Pelvic diaphragm
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have comprehensive information from Gray's Anatomy for Students and the Thieme Atlas. Here is a thorough, well-illustrated account of the pelvic diaphragm.
Pelvic Diaphragm
Overview
The pelvic diaphragm is the muscular component of the pelvic floor. It is shaped like a bowl or funnel and is attached superiorly to the pelvic walls. Together with the perineal membrane and the deep perineal muscles (anteriorly), it forms the complete pelvic floor, separating the pelvic cavity above from the perineum below.
The pelvic diaphragm sits at the upper level of a three-tiered arrangement of the pelvic floor:
- Upper level: pelvic diaphragm
- Middle level: deep urogenital muscles (deep perineal pouch)
- Lower level: sphincters and erectile muscles
Composition
The pelvic diaphragm is formed by two paired muscles and their fasciae:
- Levator ani (the major muscle)
- Coccygeus
Both muscles are covered by the superior fascia (above) and inferior fascia (below) of the pelvic diaphragm.
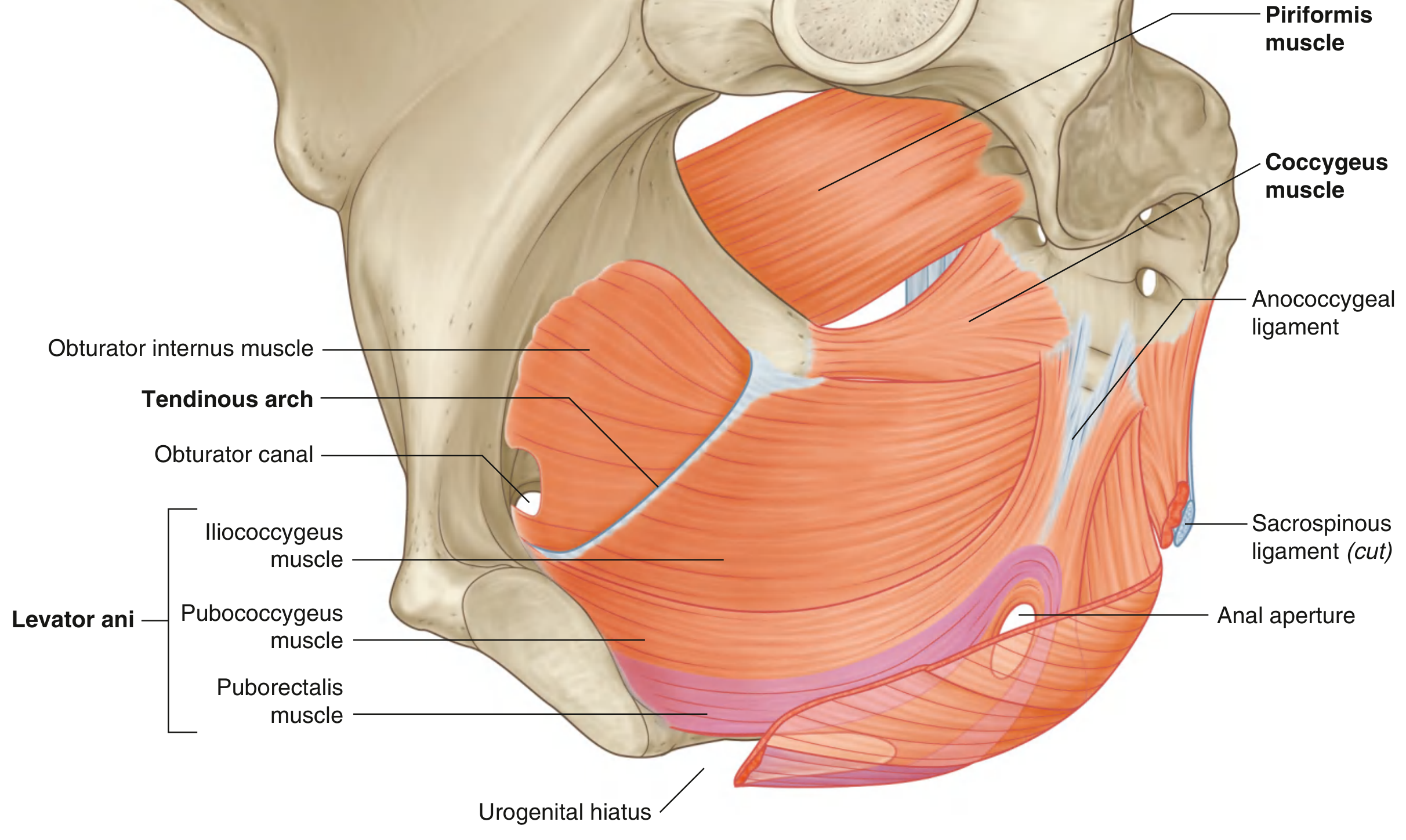
Levator Ani
The levator ani is the principal muscle of the pelvic diaphragm. The two muscles originate from each side of the pelvic wall, course medially and inferiorly, and join together in the midline.
