Tracheostomy
Reading File
Finding Sources
Searching PubMed
tracheostomy indications complications management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Tracheostomy
A comprehensive review based on Sabiston Textbook of Surgery, Current Surgical Therapy (14e), Scott-Brown's Otorhinolaryngology, and Fishman's Pulmonary Diseases.
Tracheal Anatomy
The trachea is a centrally located unpaired organ extending obliquely from the neck into the mediastinum. Average length: 11 ± 1 cm (males), 10 ± 1 cm (females). It contains 18-22 incomplete semicircular cartilaginous rings. The cricoid cartilage has the only complete cartilaginous ring and connects to the first tracheal ring inferiorly. Important sex difference in tracheal diameter: 2.5-2.7 cm (men) vs. 2.1-2.3 cm (women) - relevant for tube size selection.
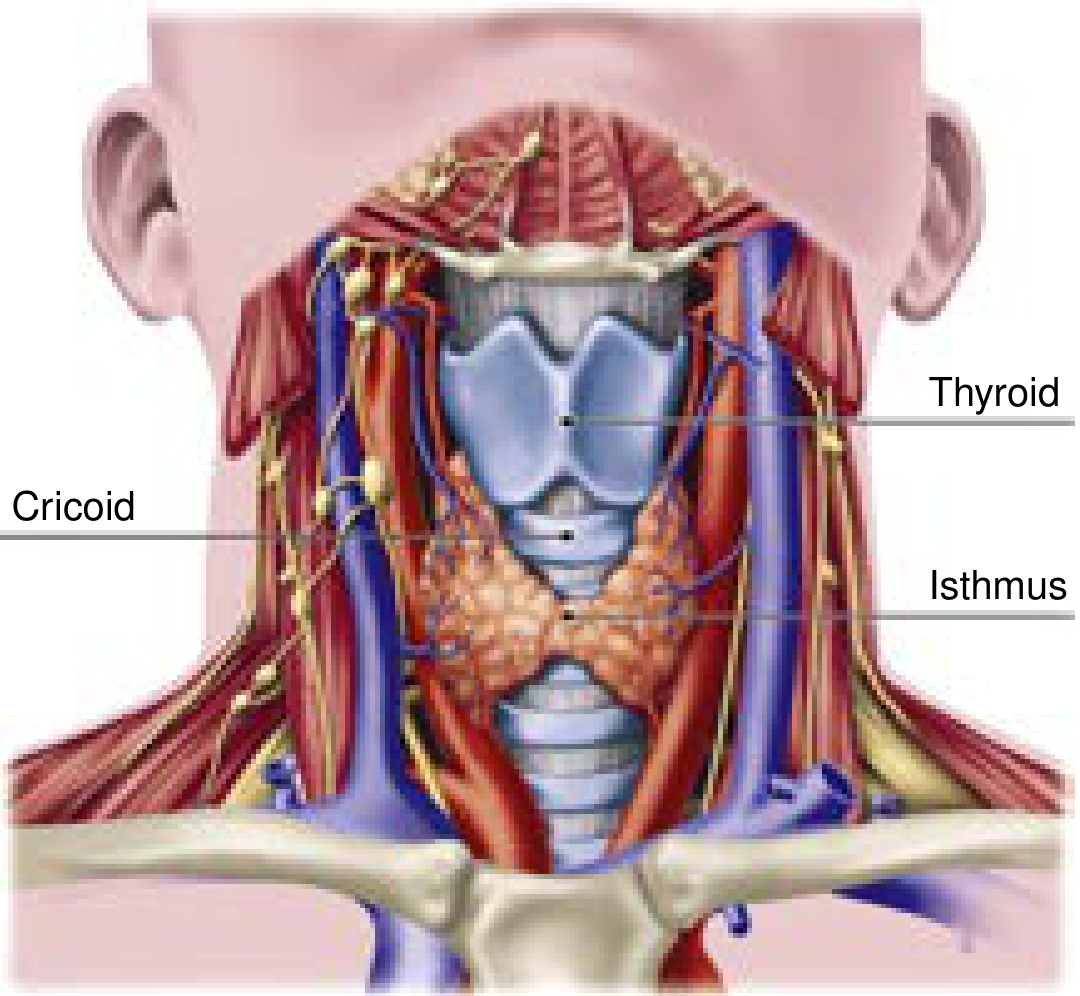
The thyroid isthmus overlies the 2nd-4th tracheal rings and must be managed (retracted or divided) during tracheostomy. The innominate artery crosses the trachea at approximately the 9th tracheal ring - a key landmark for avoiding tracheoinnominate fistula. (Current Surgical Therapy 14e)
Indications
Indications fall into three broad categories: (Sabiston, Table 47.1)
1. Upper airway obstruction
- Difficult airway / failed intubation
- Significant maxillofacial trauma
- Angioedema
- Upper airway tumors
2. Neurologic conditions preventing safe extubation
- Acute or progressive brain injury
- Spinal cord injury (including halo fixation)
- Severe agitation or delirium
- Prolonged altered mental status
3. Prolonged mechanical ventilation
- The single most common indication in the ICU
Additional specific indications:
- Need for ongoing bronchial toilet after weaning
- Laryngeal papillomatosis with severe airway disease (last resort)
- Pediatric croup with intubation failure or inadequate nursing facilities for nasotracheally intubated child
Contraindications (mostly relative)
| Contraindication | Notes |
|---|---|
| Recent anterior neck surgery (<7 days) | Relative |
| High ventilator settings (FiO₂ >50%, PEEP >10 cmH₂O) | Relative |
| Elevated intracranial pressure | Relative |
| Hemodynamic instability | Relative |
| Significant bleeding risk / coagulopathy | Relative |
| Local infection or malignancy at proposed site | Relative |
| Predicted early mortality | Relative |
Most contraindications are temporary. Predicted early mortality is perhaps the strongest reason to defer.
