According to respiratory physiology What will happen if lymphatic system for kung is not welloped
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from authoritative textbooks. Let me compose a thorough answer.
What Happens if the Pulmonary Lymphatic System is Not Well Developed?
The pulmonary lymphatic system has several critical functions in normal lung physiology. If it is underdeveloped (hypoplastic) or dysfunctional, there are major consequences across fluid balance, gas exchange, immune defense, and - critically - survival at birth.
1. Normal Role of Pulmonary Lymphatics (Why They Matter)
The lymphatic system in the lung serves three main functions:
A) Fluid drainage and prevention of pulmonary edema
Under normal conditions, there is a net outward filtration pressure of +1 mmHg that continuously pushes fluid from pulmonary capillaries into the interstitial space. The lymphatic pump (operating at approximately -4 to -5 mmHg) removes this excess fluid and returns it to the circulation. Pulmonary lymph flow can reach up to 20 mL/hour.
As Guyton & Hall explains: "The pulmonary capillaries and pulmonary lymphatic system normally maintain a slight negative pressure in the interstitial spaces; whenever extra fluid appears in the alveoli, it is sucked mechanically into the lung interstitium through the small openings between the alveolar epithelial cells. The excess fluid is then carried away through the pulmonary lymphatics. Under normal conditions, the alveoli are kept dry."
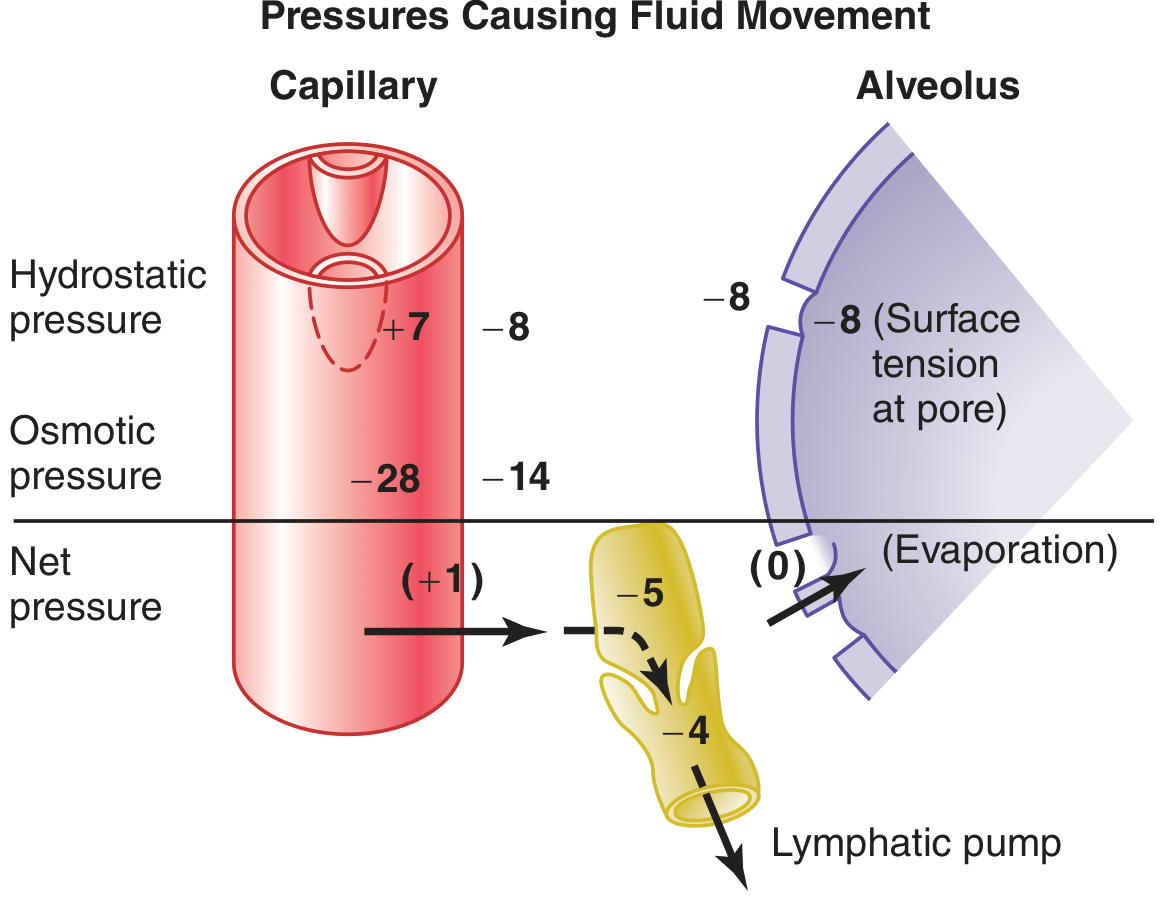
Figure: Hydrostatic and osmotic pressures (in mmHg) at the pulmonary capillary and alveolar membrane, with the lymphatic pump draining excess fluid from the interstitial space. (Guyton & Hall, Fig. 39.7)
B) Immune cell trafficking
Pulmonary lymphatics transport antigen-presenting cells (dendritic cells, macrophages) from the lung parenchyma to mediastinal lymph nodes. This is guided by CCL21 on lymphatic endothelium and CCR7 on T cells/dendritic cells. Without this, adaptive immune responses against inhaled pathogens cannot be properly coordinated.