Origin (line of attachment to pelvic wall)
- Posterior aspect of the body of the pubic bone
- The tendinous arch - a linear thickening of the fascia covering the obturator internus muscle
- Spine of the ischium
Insertion / Midline attachments
- Posterior to the vagina (in women) and around the anal aperture (both sexes)
- The anococcygeal ligament (anococcygeal body) - where muscles join as a raphe and attach to the coccyx
- Anteriorly, there is a U-shaped gap - the urogenital hiatus - which allows passage of the urethra (in both sexes) and vagina (in women)
Three Parts of Levator Ani
| Part | Origin | Insertion | Key Feature |
|---|---|---|---|
| Pubococcygeus | Body of pubis (lateral) | Anococcygeal ligament, coccyx | Further subdivided into puboprostaticus, pubovaginalis, puboanalis |
| Puborectalis | Superior pubic ramus (both sides of symphysis) | Loop around anorectal junction, interwoven with external anal sphincter | Forms a muscular sling; maintains the perineal flexure (anorectal angle) |
| Iliococcygeus | Tendinous arch of obturator internus fascia | Iliococcygeal raphe, anococcygeal ligament, coccyx | Joins its partner to form the levator plate |
Innervation
- Direct branches from the anterior ramus of S4
- Inferior rectal branch of the pudendal nerve (S2-S4)
Functions of Levator Ani
- Supports pelvic viscera
- Maintains the anorectal angle (continence mechanism)
- Reinforces the external anal sphincter
- In women, acts as a vaginal sphincter (pubovaginalis)
- Raises the pelvic floor during increased intra-abdominal pressure (coughing, sneezing)
Coccygeus
| Feature | Detail |
|---|---|
| Origin | Ischial spine and pelvic surface of the sacrospinous ligament |
| Insertion | Lateral margin of coccyx and adjacent border of sacrum |
| Innervation | Branches from anterior rami of S4 and S5 |
| Function | Supports pelvic viscera; pulls coccyx forward after defecation |
The coccygeus lies on the posterior part of the pelvic floor, posterior to the levator ani. Note: it is often considered the pelvic equivalent of the sacrospinous ligament, which lies on its deep (inferior) surface.
Relation to Sciatic Foramina
The circular line of attachment of the pelvic diaphragm to the pelvic wall passes between the greater and lesser sciatic foramina on each side:
- Greater sciatic foramen - lies above the pelvic floor; connects the pelvic cavity to the gluteal region
- Lesser sciatic foramen - lies below the pelvic floor; connects the gluteal region to the perineum
Urogenital Hiatus
The anterior part of the levator ani muscles are separated by a U-shaped defect, the urogenital hiatus. Its margins merge with the visceral walls and with the deep perineal muscles below. It transmits:
- Urethra (in both males and females)
- Vagina (in females only)
Fasciae of the Pelvic Diaphragm
The muscles are enclosed between two fascial layers:
- Superior fascia of the pelvic diaphragm - forms the floor of the pelvic cavity proper
- Inferior fascia of the pelvic diaphragm - forms the roof of the ischiorectal (ischioanal) fossa laterally, and the roof of the deep perineal pouch anteriorly
Clinical Relevance
- Pelvic organ prolapse - weakening of the levator ani (especially pubococcygeus) allows the bladder, uterus, or rectum to descend through the urogenital hiatus
- Stress urinary incontinence - impaired closure of the urogenital hiatus and loss of urethrovesical angle support
- Perineal flexure - the anorectal angle maintained by puborectalis is critical for fecal continence; loss (as in pudendal nerve injury) leads to fecal incontinence
- Obstetric injury - levator ani tears and avulsion from the pubic bone are common in vaginal delivery, especially with instrumented delivery
Sources: Gray's Anatomy for Students, pp. 529-531 | Thieme Atlas of General Anatomy and Musculoskeletal System, pp. 163, 183, 203
Little short
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive multi-textbook content. Here is the full, expanded account:
Pelvic Diaphragm - Comprehensive Anatomy
Definition and Overview
The pelvic diaphragm is a funnel-shaped (bowl-shaped) fibromuscular partition that forms the primary supporting structure for the pelvic contents. It is the muscular component of the pelvic floor and separates the pelvic cavity above from the perineum below.
