Paronochia treatment
Reading File
Finding Sources
Searching PubMed
paronychia treatment management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have excellent information from multiple authoritative sources to provide a comprehensive answer.
Paronychia: Treatment
Paronychia is an infection of the soft tissue surrounding the proximal and lateral nail folds. It is one of the most common hand infections. Treatment depends on whether the infection is in its early cellulitic phase, has progressed to abscess, and whether it is acute or chronic.
Classification
| Type | Features |
|---|---|
| Acute | Bacterial (Staphylococcus most common; also anaerobes, gram-negatives, Group A strep, CA-MRSA); painful erythema, swelling, possible pus at nail fold corner |
| Chronic | Usually from repeated irritant/water/trauma exposure; loss of cuticle, nail plate changes, Beau lines; often mixed bacterial/fungal |
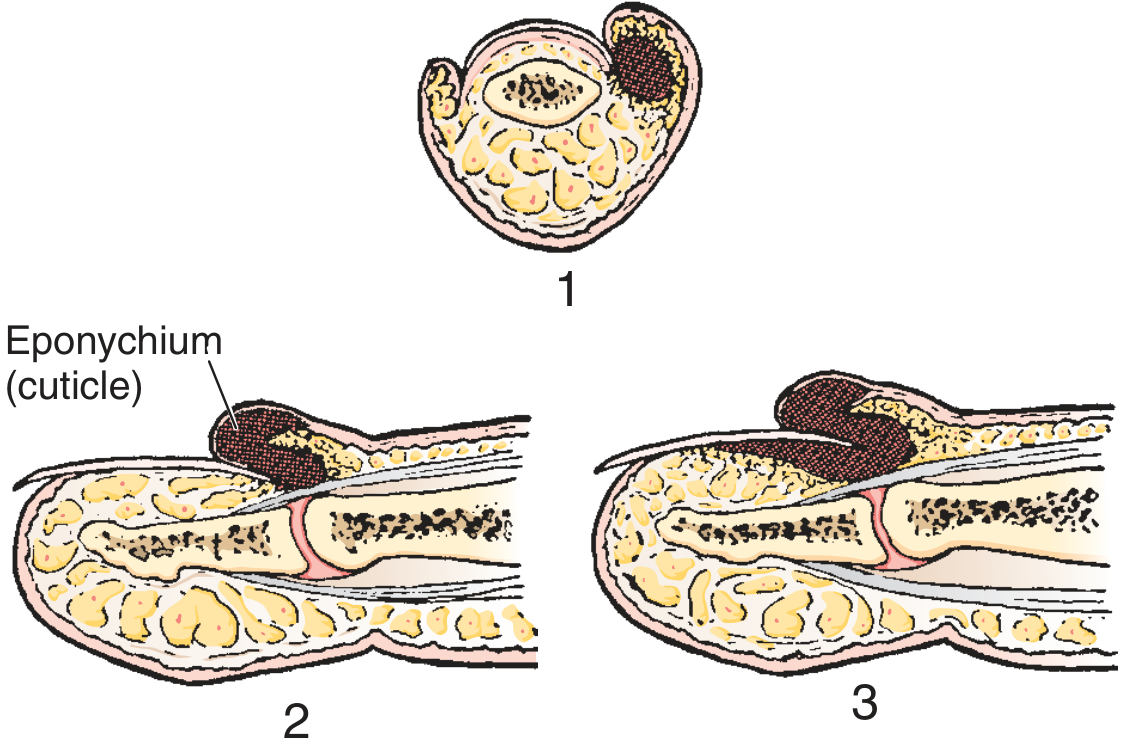
Stages of paronychia: 1 = abscess at side of nail; 2 = infection under eponychium, not yet subungual; 3 = subeponychial and subungual abscess.
Acute Paronychia Treatment
Stage 1 - Early Cellulitis (No Abscess)
- Warm soaks 3x/day
- Topical antibiotics (e.g., mupirocin/Bactroban) with or without topical corticosteroids
- If significant cellulitis is present: oral broad-spectrum antistaphylococcal antibiotic - cephalosporin or semi-synthetic penicillin (e.g., dicloxacillin, cefalexin)
- Incision has no value at the purely cellulitic stage
Stage 2 - Frank Abscess
Drainage is the definitive treatment. Key principles:
- Digital block for anesthesia (not always required for small lesions)
- Elevation of the eponychial fold away from the nail matrix - this alone often allows adequate drainage, as paronychia is a collection in the potential space between cuticle and nail, not a true cutaneous abscess
- A simple nick through the most translucent area of the abscess is usually sufficient
- If the abscess is unilateral, incise at that corner, angling the knife away from the nail to avoid cutting the nail bed (which causes ridging)
- If abscess is under one corner of the nail root, remove that corner of nail
- If infection has migrated to the opposite side and under the nail: make a second incision, reflect the skin proximally, and excise the proximal one-third of the nail
- Pack loosely with iodoform gauze for 48 hours
- Alternative technique: lift the nail fold with the tip of a 21- or 23-gauge needle - resolved 8/10 cases with no anesthesia needed
Antibiotics post-drainage: Generally unnecessary in uncomplicated cases. Reserve for:
- Marked surrounding cellulitis
- Immunocompromised patients
- Diabetics
- Suspicion of CA-MRSA (add TMP-SMX or doxycycline)
Stage 3 - Subungual Abscess
- Full partial or complete nail avulsion is required
- Wound packing + oral antibiotics usually indicated here
Chronic Paronychia Treatment
- Protective measures: cotton-lined rubber gloves to avoid contact with water and irritants
- Topical steroids (for the inflammatory component)
- Topical antimicrobials (including antifungals if Candida is suspected)
- Address the underlying cause (occupational exposure, nail cosmetics, frequent wetting)
Herpetic Whitlow (Important Differential)
HSV-1 or HSV-2 can mimic bacterial paronychia. Key features:
- Clear vesicle formation (rather than frank pus)
- May have lymphangitis and lymphadenopathy
- Confirm with viral culture, Tzanck smear, or serum antibody titers
- Self-limiting - usually resolves without intervention
- Do NOT incise - incision worsens outcome and risks spread
- Acyclovir (oral) can shorten duration, especially in immunocompromised patients
Causative Organisms
| Population | Organisms |
|---|---|
| Adults | Staphylococcus aureus (most common), mixed aerobic/anaerobic (50%), anaerobes alone (25%) |
| Children | Anaerobes (from finger sucking/nail biting), Group A strep (from strep pharyngitis + thumb sucking) |
| HIV patients / EGFR inhibitor users | Acute paronychia as side effect; periungual pyogenic granuloma-like lesions |
| Immunocompromised | Herpetic whitlow, MRSA |
Summary Algorithm
Paronychia
├── No abscess (cellulitis only)
│ └── Warm soaks + topical abx ± topical steroids
│ └── If significant cellulitis: oral antistaphylococcal abx
├── Abscess present
│ └── Drain (lift eponychial fold or small nick)
│ ├── Confined to one side: unilateral incision
│ ├── Under nail root corner: remove that nail corner
│ └── Bilateral / subungual: reflect flap + excise proximal 1/3 nail
│ └── Antibiotics only if: cellulitis, immunocompromised, MRSA risk
└── Chronic paronychia
└── Protective measures + topical steroids + topical antifungals/antibiotics
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine, p.888 | Campbell's Operative Orthopaedics 15e, p.4577 | Goldman-Cecil Medicine | Pfenninger & Fowler's Procedures for Primary Care
This is a shared conversation. Sign in to Orris to start your own chat.