C) Local immunity / iBALT
Lymphatics contribute to the formation of inducible bronchus-associated lymphoid tissue (iBALT), which allows local antigen presentation without requiring traffic to distant lymph nodes.
2. Consequences of Underdeveloped Pulmonary Lymphatics
A) Pulmonary Edema
This is the most immediate and life-threatening consequence. Without functional lymphatics:
- Interstitial fluid pressure rises from negative into positive range
- Fluid accumulates in the interstitial spaces and then floods the alveoli
- Gas exchange is severely impaired
- The result is non-cardiogenic pulmonary edema and hypoxia
"Any factor that increases fluid filtration out of the pulmonary capillaries OR that impedes pulmonary lymphatic function and causes pulmonary interstitial fluid pressure to rise from the negative range into the positive range will tend to cause filling of the pulmonary interstitial spaces and alveoli with free fluid." - Guyton & Hall
B) Congenital Pulmonary Lymphangiectasia (CPL) - The Clinical Prototype
The human disease that best illustrates underdeveloped/dysfunctional pulmonary lymphatics is Congenital Pulmonary Lymphangiectasia. According to Murray & Nadel:
- Lymphatic endothelial cells (LECs) undergo a critical maturation program just before birth, essential for the first breath
- Disorders of lung lymphatics are an underrecognized cause of early respiratory failure in preterm infants
- Experimental data from genetically engineered mice show that abnormal lymphatic development causes:
- Dilated lymphatics
- Chylous effusions (chyle leaking into pleural space)
- Respiratory failure
- Features identical to human lymphangiectasia
C) Bilateral Pleural Effusions / Chylothorax
Underdeveloped lymphatics cause chylous pleural effusions (chylothorax). According to Creasy & Resnik's Maternal-Fetal Medicine:
"Pulmonary effusions may be bilateral, pointing to pulmonary lymphangiectasia; this carries a poor prognosis despite fetal treatment, because the abnormal lymphatics preclude normal gas exchange in the lung."
