Airway assessment with recent updates and also USG ASSESSMENT
Reading File
Finding Sources
Finding Sources
Searching PubMed
airway assessment ultrasound prediction difficult intubation
Reading File
Reading File
Finding Sources
Reading Article
PMID: 40891437
Reading Article
PMID: 39020308
Reading File
Finding Sources
Finding Sources
Searching the Web
airway ultrasound assessment 2024 2025 update difficult intubation prediction POCUS
Reading File
Reading File
Finding Sources
Reading Web Page
https://www.bjanaesthesia.org.uk/article/S0007-0912(25)00693…
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content. Let me compile the complete, detailed response.
Airway Assessment: Comprehensive Review with Recent Updates & Ultrasound Assessment
1. WHY AIRWAY ASSESSMENT MATTERS
Preanesthetic airway assessment is mandatory before every anesthetic procedure. Up to 15% of initial emergency intubation attempts fail with standard techniques, and ~1-3% overall intubations are problematic. Failed airway management remains a leading cause of anesthesia-related mortality. The goal is to identify patients at risk of:
- Difficult mask ventilation
- Difficult supraglottic airway (SGA) placement
- Difficult laryngoscopy
- Difficult tracheal intubation
- Difficult surgical airway (front-of-neck access)
(Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 570)
2. STANDARD CLINICAL AIRWAY ASSESSMENT
A. History
- Prior anesthetic records (previous difficult airway)
- Symptoms: dysphagia, odynophagia, stridor, positional dyspnea, changes in voice
- Diseases: rheumatoid arthritis (atlanto-axial instability), obesity, diabetes (stiff joint syndrome), previous neck surgery, radiotherapy, burns
- Neck masses, obstructive sleep apnea
B. Physical Examination - Bedside Tests
1. Mouth Opening (Inter-incisor Distance)
- Normal: >3 cm (3 fingerbreadths) in adults
- <3 cm predicts difficulty
2. Mallampati Classification (Modified Samsoon & Young)
Performed with patient seated, mouth maximally open, tongue protruded, phonation avoided:
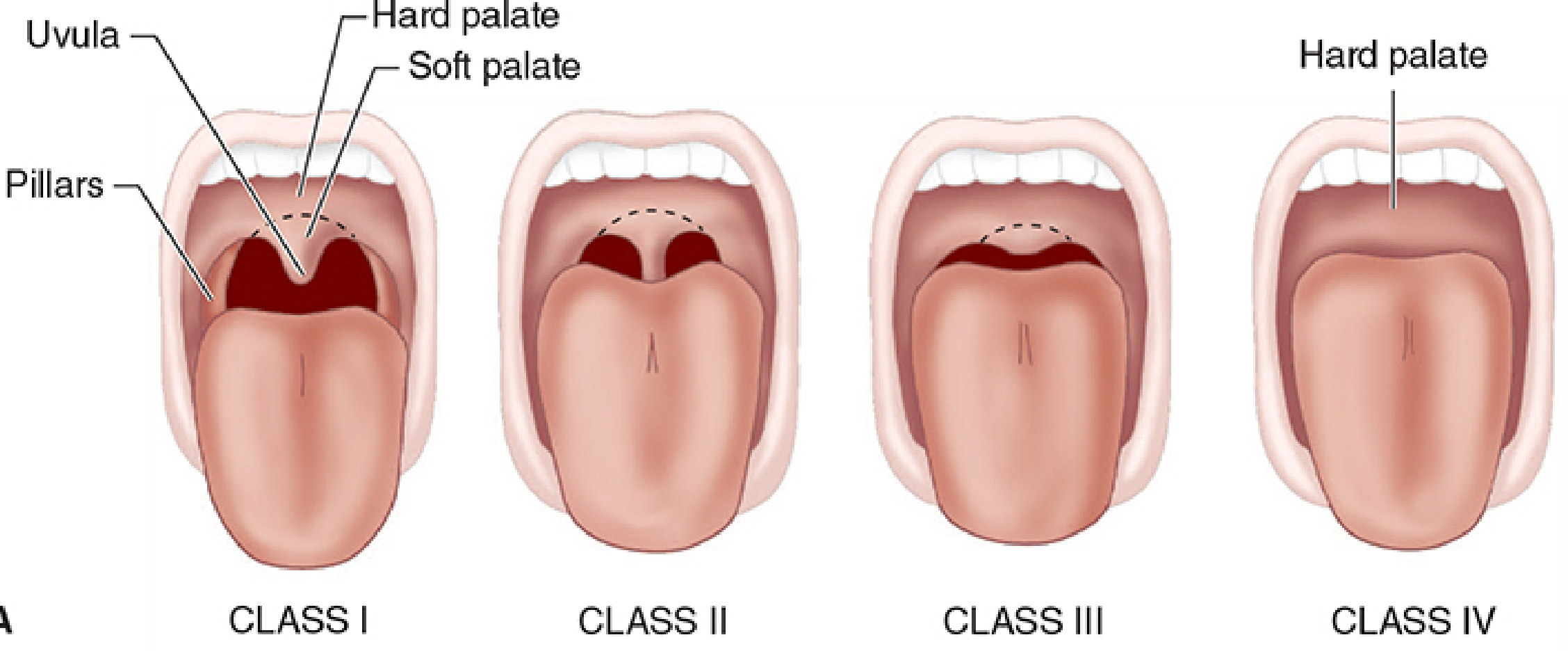
| Class | Structures Visible |
|---|---|