The pelvic floor as a whole is formed by three layers:
- Upper level - the pelvic diaphragm (levator ani + coccygeus + their fasciae)
- Middle level - deep urogenital muscles (deep perineal pouch)
- Lower level - sphincters and erectile muscles of the urogenital and intestinal tract
The pelvic diaphragm's circular line of attachment to the pelvic wall passes on each side between the greater sciatic foramen (above the floor, communicating pelvic cavity with the gluteal region) and the lesser sciatic foramen (below the floor, communicating the gluteal region with the perineum). Its inferior surface forms the ceiling of the ischiorectal (ischioanal) fossa.
Composition
The pelvic diaphragm consists of:
- Levator ani (the principal and largest component)
- Coccygeus (the posterior, smaller component)
- Superior fascia of the pelvic diaphragm - floor of the pelvic cavity proper
- Inferior fascia of the pelvic diaphragm - roof of the ischiorectal fossa and deep perineal pouch
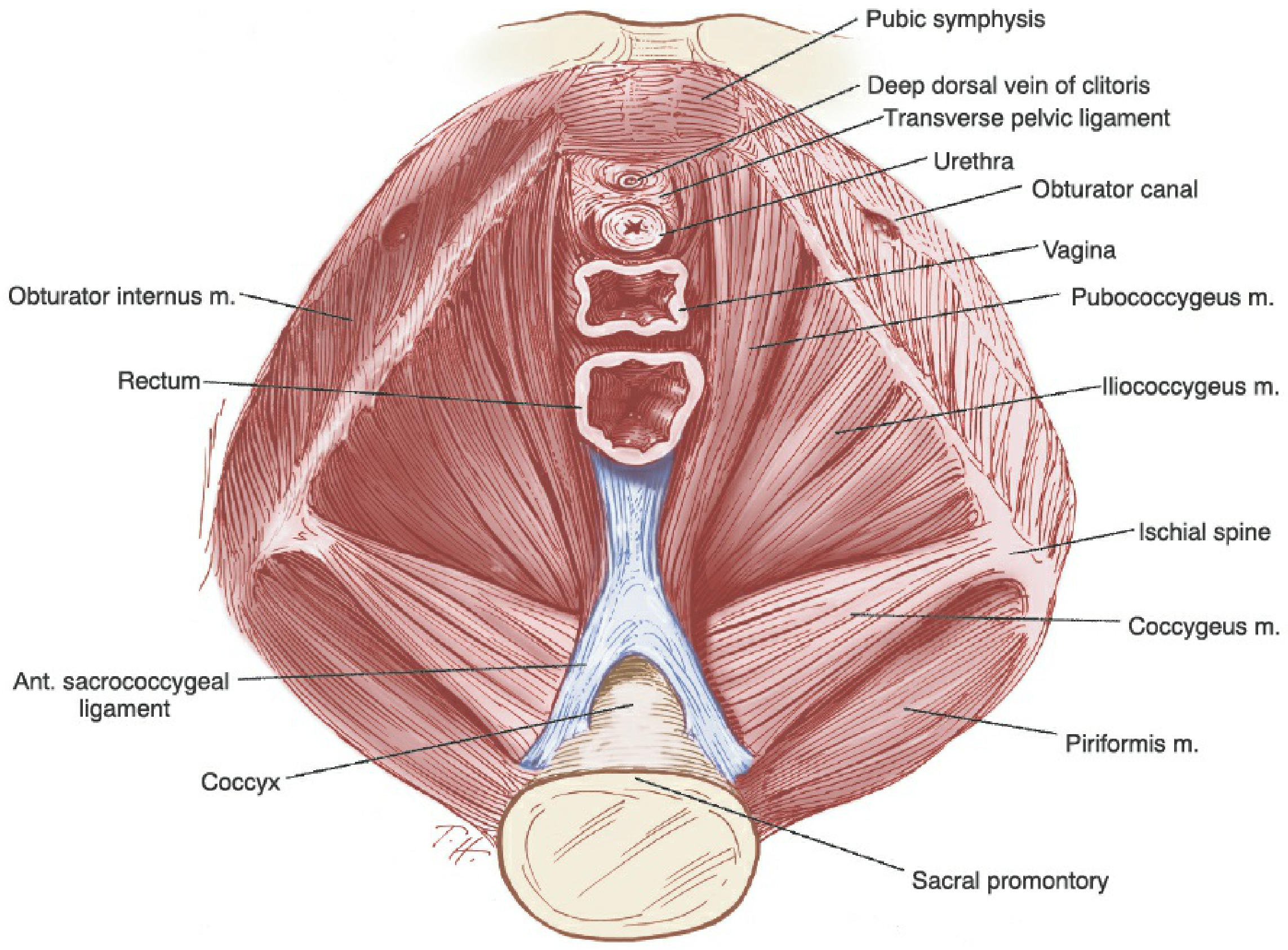
Levator Ani
The levator ani is a broad, thin, curved sheet of striated muscle stretching from the pubis anteriorly to the coccyx posteriorly, arching across the entire pelvic outlet from one side to the other. It is perforated by the urethra, vagina, and anal canal.
