pOcus
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching the Web
POCUS point-of-care ultrasound overview 2024 2025
Reading File
Reading File
Searching Images
point of care ultrasound POCUS overview applications
Reading File
Reading File
Reading File
Excellent — I now have rich content from multiple authoritative textbooks. Let me compile a comprehensive overview.
Point-of-Care Ultrasound (POCUS) — Overview
What Is POCUS?
POCUS is a goal-directed, bedside ultrasound examination performed by trained clinicians to obtain real-time information for diagnosis, therapeutic decision-making, and procedural guidance. It is widely accepted as an extension of the physical examination, and its scope has expanded well beyond emergency medicine and critical care into anesthesiology, surgery, internal medicine, and primary care.
"POCUS represents a disruptive innovation that addresses immediate clinical needs in a cheaper, faster, and more accessible manner than consultative ultrasonography." — Barash's Clinical Anesthesia, 9e
POCUS vs. Consultative Ultrasonography
| Feature | POCUS | Consultative US (Radiology/Cardiology) |
|---|---|---|
| Scope | Limited, goal-directed | Comprehensive |
| Training required | Less extensive | Extensive |
| Imaging mode | Primarily 2D | 2D, 3D, Doppler, advanced techniques |
| Output | Yes/No answers to specific questions | Full diagnosis, severity grading, incidentals |
| Repeat-ability | Designed to be repeated at bedside | Formal appointment-based |
| Operator | Treating clinician | Dedicated sonographer + specialist |
Core Clinical Questions POCUS Can Answer
From the clinical data (Barash's Clinical Anesthesia, 9e):
| Question | Answer Rate |
|---|---|
| Is the patient stable? | 98% |
| Is the patient in shock? | 95% |
| Is the patient bleeding? | 94% |
| Is the patient in respiratory distress? | 93% |
| Is the patient in pain? | 92% |
| Is the patient in atrial fibrillation? | 91% |
Organ Systems Covered by POCUS
POCUS can be applied to virtually any organ system. The primary domains are:
1. 🫀 Cardiac — Focused Cardiac Ultrasound (FoCUS)
FoCUS addresses specific yes/no questions in the clinical context using simplified, qualitative imaging. The 5 standard views used in most FoCUS protocols:
- PLAX — Parasternal Long Axis
- PSAX — Parasternal Short Axis
- A4C — Apical 4-Chamber
- SC4 — Subcostal 4-Chamber
- SIVC — Subcostal Inferior Vena Cava
Key questions FoCUS answers:
- Is there significant LV systolic dysfunction? (walls thicken <30% during systole; LV chamber empties <50%)
- Is there RV dilation/dysfunction? (RVLV ratio >2/3 on A4C; TAPSE <17 mm)
- Is there pericardial effusion or tamponade? (RA collapse in systole; RV collapse in diastole)
- Is venous return adequate? (IVC collapsibility, end-systolic LV cavity obliteration)
If FoCUS reveals no pathology but cardiac disease is still clinically suspected, formal comprehensive echocardiography should be pursued.
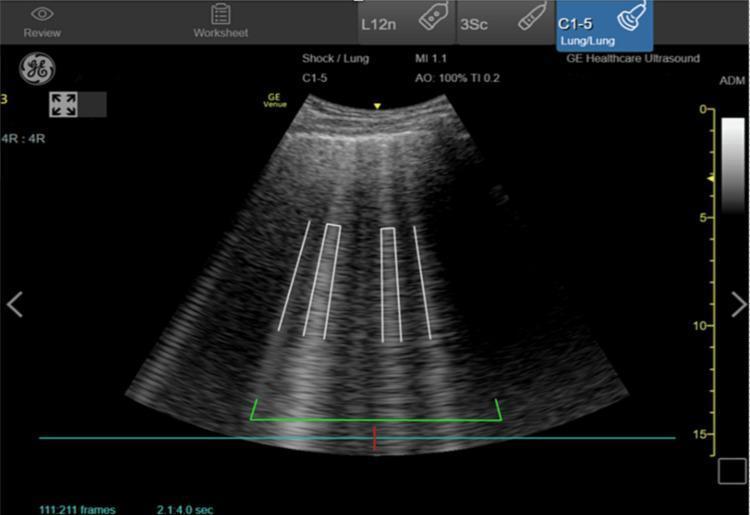
2. 🫁 Pulmonary / Lung Ultrasound
- Detection of pneumothorax (absent lung sliding, "barcode sign")
- Detection of pulmonary edema (B-lines — vertical laser-like artifacts from the pleural line)
- Pleural effusion (anechoic fluid above diaphragm)
- Comet-tail artifacts distinguish acute heart failure from COPD/asthma in undifferentiated dyspnea
3. 🫃 Abdominal — FAST Exam
- FAST (Focused Assessment with Sonography in Trauma): screens for free intraperitoneal fluid (blood) in trauma
- eFAST adds bilateral lung views to assess hemothorax/pneumothorax
- Can detect aortic aneurysm, hydronephrosis, free fluid
4. Other Applications
| Domain | Uses |
|---|---|
| Vascular | DVT assessment, IVC diameter/collapsibility for volume status |
| Gastric | Gastric contents/aspiration risk assessment before anesthesia |
| Ocular | Optic nerve sheath diameter (raised ICP), retinal detachment, CRAO |
| Procedural guidance | Central/peripheral IV lines, arterial lines, nerve blocks, thoracentesis, paracentesis, pericardiocentesis |
| Musculoskeletal | Rib fractures, joint effusions |
Key Advantages
- Portability — handheld devices made possible by military field use driving miniaturization
- Real-time imaging — immediate answers at the bedside
- Non-invasive — no radiation exposure
- Repeatable — track response to therapy over time
- Procedure safety — ultrasound guidance reduces complications for vascular access, regional blocks, and drainage procedures
Important Limitations
- Operator-dependent — image quality and interpretation tied to skill/knowledge
- Should not replace formal echocardiography when cardiology expertise is indicated
- Visual findings must be interpreted alongside the full clinical picture
- Obesity, subcutaneous emphysema, bowel gas, and dressings can degrade image quality
Training & Certification
Training requirements vary by specialty and procedure type. Several society-endorsed curricula exist (ASE, ASRA, ASA, ACEP, SCCM). Certification pathways in perioperative echocardiography (NBE) and critical care ultrasound are available and evolving globally. — Barash's Clinical Anesthesia, 9e; Miller's Anesthesia, 10e
Sources: Miller's Anesthesia 10e, Barash's Clinical Anesthesia 9e, Rosen's Emergency Medicine, Goldman-Cecil Medicine, Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.