| I | Full uvula, faucial pillars, soft & hard palate |
| II | Upper pillars, most uvula |
| III | Only soft & hard palate |
| IV | Only hard palate |
- Class III/IV predicts difficult intubation (corresponds to Cormack-Lehane Grade III/IV on laryngoscopy)
- Sensitivity ~39%, Specificity ~86% (2024 meta-analysis, 686,089 patients)
3. Thyromental Distance (TMD / Patil's test)
- Measured from the mentum to superior thyroid notch with neck fully extended
- Normal: >6.5 cm (3 fingerbreadths)
- <6 cm = difficult intubation likely
- Sensitivity ~38%, Specificity ~83%
4. Sternomental Distance
- Chin to sternal notch, neck extended
- Normal: >12.5 cm
5. Upper Lip Bite Test (ULBT)
| Class | Finding |
|---|---|
| Class I | Lower incisors bite upper lip above the vermilion border |
| Class II | Lower incisors bite below vermilion border |
| Class III | Cannot bite upper lip |
- Class III = difficult intubation; Sensitivity ~52%, Specificity ~84% (best single predictor among physical exam tests per 2024 meta-analysis)
6. Neck Circumference
- >40 cm associated with difficult bag-mask ventilation
- >17 inches (43 cm) associated with difficult glottic visualization
7. Neck Mobility
- Normal: flexion/extension 90°+
- Reduced in rheumatoid arthritis, ankylosing spondylitis, prior fusion, halo traction
8. 3-3-2 Rule (for laryngoscopy geometry)
- 3 fingers = inter-incisor gap
- 3 fingers = hyoid-to-chin distance (mandibular space)
- 2 fingers = hyoid to thyroid notch (to ensure larynx is in submandibular space)
9. Cormack-Lehane Grading (at direct laryngoscopy)
| Grade | View |
|---|---|
| I | Full glottis visible |
| II | Only posterior commissure visible |
| III | Only epiglottis visible |
| IV | No laryngeal structures visible |
(Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 570-571)
3. MULTIVARIATE SCORING SYSTEMS
LEMON Score (Emergency Medicine Standard)
(Tintinalli's Emergency Medicine; Rosen's Emergency Medicine)
| Letter | Component | Score |
|---|---|---|
| L | Look externally (facial trauma, large incisors, beard, large tongue, morbid obesity) | 1 |
| E | Evaluate 3-3-2 rule (any abnormality) | 1 |