Origin
The muscles originate along a continuous line from the pelvic wall:
- Posterior aspect of the body of the pubic bone
- The arcus tendineus levator ani (ATLA) - a thickened condensation of the obturator internus fascia running as a tendinous arch from the back of the pubic body to the ischial spine
- Ischial spine
The ATLA is an important lateral landmark used during vaginal suspension procedures.
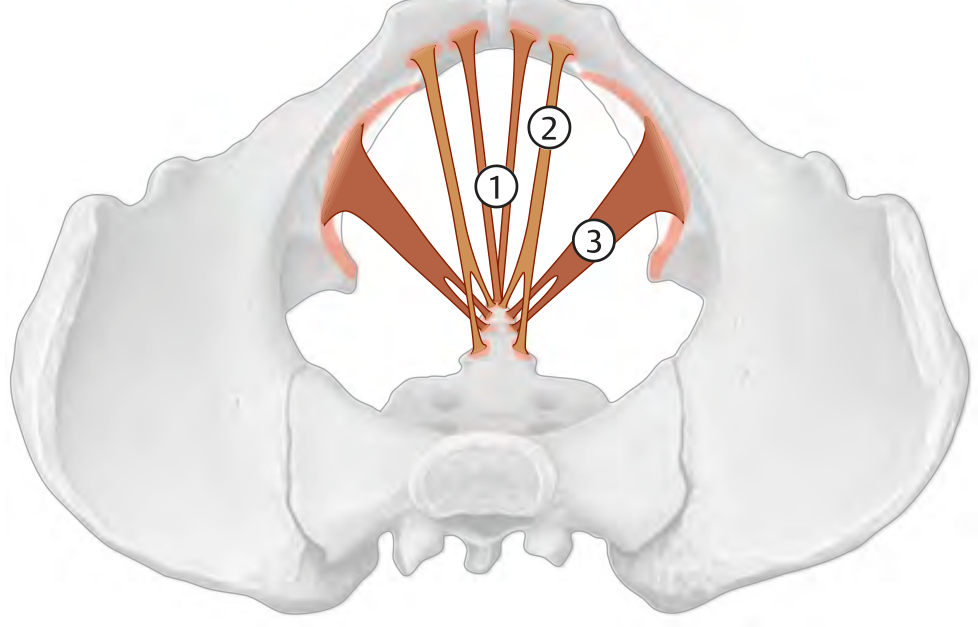
Three Parts of the Levator Ani
1. Puborectalis
- Origin: Superior pubic ramus on both sides of the pubic symphysis, and the superior fascia of the urogenital diaphragm
- Course: Runs backward alongside the anorectal junction; the two muscles join to form a U-shaped muscular sling around the posterior aspect of the anorectal junction
- Insertion: Loop-shaped around the anorectal junction; interwoven with the deep part of the external anal sphincter
- Key function: Maintains the perineal (anorectal) flexure - normally keeps an angle of approximately 90 degrees between the rectum and anal canal, acting as a "pinch valve" to prevent defecation. When the puborectalis relaxes during defecation, this angle opens to approximately 130-140 degrees. This is the single most important muscle for fecal continence.