These effusions can cause:
- Mediastinal shift
- Abnormal venous return
- Secondary lung compression
- Fetal hydrops
- Intrauterine fetal death (IUFD)
D) Impaired Immune Defense
Without proper lymphatic trafficking:
- Antigen-presenting cells cannot migrate to mediastinal lymph nodes
- The adaptive immune response to inhaled pathogens is delayed or absent
- The lung becomes vulnerable to recurrent infections
- Abnormal BALT/iBALT formation may occur, leading to local inflammatory dysregulation
E) Air Space Enlargement / COPD-Like Changes
Experimental data shows that lymphatic dysfunction alone (without other triggers) can lead to:
- Bronchus-associated lymphoid tissue (BALT) formation
- Air space enlargement resembling emphysema
- This is especially relevant in COPD, where lymphatic vessel density increases around alveolar spaces in advanced disease (Murray & Nadel, Table 7.2)
3. Summary Table
| Consequence | Mechanism |
|---|---|
| Pulmonary edema | No lymphatic drainage of interstitial fluid → alveolar flooding |
| Chylous pleural effusions | Lymph leaks into pleural space instead of draining normally |
| Respiratory failure at birth | Underdeveloped lymphatics fail on first breath |
| Impaired immunity | No antigen-presenting cell trafficking to lymph nodes |
| Air space enlargement | Lymphatic dysfunction leads to BALT and emphysema-like changes |
| Fibrosis (over time) | Persistent fluid and inflammation stimulate fibroblasts |
Key Takeaway
The pulmonary lymphatic system is not merely a "backup drain" - it is essential for keeping the alveoli dry and enabling the first breath. An underdeveloped pulmonary lymphatic system leads primarily to pulmonary edema, chylous effusions, and respiratory failure, which may be fatal in neonates. In survivors, impaired immune trafficking and structural lung remodeling follow over time.
Sources:
- Guyton and Hall Textbook of Medical Physiology (Chapter 39: Pulmonary Circulation, Pulmonary Edema, Pleural Fluid)
- Murray & Nadel's Textbook of Respiratory Medicine (Chapter 7: Pulmonary Lymphatics)
- Creasy & Resnik's Maternal-Fetal Medicine (Fetal Pleural Effusions)
Breathing holding after 100 percent breath holding

5dae96f9-e7c5-448e-970c-b6acc654a1fd.jpeg
Only question 17
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Ganong's has given us the precise, complete answer. Here it is:
Question 17: What Happens to Breath Holding After Inhalation of 100% Oxygen?
Answer: The Breath-Holding Time is PROLONGED (Breaking Point is Delayed)
Explanation
The breaking point of breath holding is the moment when voluntary breath holding can no longer be maintained and a breath must be taken. This breaking point is determined by two chemical stimuli:
| Stimulus | Effect |
|---|---|
| Rising arterial PCO2 (hypercapnia) | Stimulates central chemoreceptors → urge to breathe |
| Falling arterial PO2 (hypoxia) | Stimulates peripheral chemoreceptors (carotid bodies) → urge to breathe |
Both stimuli act together to force the breaking point.
What 100% O2 Inhalation Does
When a person breathes 100% oxygen before breath holding:
- Alveolar PO2 rises dramatically (from ~100 mmHg on room air to ~673 mmHg on 100% O2 at sea level)
- This creates a large oxygen reserve in the alveoli and arterial blood
- During the subsequent breath hold, it takes much longer for alveolar/arterial PO2 to fall to hypoxic levels
- The peripheral chemoreceptor (carotid body) stimulus is therefore delayed
- Result: The breaking point is delayed - the person can hold their breath for a significantly longer time
"Breathing 100% oxygen before breath holding raises alveolar PO2 initially, so that the breaking point is delayed." — Ganong's Review of Medical Physiology, 26th Edition
Important Parallel Comparison
The same principle applies to hyperventilation of room air - it blows off CO2, lowering arterial PCO2 at the start, which also delays the breaking point. However, hyperventilation is dangerous (can cause syncope from hypocapnia-induced cerebral vasoconstriction before the hypoxic breaking point is felt).
Mechanistic Summary
Inhale 100% O2
↓
Alveolar PO2 ↑↑ (very high oxygen reserve)
↓
During breath hold → PO2 falls slowly from a high baseline
↓
Carotid body stimulation is DELAYED
↓
Breaking point is DELAYED
↓
Breath holding time is PROLONGED
Source: Ganong's Review of Medical Physiology, 26th Edition - Chapter 36: Breath Holding
This is a shared conversation. Sign in to Orris to start your own chat.