Occludable angle stages according to standard book of ophthalmology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete, textbook-sourced answer on occludable angle stages.
Occludable Angle - Stages and Classification
The term "occludable angle" refers to an angle at risk of iridotrabecular contact (ITC) blocking aqueous outflow. The classification has evolved from symptom-based to a disease-stage model based on gonioscopic findings, IOP, and optic nerve status.
A. AIGS Disease-Stage Classification (Kanski's, 10th ed.)
This is the consensus scheme recommended by the Association of International Glaucoma Societies and is the most clinically relevant staging system:
Stage 1: Primary Angle-Closure Suspect (PACS)
- Shallow axial anterior chamber depth (eclipse sign positive - crescentic shadow on nasal iris)
- Gonioscopy: ITC in 3 or more quadrants but no PAS and no raised IOP
- Lower threshold: 2 quadrants of ITC + pigment smudging (signs of intermittent closure)
- Normal IOP, optic disc, and visual field
- AS-OCT confirms an occludable angle
- Risk of progression to overt angle-closure disease is low
Stage 2: Primary Angle Closure (PAC)
- Gonioscopy: ITC in 3 or more quadrants PLUS raised IOP and/or PAS (assessed by indentation gonioscopy)
- Normal optic disc and visual field (no glaucomatous damage yet)
- Subcategory: non-ischaemic vs. ischaemic PAC (the latter shows iris changes or glaukomflecken from prior severe IOP elevation)
Stage 3: Primary Angle-Closure Glaucoma (PACG)
- ITC in 3 or more quadrants
- Glaucomatous optic neuropathy present (structural and/or functional damage)
- Note: Optic nerve damage from acute angle closure may not show typical cupping
B. Shaffer Gonioscopic Grading System
The most widely used grading system for angle width:
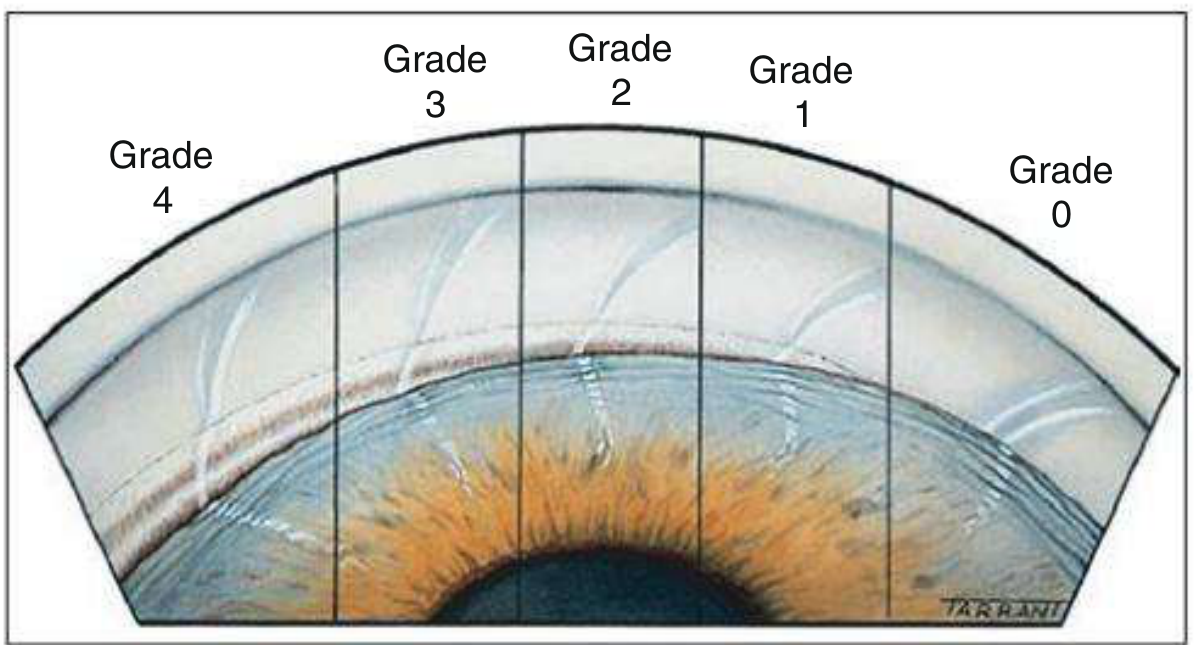
Fig. 11.31 - Kanski's Clinical Ophthalmology, 10th ed.
| Grade | Angle | Structures visible | Clinical significance |
|---|---|---|---|
| 4 | 35-45° | Ciliary body visible without lens tilt | Widest; seen in myopia/pseudophakia - closure not possible |
| 3 | 25-35° | Scleral spur visible | Open angle - closure not possible |
| 2 | 20° | Trabecular meshwork only (no scleral spur) | Closure possible - gonioscopy mandatory |
| 1 | 10° | Schwalbe line ± top of trabeculum | Very narrow - closure probable |
| Slit | - | No iridocorneal contact but no structures seen | Dangerously narrow |
| 0 | 0° | Iridocorneal contact present | Closed (appositional vs. synechial distinguished by indentation) |
Grades 0-1 (and slit) are occludable. Grade 2 is potentially occludable.
C. Van Herick Slit-Lamp Grading (Screening Tool)
Compares peripheral anterior chamber depth to corneal thickness:
| Grade | AC depth : Corneal thickness | Clinical interpretation |
|---|---|---|
| 4 | ≥ 1 (equal or greater) | Wide open |
| 3 | 1/4 - 1/2 | Incapable of closure |
| 2 | = 1/4 | Angle closure possible - formal gonioscopy needed |
| 1 | < 1/4 | Gonioscopy will usually show a dangerously narrow angle |
Important caveat: Van Herick overestimates angle width in plateau iris configuration. It is a screening tool only - not a substitute for gonioscopy.
D. Wills Eye Manual - Spaeth System Guidelines for Occludability
The Spaeth system encodes iris insertion (A/B/C/D/E), angular approach, and peripheral iris curvature. General guidelines for occludability:
Definite occludable angles include:
- Any angle narrower than 10 degrees
- Any "p" (posterior bowing) iris configuration
Potentially occludable angles include:
- Any angle narrower than 20 degrees
- Any "B" (behind Schwalbe line) iris insertion
Examples:
- C15b 2+ ptm = Open but narrow, occludable angle
- A40f = Closed angle
- (B)D30p 0 ptm = Open, atypical narrow angle, occludable with dilation
Key Points
- The primary staging framework is PACS → PAC → PACG based on presence of ITC, PAS, IOP elevation, and optic nerve damage
- Shaffer grades 0 and 1 are definitively occludable; grade 2 is potentially occludable
- Van Herick grade ≤ 2 warrants formal gonioscopy
- Indentation gonioscopy distinguishes appositional (reversible) from synechial (permanent) closure - a management-critical distinction
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. (pp. 389-390); The Wills Eye Manual, pp. 1132-1134
This is a shared conversation. Sign in to Orris to start your own chat.