| M | Mallampati score >3 | 1 |
| O | Obstruction (epiglottitis, peritonsillar abscess, trauma) | 1 |
| N | Neck mobility reduced | 1 |
- Score 0-1: lower risk; Score ≥3: high risk for difficult intubation
- Widely used in emergency settings; higher scores predict difficult laryngoscopy
Wilson Risk Score (5 factors, score ≥2 = difficult intubation risk)
- Weight >90 kg
- Head & neck movement <90°
- Jaw movement limited
- Receding mandible
- Buck teeth
El-Ganzouri Score (multiparameter, range 0-12)
Components: mouth opening, TMD, Mallampati, neck mobility, ability to prognath, weight, history of difficult intubation
(2024 Systematic Review, 227 studies, 686,089 patients - Wang Z et al., BMC Anesthesiology)
4. PREDICTORS OF DIFFICULT BAG-MASK VENTILATION
MOANS Mnemonic:
- M - Mask seal (beard, facial abnormality)
- O - Obesity/Obstruction
- A - Age >55 years
- N - No teeth (edentulous)
- S - Snoring/Stiff lungs (COPD, pregnancy)
5. THE DIFFICULT AIRWAY ALGORITHM (ASA/DAS)
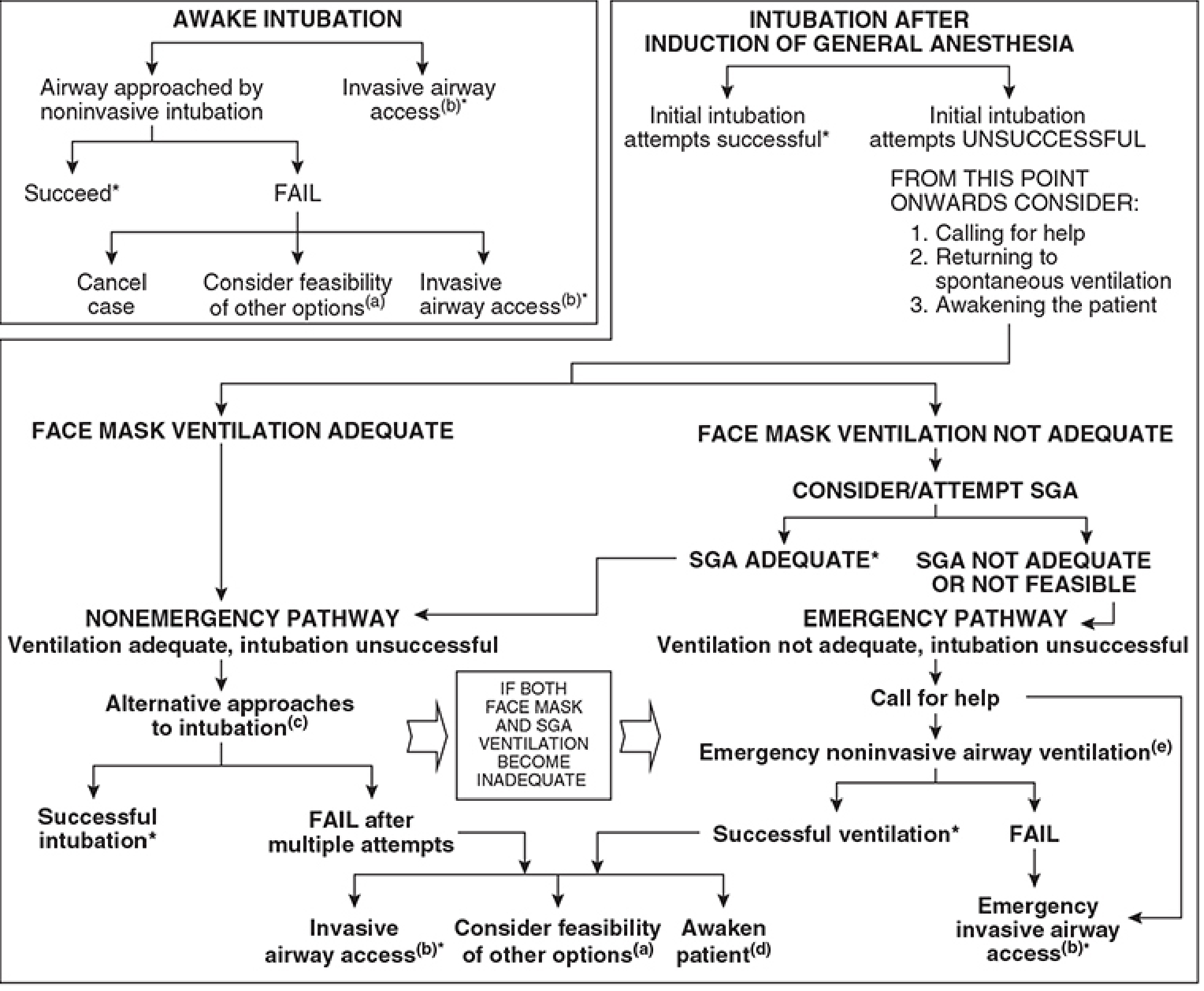
ASA Task Force - 4 Core Steps:
- Assess likelihood of difficult: cooperation/consent, mask ventilation, SGA, laryngoscopy, intubation, surgical airway
- Actively pursue supplemental O2 throughout
- Consider basic choices: Awake vs. asleep intubation; non-invasive vs. invasive; video laryngoscopy as initial approach; preserve vs. ablate spontaneous ventilation
- Primary + alternative strategies ready before induction
Unanticipated difficult airway:
- If face mask ventilation adequate → Nonemergency pathway → alternative intubation devices
- If face mask ventilation NOT adequate → Attempt SGA → if SGA adequate = nonemergency pathway; if SGA fails → Emergency pathway → Front-of-Neck Access (FONA)
(Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 608-609)
6. ULTRASOUND (USG/POCUS) AIRWAY ASSESSMENT
Why USG? The Paradigm Shift
Traditional bedside tests have poor sensitivity (Mallampati Sn ~39%, TMD Sn ~38%). A landmark 2025 systematic review and meta-analysis (Soni et al., Anaesthesia, 60 studies, 10,580 patients, 58 parameters) established POCUS as a superior and additive tool.