2. Pubococcygeus
- Origin: Posterior portion of the pubis and the arcus tendineus (lateral to puborectalis origin)
- Insertion: Anococcygeal ligament, coccyx; visceral organs (forms slings around the vagina and urethra)
- Subdivisions based on visceral relationships:
- Puboprostaticus (levator prostatae) - in males
- Pubovaginalis - forms a muscular sling around the vagina in females; functions as a vaginal sphincter
- Pubourethralis - provides urethral support
- Puboanalis - inserts into the wall of the anal canal
- During simulated vaginal delivery, the pubococcygeus muscle has been shown to stretch to more than three times its original length.
3. Iliococcygeus
- Origin: Tendinous arch of the obturator internus fascia (the posterior and lateral portion of the arcus tendineus levator ani)
- Insertion: Iliococcygeal raphe, anococcygeal ligament, coccyx
- The two iliococcygeus muscles join their partners in the midline to form the levator plate (iliococcygeal raphe extending from the anal aperture to the coccyx). This plate acts as a horizontal shelf upon which the pelvic organs rest.
- Weakening of this plate allows it to sag, opening the hiatus and predisposing to pelvic organ prolapse.
Insertion / Midline Attachments of Levator Ani (summary)
- Central tendon of the perineum (perineal body)
- Wall of the anal canal
- Anococcygeal ligament (anococcygeal body/raphe)
- Coccyx
- Vaginal wall (in women)
- Anteriorly: the urogenital hiatus (see below)
The Urogenital Hiatus
The anterior part of the levator ani muscles is separated by a U-shaped defect called the urogenital hiatus (also called the levator hiatus anteriorly). Its margins merge with the walls of the viscera passing through it and with the deep perineal muscles below.
Structures passing through:
- Urethra (both sexes)
- Vagina (females)
- Rectum (passes through the posterior part, the anal hiatus)
The levator hiatus is the complete opening between the levator ani muscle groups that transmits the urethra, vagina, and rectum. The portion of this hiatus ventral to the perineal body is specifically the urogenital hiatus, through which prolapse of the vagina, uterus, bladder, and rectum occurs when tone is lost.
The tonic activity of the levator muscles normally keeps the urogenital hiatus closed by compressing the urethra, vagina, and rectum against the pubic bone. With loss of tone, the hiatus widens, endopelvic fascial ligaments are subjected to excessive load, and prolapse ensues.
