Burning redness swelling of the eyes what will be the management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a complete, well-structured answer. Here is the full management guide:
Management of Burning, Redness, and Swelling of the Eyes (Conjunctivitis)
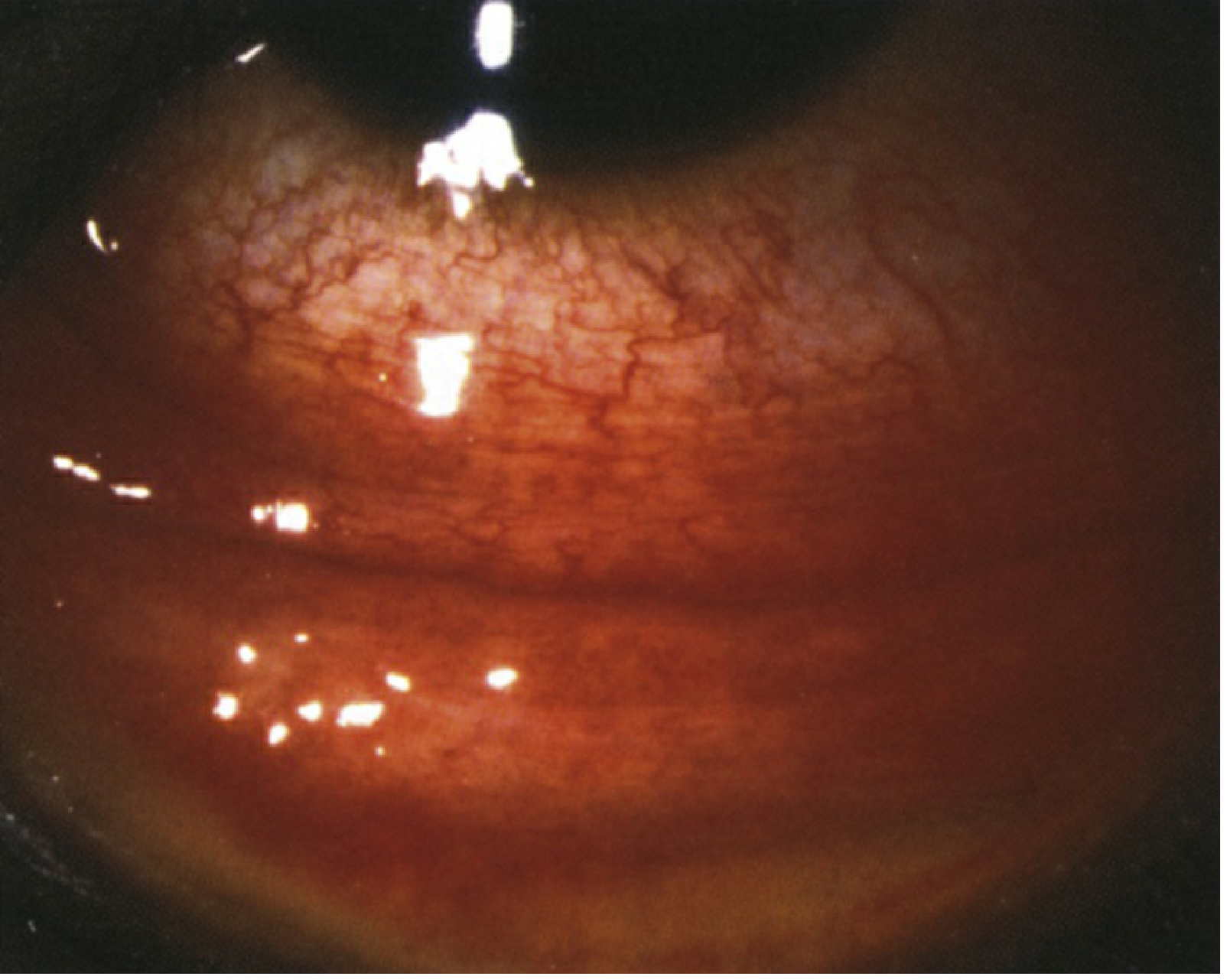
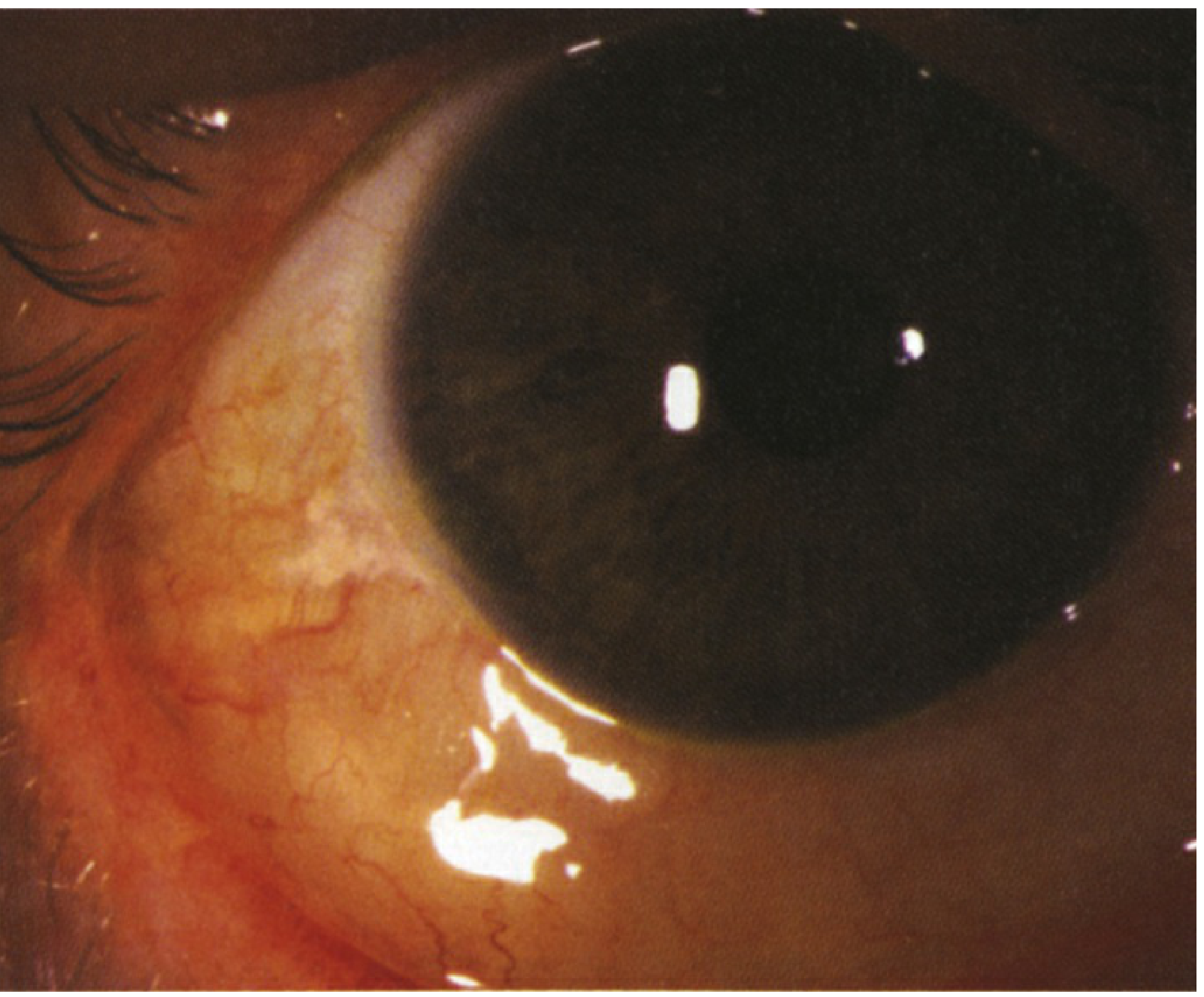
Burning, redness, and swelling of the eyes is the classic presentation of conjunctivitis - inflammation of the conjunctiva. The first step is identifying the cause, as management differs significantly between types.
Step 1 - Identify the Type
Before treating, classify the conjunctivitis based on history and signs:
| Feature | Viral | Bacterial | Allergic |
|---|---|---|---|
| Discharge | Watery / serous | Mucopurulent (yellow/green) | Stringy / white |
| Itch | Mild-moderate | Mild | Prominent |
| Bilateral | Often starts unilateral | Usually bilateral | Bilateral |
| Lymph node | Palpable preauricular node | Absent (except gonorrhea) | Absent |
| History | Recent URI, contact with infected person | None specific | Allergy history, seasonal |
| Eyelids stuck shut | Morning crusting | More prominent | Less common |
Purulent (thick yellow) discharge + no preauricular node = bacterial. Watery discharge + preauricular node + burning = viral. Itching + watery + allergy history = allergic. - Wills Eye Manual, §5.1; Textbook of Family Medicine 9e, p. 347
VIRAL CONJUNCTIVITIS
Most commonly adenovirus. Self-limited - usually resolves in 2-3 weeks. No antibiotic is indicated for uncomplicated viral conjunctivitis.