USG Applications in Airway Assessment
A. Prediction of Difficult Laryngoscopy
Key Measurement: Distance from Skin to Vocal Cords (DSVC)
- Linear high-frequency probe (7-12 MHz), transverse view at level of thyroid cartilage
- Pooled Sensitivity: 0.84 (95%CI 0.74-0.91)
- Pooled Specificity: 0.81 (95%CI 0.61-0.92)
- AUROC: 0.87 - HIGH certainty of evidence
B. Prediction of Difficult Tracheal Intubation
Best Measurement 1: Distance from Skin to Epiglottis (DSE)
- Transverse probe at hyoid level, scan down to visualize epiglottis
- Sensitivity: 0.80, Specificity: 0.86 - HIGH certainty of evidence
- Increased DSE = more soft tissue = more difficult intubation
Best Measurement 2: Distance from Skin to Hyoid (DSH)
- Highest AUROC: 0.86 (95%CI 0.73-0.92) - moderate certainty
- Sensitivity 0.78, Specificity 0.81
C. Prediction of Difficult Bag-Mask Ventilation
- Tongue thickness (assessed at floor-of-mouth): increased thickness associated with difficult mask ventilation
- Useful in obese patients where clinical assessment is unreliable
D. Cricothyroid Membrane (CTM) Identification
- Gold standard application with strongest evidence
- USG vs. palpation for CTM identification - OR: 3.61 (95%CI 2.20-5.92) - moderate-high certainty
- DAS 2025 guidelines explicitly recommend USG (or visual assessment) for CTM identification during preoperative airway assessment, especially in obese patients or those with difficult anatomy
- Technique: Linear probe, midline neck, longitudinal scan - identify thyroid cartilage (hyperechoic) → CTM (hypoechoic band between thyroid and cricoid cartilages) → cricoid ring
E. Endotracheal Tube Confirmation
Correct tracheal placement:
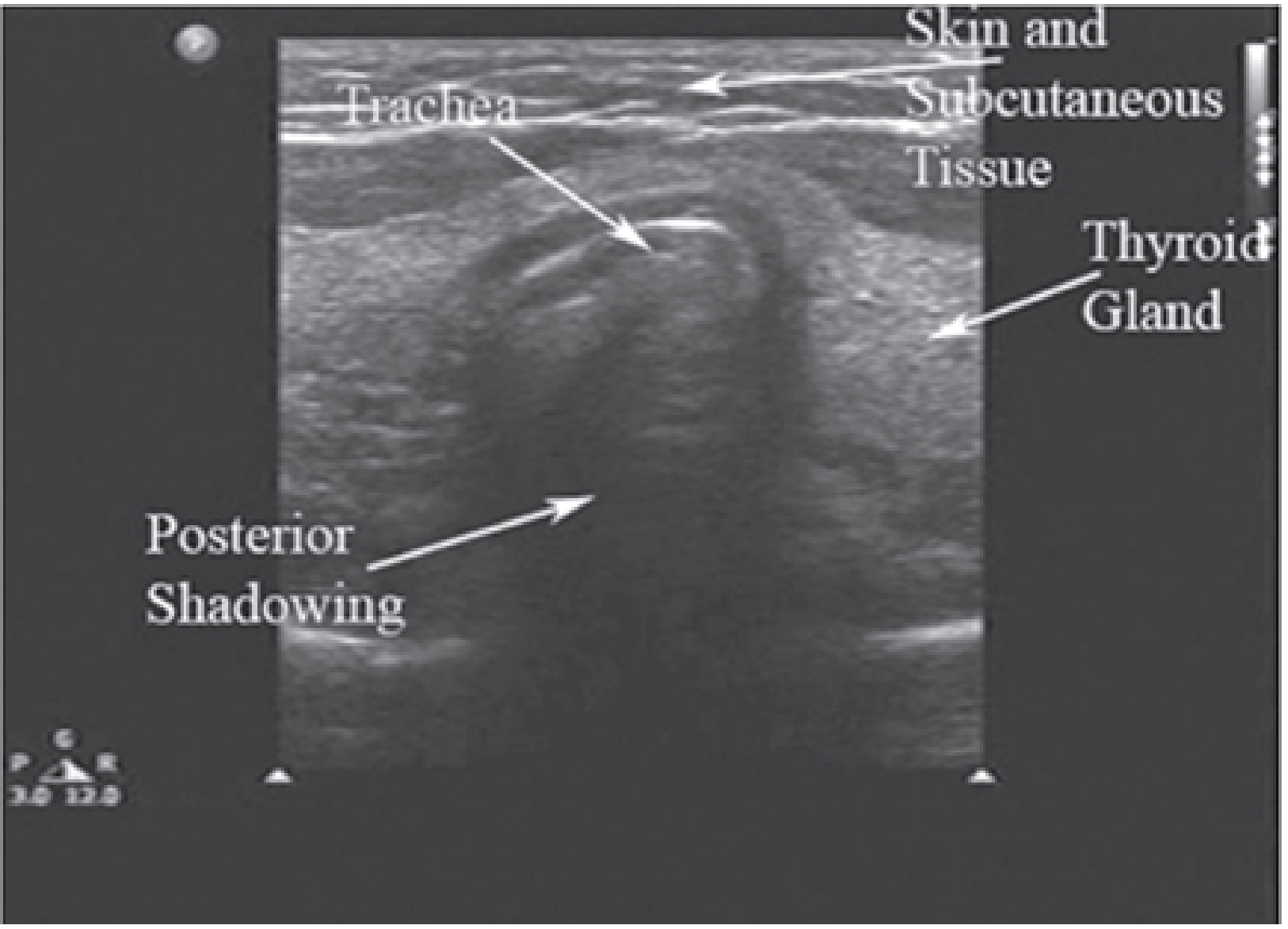
- Trachea: hyperechoic horseshoe-shaped cartilage, posterior acoustic shadowing (air artifact)
- On intubation: single echogenic line (comet-tail artifact) in trachea = correct placement
- Esophageal intubation: second lumen appears posterior/lateral to trachea ("double trachea sign")
- Useful when capnography unreliable (low cardiac output, cardiac arrest)
F. Percutaneous Tracheostomy Guidance
- USG use associated with higher first-pass success: OR 3.9 (95%CI 2.1-7.1) - low-moderate certainty
- Identifies tracheal rings, avoids inadvertent vessel injury, confirms Seldinger wire position
