstruction with tendon autograft (Tommy John surgery) — 75–80% return to sport at same level or better at 1 year
- Sequelae of untreated MCL insufficiency: Capitellar wear, posteromedial impingement, olecranon osteophyte formation, loose bodies → valgus overload syndrome
Classification by Complexity (Elbow Dislocation Model — O'Driscoll's Circle of Horii)
Simple elbow dislocation results from sequential, lateral-to-medial soft tissue disruption — the Circle of Horii:
| Stage | Name | Pathology |
|---|---|---|
| Stage 1 | Posteroexternal rotational instability | LCL partially or completely disrupted |
| Stage 2 | Perched ulna | Additional anterior/posterior disruption; radial head subluxed/dislocated, medial edge of ulna perched on trochlea; incomplete posterolateral dislocation |
| Stage 3A | Complete dislocation | Posterior soft tissue sleeve disrupted including posterior MCL (anterior MCL intact) |
| Stage 3B | Complete dislocation | Entire MCL disrupted — varus, valgus, AND rotatory instability all present after reduction; immobilize at 90° in cast |
| Stage 3C | Gross instability | Soft tissues stripped off entire distal humerus including flexor-pronator and common extensor origins; unstable even in flexion |
Complex (Fracture-Dislocation) Patterns
- Terrible Triad: Elbow dislocation + LCL injury + radial head fracture + coronoid fracture — the most unstable pattern
- Monteggia fracture-dislocation: Proximal-third ulnar fracture + radial head subluxation/dislocation; persistent proximal radioulnar instability may require annular ligament reconstruction
Summary Table
| Type | Key Ligament | Direction | Classic Setting |
|---|---|---|---|
| Posterolateral rotatory (PLRI) | LUCL | Posterolateral | Post-dislocation, iatrogenic |
| Varus posteromedial rotatory (PMRI) | LCL + posterior MCL | Posteromedial | Anteromedial coronoid fracture |
| Valgus | MCL (anterior bundle) | Medial | Throwing athletes |
| Simple dislocation (Stages 1–3) | LCL → MCL | Posterior | Traumatic fall on outstretched hand |
| Terrible triad | LCL + coronoid + radial head | Posterior | High-energy trauma |
Sources: Miller's Review of Orthopaedics 9th Ed., Rockwood and Green's Fractures in Adults 10th Ed. (2025)
This is a shared conversation. Sign in to Orris to start your own chat.