Treatment:
- Artificial tears (preservative-free) 4-8 times/day for 1-3 weeks - use single-use vials to prevent spread
- Cool compresses several times per day
- Antihistamine drops (e.g., epinastine 0.05% b.i.d.) if itching is severe
- Topical steroids only if:
- A membrane/pseudomembrane is present (peel gently with cotton-tip applicator first)
- Subepithelial infiltrates (SEIs) reduce vision or cause photophobia
- Use loteprednol 0.5% or prednisolone acetate 1% q.i.d., taper over weeks
- Infection control - highly contagious for 10-12 days:
- Frequent hand washing
- Avoid touching eyes, sharing towels or pillows
- Restrict school/work while eyes are red and weeping
- The Wills Eye Manual, §5.1
BACTERIAL CONJUNCTIVITIS
Most commonly caused by Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis. Usually self-limiting in 7-14 days but antibiotics shorten duration.
Treatment:
- Topical broad-spectrum antibiotic drops for 5-7 days:
- Fluoroquinolones (first choice): Ciprofloxacin 0.3% or ofloxacin 0.3% - 4 times/day
- Tobramycin 0.3% or gentamicin 0.3% - q.i.d.
- Chloramphenicol 0.5% drops q.i.d. (widely used, effective)
- Azithromycin 1% b.i.d. × 3 days (convenient dosing)
- Lid hygiene - clean crusting from lids with warm water and clean cloth
- Irrigation to remove excessive discharge in hyperpurulent cases
- Discontinue contact lenses until 48 hours after complete resolution
Special cases:
-
Gonococcal conjunctivitis (hyperacute, profuse purulent discharge, risk of corneal perforation): requires IV/IM ceftriaxone 1g single dose + topical fluoroquinolone + urgent referral
-
Neonatal conjunctivitis (ophthalmia neonatorum): requires urgent investigation (Gram stain, culture) and systemic treatment based on organism
-
Kanski's Clinical Ophthalmology 10th, p. 188-189; Bailey and Love's Surgery 28th, p. 754
ALLERGIC CONJUNCTIVITIS
Treatment (stepwise):
- Eliminate the inciting agent (dust, pollen, pet dander). Wash hair and clothes frequently
- Cool compresses several times per day
- Topical drops by severity:
- Mild: Artificial tears 4-8 times/day
- Moderate: Antihistamine/mast-cell stabilizer drops:
- Olopatadine 0.2% once daily (OTC), or 0.7% once daily
- Azelastine 0.05% b.i.d.
- Ketotifen 0.025% b.i.d. (OTC)
- Bepotastine 1.5% b.i.d.
- Ketorolac 0.5% q.i.d. (NSAID - reduces inflammation but monitor for corneal toxicity with prolonged use)
- Severe: Add mild topical steroid for 1-2 weeks:
- Loteprednol 0.2% q.i.d. or fluorometholone 0.1% q.i.d.
- Oral antihistamine (e.g., cetirizine, loratadine, diphenhydramine 25 mg q6h) for systemic allergy symptoms
- The Wills Eye Manual, §5.1; Textbook of Family Medicine 9e
General Supportive Measures (All Types)
| Measure | Detail |
|---|---|
| Hand hygiene | Wash hands frequently; avoid rubbing eyes |
| Cold compresses | 10-15 min, 3-4 times/day - reduces burning and swelling |
| Avoid contact lenses | Until fully resolved + 48h after last antibiotic dose |
| Avoid sharing | Towels, pillows, eye makeup |
| No eye patching | Patching worsens bacterial/viral conjunctivitis |
Red Flags - Refer Urgently to Ophthalmology
These features suggest a more serious condition beyond simple conjunctivitis:
- Photophobia + red ring around cornea (ciliary injection) - suggests iritis/uveitis
- Visual loss at any point
- Severe pain (not just irritation)
- Corneal opacity or ulcer on fluorescein staining
- Hyperacute profuse purulent discharge - gonococcal conjunctivitis
- Neonatal conjunctivitis - always urgent
- No improvement after 1 week of appropriate treatment
Textbook of Family Medicine 9e - "The triad of red eye, pain, and loss of vision should always alert the examiner to the possibility of a more serious ocular condition."
Quick Summary Table
| Type | First-Line Treatment | Duration |
|---|---|---|
| Viral | Artificial tears + cool compresses | Self-limiting, 2-3 weeks |
| Bacterial (mild/moderate) | Topical ciprofloxacin or tobramycin | 5-7 days |
| Bacterial (gonococcal) | IM/IV ceftriaxone + topical fluoroquinolone | Urgent/systemic |
| Allergic (mild) | Artificial tears, remove allergen | As needed |
| Allergic (moderate) | Olopatadine or ketotifen drops | Seasonal/as needed |
| Allergic (severe) | Above + loteprednol 0.2% q.i.d. | 1-2 weeks |
| Chlamydial | Oral azithromycin 1g single dose OR doxycycline 100 mg b.i.d. × 7 days | Systemic treatment needed |
Sources: The Wills Eye Manual (§5.1 Acute Conjunctivitis); Kanski's Clinical Ophthalmology 10th ed.; Bailey and Love's Short Practice of Surgery 28th ed.; Textbook of Family Medicine 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.