Advantages of Tracheostomy Over Prolonged Translaryngeal Intubation
(Scott-Brown's, Vol 1)
- Reduced sedation needs (no glottic stimulation)
- Reduced airway resistance and work of breathing
- Improved mouth care
- Reduced dead space (less significant than previously thought)
- Ongoing bronchial toilet after weaning
Timing
Timing remains controversial. Evidence summary (Sabiston/Scott-Brown's):
- Most studies show no mortality difference between early vs. late tracheostomy
- Early tracheostomy (≤7 days): associated with shorter ICU stay and fewer ventilator days in some trials
- The TracMan trial (UK, >900 patients across 72 ICUs): early (<4 days) vs. late (>10 days) - no mortality difference at 30 days to 2 years. Notably, >50% of those randomized to late tracheostomy never required one (liberated from MV or discharged)
- A medical ICU RCT: tracheostomy at 48 hrs vs. 14-16 days showed reduced mortality (32% vs. 62%), less pneumonia (5% vs. 25%), fewer accidental extubations - but this finding has not been widely replicated
- COVID-19 context: tracheostomy after 10-14 days of MV is associated with lower duration of ventilation and ICU stay without increased mortality
Methods
Percutaneous Dilatational Tracheostomy (PDT)
First described by Ciaglia in 1985. The most widely used method for elective tracheostomy in critically ill adults.
Technique (Seldinger-based):
- Partially withdraw the ETT under GA and neuromuscular blockade
- Insert needle between 2nd and 3rd tracheal rings (ideally)
- Pass guidewire, then dilate with a serial dilator, graduated dilator, or blunt forceps
- Place tracheostomy tube over wire under bronchoscopic guidance
Advantages over surgical:
- Can be done at the bedside (no OR time needed)
- More cost-effective
- Less wound infection
- Periprocedural mortality <0.1-0.2%
- Major complication rate ~0.15% (series of >3000 consecutive procedures)
Surgical (Open) Tracheostomy
Preferred when:
- Obesity (need for appropriate kit)
- Anatomical variance (previous neck surgery, goitre)
- Coagulopathy or bleeding diathesis
- Pediatric patients
- Emergency situations
Technique:
- Horizontal skin incision at level of 2nd-3rd tracheal rings
- Vertical midline division of strap muscles
- Thyroid isthmus retracted superiorly or divided/ligated
- Horizontal or vertical incision in anterior tracheal wall (between 2nd-3rd rings)
- Tracheostomy tube placed under direct visualization; secured with strap (one finger should fit between strap and skin); neck plate sutured or stapled
Comparison: PDT vs. Surgical Tracheostomy
Meta-analyses generally show equivalence. PDT is associated with:
- Fewer wound infections
- Less clinically relevant bleeding
- Tracheal ring fractures and posterior wall injuries are rare with surgical approach (direct visualization)
- No significant difference in overall mortality
Tracheostomy Tube Types
| Jackson Size | Inner diameter with inner cannula | Inner diameter without inner cannula | Outer diameter |
|---|---|---|---|
| 4 | 5.0 mm | 6.7 mm | 9.4 mm |
| 6 | 6.4 mm | 8.1 mm | 10.8 mm |
| 8 | 7.6 mm | 9.1 mm | 12.2 mm |
| 10 | 8.9 mm | 10.7 mm | 13.8 mm |
Key tube features: cuffed vs. uncuffed, fenestrated (for speaking), inner cannula (for cleaning), adjustable flange (for obese or anatomically unusual necks).
