Define coup and counter coup injury
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete breakdown of coup and counter-coup (contrecoup) injuries, drawn from multiple authoritative textbooks:
Coup and Contrecoup Brain Injuries
Definitions
- Coup injury: Brain damage (contusion) occurring at the site of impact - directly beneath the point where a blow was struck.
- Contrecoup injury: Brain damage occurring on the side opposite to the impact - the brain strikes the inner surface of the skull on the far side.
Both are forms of cerebral contusion. Their gross and microscopic appearances are indistinguishable; the distinction is made purely by identifying the point of impact.
Mechanism
The key driver is rapid acceleration-deceleration and the brain's inertia relative to the skull:
- When the skull is struck, CSF on the impact side is nearly incompressible, so the skull and brain initially move together.
- On the opposite side, the skull momentarily pulls away from the brain (due to inertia), creating a brief vacuum space in the cranial vault.
- When skull acceleration stops, this vacuum collapses and the brain is flung against the far inner skull surface, causing the contrecoup contusion.
- The moving brain may also be impaled on bony protuberances of the skull base (orbital ridges, sphenoid wing), compounding injury.
(Guyton & Hall, Medical Physiology)
Role of Head Mobility
| Head position at time of impact | Pattern of injury |
|---|---|
| Head immobile (e.g., struck while stationary) | Coup injury only |
| Head mobile (free to move) | Both coup and contrecoup, with contrecoup often predominating |
Direction of Impact and Resulting Pattern
| Direction of blow | Predominant lesion |
|---|---|
| Blow to the front | Mainly coup lesions |
| Blow to the back | Mainly contrecoup lesions (frontal/temporal lobes) |
| Blow to the side | Either or both coup and contrecoup lesions |
(Adams & Victor's Principles of Neurology, 12th ed.)
Common Locations
Regardless of where the head is struck, contusions (both coup and contrecoup) most frequently occur in:
- Frontal lobes - along the orbital ridges
- Temporal lobe poles - over the rough irregular floor of the middle cranial fossa
The occipital lobes are relatively spared because the inner occipital bone surface is smooth and the adjacent tentorium provides some protection.
Pathology of the Contusion
- Macroscopic: Wedge-shaped hemorrhagic lesions with the broad base at the cortical surface; gyral crests are most affected
- Acute: Edema, pericapillary hemorrhage, extending into cortex, white matter, and subarachnoid space
- Remote (healed): Yellow-orange discoloration called "plaque jaune" due to hemosiderin accumulation
(Robbins, Cotran & Kumar - Pathologic Basis of Disease)
Diagrammatic Illustration
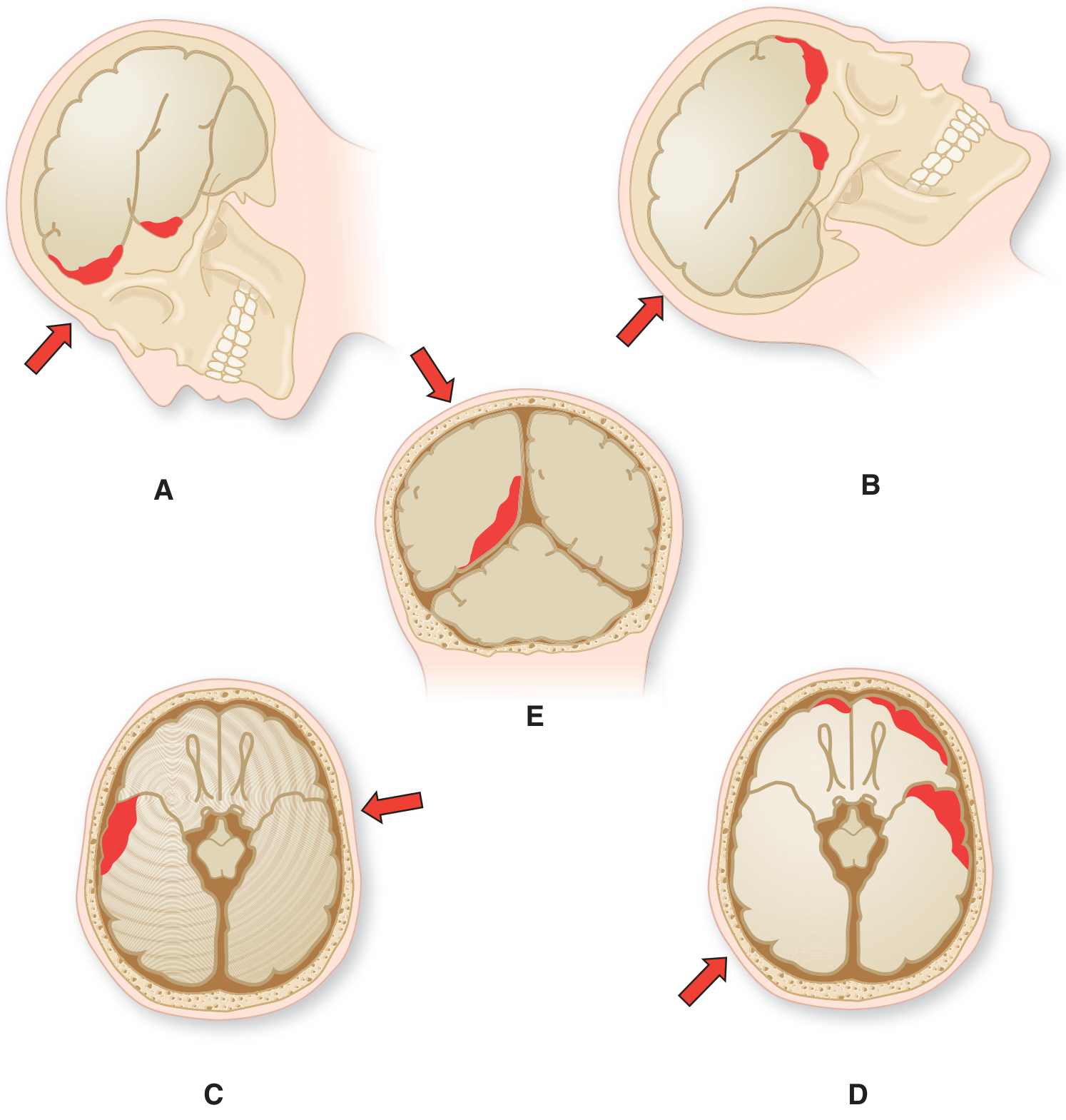
Fig. 34-4 from Adams & Victor's Principles of Neurology - Mechanisms of cerebral contusion. Red arrows = direction of impact force; dark red = contusion sites.