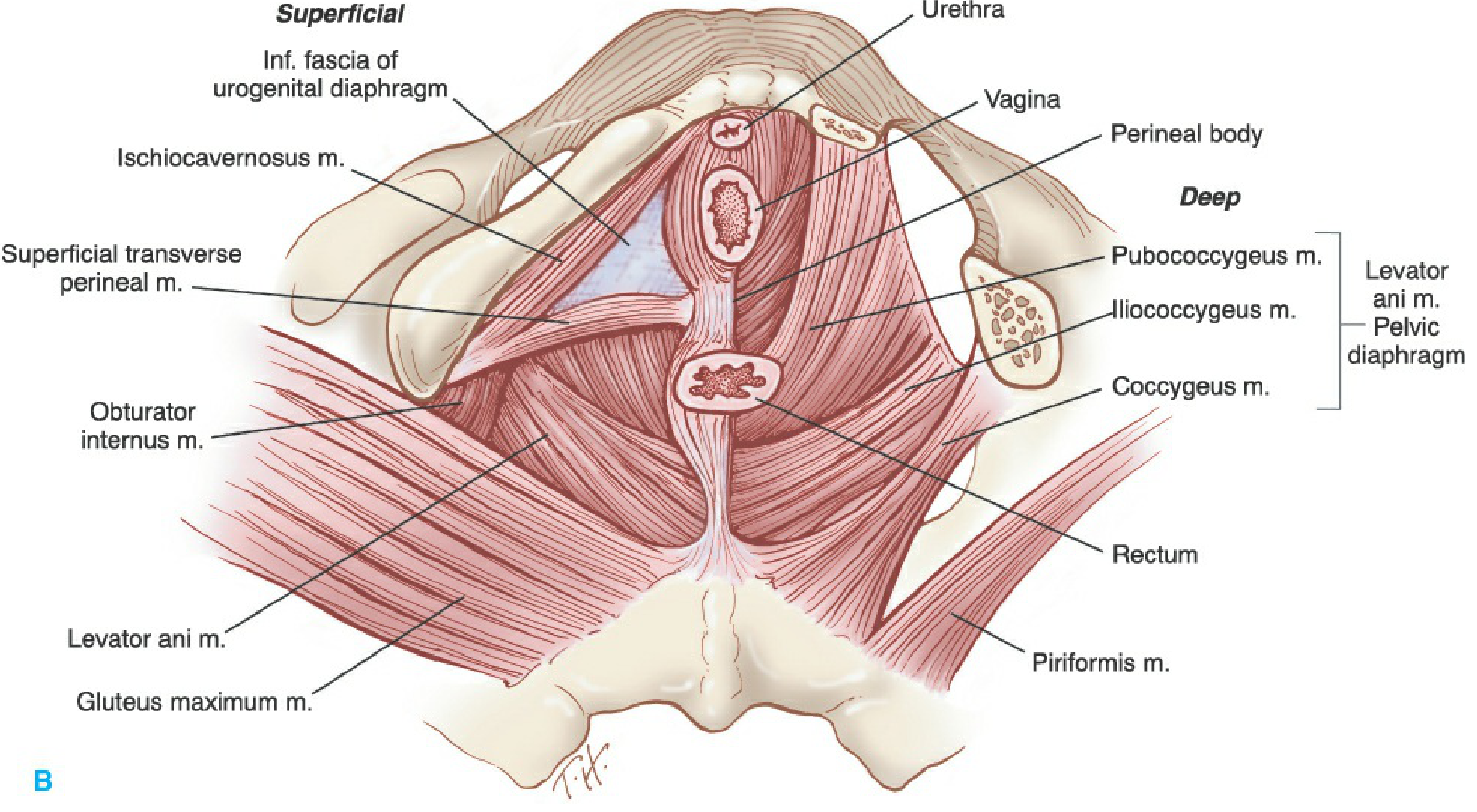
Coccygeus
The coccygeus (ischiococcygeus) completes the posterior part of the pelvic diaphragm. The two triangular coccygeus muscles lie immediately posterior to the iliococcygeus and overlie the sacrospinous ligaments.
| Feature | Detail |
|---|---|
| Origin | Ischial spine and pelvic surface of the sacrospinous ligament |
| Insertion | Lateral margin of the coccyx and adjacent inferior sacrum (S4-S5) |
| Innervation | Direct branches from anterior rami of S4 and S5 |
| Function | Supports pelvic viscera; flexes (pulls forward) the coccyx after defecation |
The coccygeus is functionally the pelvic equivalent of the sacrospinous ligament, which forms its deep (inferior) surface. In some individuals the muscular component degenerates and it becomes predominantly fibrous, effectively fusing with the sacrospinous ligament.
Innervation
This is an area of significant revision in recent decades:
- Traditional teaching: Levator ani muscles are innervated by the pudendal nerve (perineal surface) and direct sacral branches (pelvic surface).
- Current evidence: The levator ani muscles are innervated solely by the levator ani nerve, which travels on the superior (intrapelvic) surface of the muscles without pudendal nerve contribution.
- Originates from S3, S4, and/or S5
- Exits sacral foramina and travels 2-3 cm medial to the ischial spine and ATLA
- Courses across the coccygeus, iliococcygeus, pubococcygeus, and puborectalis
- Occasionally, a separate branch from S5 innervates the puborectalis independently
- Coccygeus: Direct branches from S4 and S5
The levator ani nerve's proximity to the ischial spine and sacrospinous ligament makes it vulnerable to injury during sacrospinous vaginal vault suspension and iliococcygeus suspension procedures.
Muscle Fiber Composition and Tonic Behavior
The levator ani contains predominantly type I (slow-twitch) fibers that maintain a constant resting state of contraction. This baseline tone:
- Keeps the urogenital hiatus narrowed
- Draws the distal urethra, vagina, and rectum toward the pubic bones
- Supports pelvic viscera against gravity and intra-abdominal pressure
Type II (fast-twitch) fibers allow:
- Involuntary reflex contractions with sudden increases in abdominal pressure (coughing, sneezing, Valsalva)
- Voluntary contractions (Kegel exercises)
Relaxation occurs only briefly and intermittently during evacuation (voiding, defecation) and during parturition.