(Soni VM et al., Anaesthesia, 2025, PMID: 40891437; Morgan & Mikhail 7e, p. 572; Miller's Anesthesia 10e, p. 5081; Barash Clinical Anesthesia 9e, p. 4528)
USG Technique Summary
| Structure | Probe | View | Clinical Use |
|---|---|---|---|
| Tongue/Floor of mouth | Linear 7-12 MHz | Sagittal submental | Tongue thickness for difficult MV |
| Hyoid bone | Linear | Transverse at hyoid | DSH for difficult intubation |
| Epiglottis | Linear/Curvilinear | Transverse at thyrohyoid | DSE for difficult intubation |
| Vocal cords | Linear | Transverse at thyroid | DSVC for difficult laryngoscopy |
| Cricothyroid membrane | Linear | Midline longitudinal/transverse | CTM identification for FONA |
| Trachea | Linear | Transverse at suprasternal notch | ETT confirmation |
7. RECENT UPDATES (2024-2025)
DAS 2025 Guidelines (Difficult Airway Society)
(Ahmad I et al., Br J Anaesth, 2025)
Key new recommendations:
- Video laryngoscopy as the initial approach for all anticipated and unanticipated difficult airways
- Ultrasound identification of the CTM is now recommended as a standard step during airway assessment - ideally with neck in neutral or extended position preoperatively
- Maximum 3 attempts at laryngoscopy before escalating (same operator); call for help early
- Physiologically difficult airway concept: hemodynamically unstable, hypoxic, or acidotic patients - POCUS cardiac/gastric assessment integrated into airway planning
- Front-of-neck access (FONA) = scalpel cricothyrotomy preferred over needle technique in emergency
2024 Meta-Analysis Findings (Wang Z et al., BMC Anesthesiology, 2024 - 686,089 patients)
- No single test is superior
- Ultrasound DSE outperforms all traditional tests with Sn 0.80, Sp 0.77
- ULBT performs better than Mallampati alone
- Composite/multimodal assessment mandatory - no single test sufficient
- AI and deep learning for real-time airway prediction emerging
2025 POCUS Meta-Analysis (Soni VM et al., Anaesthesia, 2025 - 10,580 patients)
- Skin-to-vocal cords = best single predictor for difficult laryngoscopy (AUROC 0.87)
- Skin-to-epiglottis = best for difficult intubation (Sn 0.80, Sp 0.86)
- USG CTM identification superior to palpation (OR 3.61)
- POCUS should be integrated with standard tests - not used in isolation
8. SPECIAL SITUATIONS
Obese Patients
- Neck circumference >40 cm = strong predictor of difficult mask ventilation