Gross Pathology (Acute Contusions)
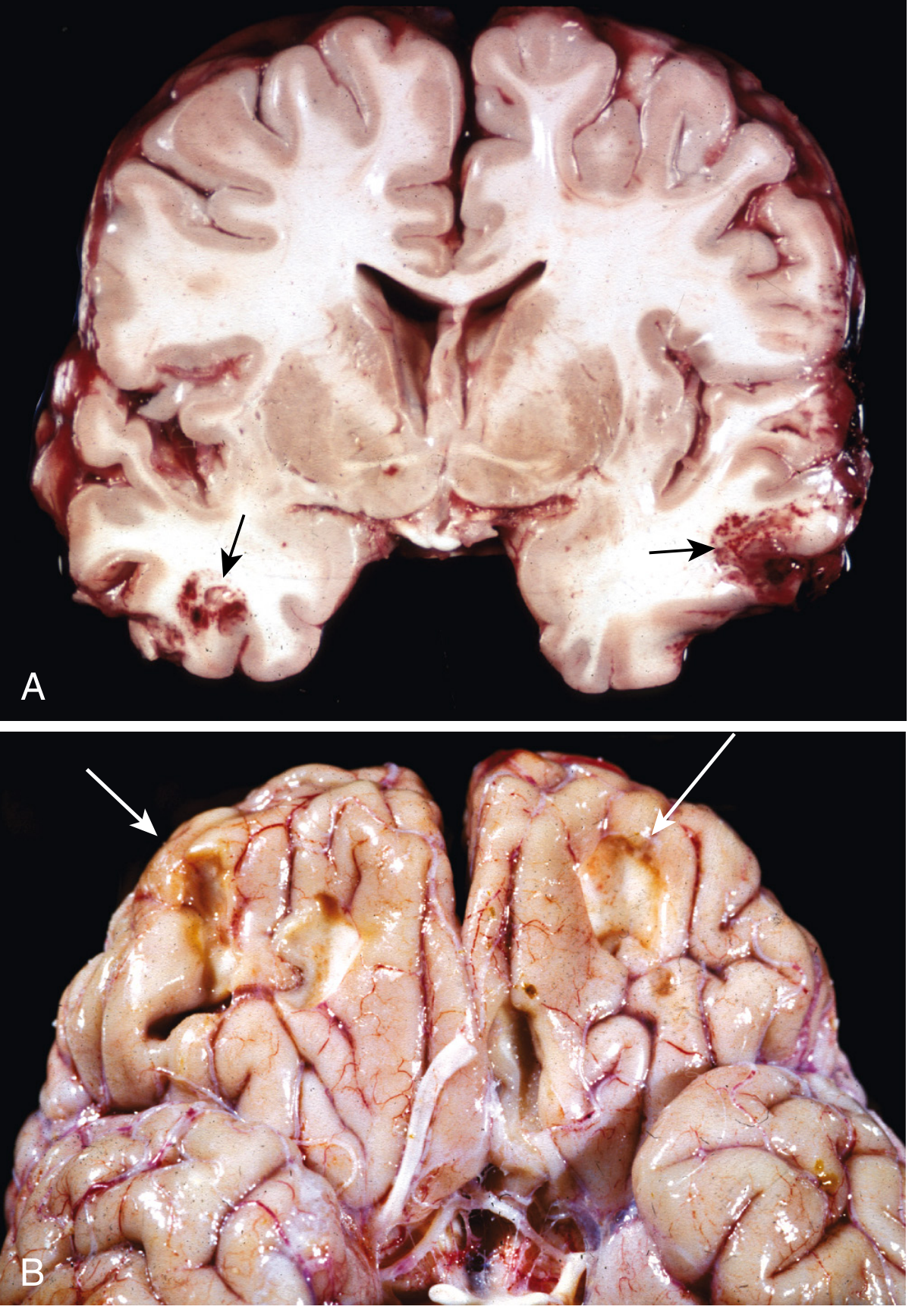
Acute contusions in both temporal lobes, with hemorrhage and tissue disruption (arrows) - Robbins & Cotran Pathologic Basis of Disease, Fig. 28.18
Without Direct Physical Impact
Coup-contrecoup injuries can also result from rapid acceleration/deceleration alone without any blow to the head - the brain bounces off one wall of the skull, then the opposite wall. Classic examples:
- Shaken baby syndrome
- High-speed vehicular accidents (whiplash-type forces)
Sources:
- Guyton and Hall Textbook of Medical Physiology - Cushioning Function of CSF
- Robbins, Cotran & Kumar - Pathologic Basis of Disease - Contusions and Lacerations, p. 1161
- Adams and Victor's Principles of Neurology, 12th ed. - Severe Head Injury, p. 896
- Robbins & Kumar Basic Pathology - Traumatic Parenchymal Injuries
This is a shared conversation. Sign in to Orris to start your own chat.