Complications
Early (within 1 week)
| Complication | Notes |
|---|---|
| Accidental decannulation | Most common catastrophic event; in pediatrics, <7 days carries highest risk as tract immature |
| Tube obstruction | Most frequent tracheostomy emergency; usually manageable with suctioning |
| Peristomal bleeding | Often from anterior jugular veins or thyroid isthmus; usually controlled with pressure, tightening collar, Surgicel, or lidocaine-epinephrine injection |
| Posterior tracheal/esophageal injury | Laceration through back wall during PDT |
| False tract / paratracheal insertion | Can cause mediastinal placement |
| Pneumothorax | Rare (~0.85%); post-procedure CXR mandatory |
| Subcutaneous emphysema / pneumomediastinum | ~1.4% |
| Infection | Wound infection |
| Apnea | Particularly in children |
| Airway fire | Risk with electrocautery (surgical approach); use lowest tolerable FiO₂ |
Late (after 1 week)
| Complication | Notes |
|---|---|
| Tracheal stenosis | Subglottic, stomal, or cuff level; clinically significant only with >75% luminal reduction; stridor appears when lumen <5 mm. Overall incidence markedly reduced with high-volume, low-pressure cuffs |
| Tracheoinnominate fistula (TIF) | Most feared; <1% overall; occurs 48 hr to 14 days post-op. Mortality ~85%. Prevention: place tube above 3rd ring (2nd-3rd preferred), keep cuff pressure <25 mmHg |
| Tracheomalacia | Cartilage erosion |
| Tracheoesophageal fistula | Presents with postoperative dysphagia/aspiration |
| Granulation tissue | Particularly in children |
| Suprastomal collapse | In pediatric patients |
| Tracheocutaneous fistula | After prolonged cannulation |
| Aspiration | Tracheostomy tethers larynx; decreases cough reflex by limiting subglottic pressure |
| Aphonia / speech delay | Particularly in children |
Key figure from Fishman's: In a survey of 478 otolaryngologists, 66% of catastrophic events involved airway loss or bleeding. Of bleeding events, >90% were TIF. Accidental decannulation was far more common than loss of airway during planned tube change. Approximately 1000 catastrophic events per year estimated, with ~50% causing death or permanent morbidity. The overwhelming majority occurred >7 days after tracheostomy.
Management of Specific Complications
Tracheoinnominate Fistula
- Do not deflate the cuff until in OR with appropriate personnel
- If stable: CT angiography of neck with contrast to assess anatomy
- If actively hemorrhaging: replace tracheostomy tube with orotracheal ETT (cuff distal to bleeding), apply digital pressure anteriorly through the stoma, take immediately to OR for surgical repair
Accidental Decannulation
- Reintroduce tube in a controlled manner
- If tract is immature (<7 days): use introducer needle and guidewire to avoid false passage
- If difficult: re-intubate transorally with ETT cuff distal to stoma first to secure airway before tube reinsertion
Tube Obstruction
- Suction
- Inner cannula cleaning or replacement
- Emergency reintubation if severe
Decannulation
A stepwise process:
- Downsize tracheostomy tube progressively
- Trial of tube capping (patient must tolerate breathing around/above the tube)
- Remove tube when patient tolerates capping; tape/cover stoma
- Instruct patient on stoma occlusion during speech and coughing while stoma heals
- Most stomata close spontaneously; tracheocutaneous fistula requiring repair is uncommon
In pediatric patients, decannulation requires assessment of:
- Adequate natural airway above tracheostomy
- Ability to protect airway from aspiration
- Adequate cough and secretion management
Special Situations
COVID-19 and Aerosol-Generating Procedures: Tracheostomy is an aerosol-generating procedure requiring airborne/droplet precautions. Negative-pressure rooms, full PPE, minimal staff, and avoidance of circuit disconnects are recommended.
ECMO patients: Tracheostomy can be performed safely at the bedside. Complication rates are higher (almost entirely bleeding-related); no significant difference between PDT and open technique.
Pediatric tracheostomy: Higher risks than adult; tube obstruction and accidental decannulation are the leading causes of tracheostomy-related death (0-3.6% tube-related mortality). Maturation sutures and stay sutures are recommended. Papillomatosis is a specific pediatric concern - tracheostomy may promote tracheobronchial seeding and is a last resort.
Sources: Sabiston Textbook of Surgery, p. 960-961 | Current Surgical Therapy 14e, p. 1591-1594 | Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1 & 2 | Fishman's Pulmonary Diseases and Disorders, p. 2587-2588
This is a shared conversation. Sign in to Orris to start your own chat.