- Ramp position ("sniffing" extended with shoulders elevated) mandatory
- USG tongue thickness and DSE especially useful when standard exam unreliable
Obstetric Airway
- Mallampati score worsens during labor (edema, fluid shifts)
- Higher risk of difficult and failed intubation than general surgical population
- Failed intubation rate ~1:300 in obstetrics vs. ~1:2000 general
Trauma / Emergency Airway
- LEMON score used to stratify risk quickly
- Assume cervical spine injury = manual in-line stabilization during laryngoscopy
- Blood/secretions = SALAD technique (Suction-Assisted Laryngoscopy Airway Decontamination)
- POCUS in trauma: predicts difficult airway, confirms ETT, identifies CTM in distorted anatomy
Cannot Intubate, Cannot Oxygenate (CICO)
- Call for help immediately
- SGA attempt
- If SGA fails → Scalpel cricothyrotomy (DAS 2025: preferred over needle technique)
- Ultrasound pre-marking of CTM reduces time to surgical airway in CICO
9. KEY TAKEAWAYS
| Test | Sensitivity | Specificity | Clinical Role |
|---|---|---|---|
| Mallampati (MMT) | 39% | 86% | Standard screen |
| TMD | 38% | 83% | Standard screen |
| ULBT | 52% | 84% | Better than MMT |
| USG Skin-to-Epiglottis | 80% | 86% | Best single predictor |
| USG Skin-to-Vocal Cords | 84% | 81% | Best for laryngoscopy prediction |
| USG CTM identification | Outperforms palpation (OR 3.61) | FONA preparation |
Bottom line: No single test predicts difficult airway reliably. A multimodal approach - combining history, LEMON/physical exam, and POCUS - is recommended by both the 2024 meta-analysis and DAS 2025 guidelines. POCUS has emerged as the highest-performing adjunct, particularly for CTM identification and predicting difficult intubation/laryngoscopy.
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e (pp. 570-573, 608-609)
- Miller's Anesthesia, 10e (p. 5081)
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e (p. 4528)
- Tintinalli's Emergency Medicine, Rosen's Emergency Medicine
- Soni VM et al., Anaesthesia, 2025 (PMID 40891437) - POCUS airway meta-analysis (60 studies, 10,580 patients)
- Wang Z et al., BMC Anesthesiology, 2024 (PMID 39020308) - Airway prediction methods meta-analysis (227 studies, 686,089 patients)
- Ahmad I et al., Br J Anaesth, 2025 - DAS 2025 Guidelines for unanticipated difficult intubation
This is a shared conversation. Sign in to Orris to start your own chat.