Fasciae of the Pelvic Diaphragm
Superior Fascia (Endopelvic Fascia - Parietal Layer)
- Lines the superior (pelvic) surface of the levator ani
- Continuous with the transversalis fascia of the abdominal wall
- Condensations form important ligaments: arcus tendineus fascia pelvis (ATFP) runs from the lower pubic bone (1 cm lateral to midline) to the ischial spine, providing attachment for the endopelvic fascia supporting the urethra and bladder
- Level II vaginal support is provided by the lateral attachment of the midvagina to the superior fascia of the levator ani via the ATFP (DeLancey's anatomical levels)
Inferior Fascia
- Lines the inferior (perineal) surface of the levator ani
- Forms the medial wall and roof of the ischiorectal (ischioanal) fossa
- The ischiorectal fossa is bounded:
- Medially: inferior fascia of pelvic diaphragm (levator ani)
- Laterally: obturator internus fascia and sacrotuberous ligament
- Content: fat, pudendal nerve and vessels in Alcock's canal
Pelvic Floor Support - DeLancey's Three Levels
The pelvic diaphragm is integral to the three-level support system described by DeLancey (1992):
| Level | Region | Support Structures | Prolapse if Lost |
|---|---|---|---|
| I | Cervix + upper 1/3 vagina | Parametrium, paracolpium, uterosacral/cardinal ligaments | Uterine prolapse or vaginal vault prolapse |
| II | Middle 1/3 vagina | Lateral attachment to superior fascia of levator ani and ATFP | Cystocele (anterior), rectocele (posterior) |
| III | Lower 1/3 vagina | Fusion with perineal membrane, levator ani muscles, perineal body | Deficient perineum, urethral hypermobility |
Functions of the Pelvic Diaphragm (Summary)
- Visceral support - bears the weight of pelvic organs against gravity and intra-abdominal pressure
- Urinary continence - tonic closure of the urogenital hiatus compresses the urethra; reflex fast-twitch contractions resist stress incontinence
- Fecal continence - puborectalis maintains the anorectal angle; relaxation opens this angle during defecation
- Vaginal sphincter function - pubovaginalis narrows the vaginal introitus
- Defecation assistance - relaxation + increased intra-abdominal pressure allows feces passage; levator ani then elevates and returns the anal canal to position
- Parturition - supports the fetal head during cervical dilation; the pubococcygeus guides fetal rotation
- Coccyx control - coccygeus pulls the coccyx forward after defecation
Relations to Adjacent Structures
Ischiorectal Fossa
- Lies below and lateral to the pelvic diaphragm
- Bounded medially by the inferior fascia of the pelvic diaphragm and the external anal sphincter
- Bounded laterally by the obturator internus muscle and its fascia, and the sacrotuberous ligament
- The fossa contains fat, the pudendal nerve and internal pudendal vessels (in Alcock's canal on the lateral wall), the inferior rectal nerve and vessels
- Anteriorly it has a recess extending above the urogenital diaphragm
- Posteriorly it communicates through the sciatic foramina into the pelvis, which allows spread of perirectal infections
Lateral Pelvic Wall
- The obturator internus muscle forms the lateral wall of the pelvis and gives origin to the ATLA
- The piriformis lies posterolaterally and exits through the greater sciatic foramen above the pelvic diaphragm
Surgical Relevance
| Clinical Scenario | Pelvic Diaphragm Relevance |
|---|---|
| Abdominoperineal resection (APR) | The levator ani is the key boundary between abdominal and perineal phases; its division is the primary surgical step in the perineal component |
| Sacrospinous ligament fixation | The levator ani nerve runs 2-3 cm medial to the ischial spine - suture placement risks nerve injury |
| Vaginal delivery | Pubococcygeus stretches >3x its length; up to 20% of primiparous women sustain visible MRI defects in levator ani |
| Pelvic organ prolapse | Levator ani avulsion from pubic bone is the most common site of delivery-related injury |
| Fecal incontinence | Pudendal nerve injury or puborectalis damage abolishes the anorectal angle |
| Kegel exercises | Target type II fast-twitch fibers of levator ani to improve stress urinary incontinence |
| Perirectal abscess | Spreads through ischiorectal fossa and communicates with the pelvis via sciatic foramina |
Sources: Gray's Anatomy for Students, pp. 529-531 | Berek & Novak's Gynecology, pp. 154-159 | Campbell-Walsh-Wein Urology, pp. 3214-3215, 3415-3416 | Thieme Atlas of General Anatomy and Musculoskeletal System, pp. 163, 183, 203 | Fischer's Mastery of Surgery, p. 4058
This is a shared conversation. Sign in to Orris to start your own chat.