squamous cell Ca from first aid for Fcps exam prep
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive data from Robbins. Let me compile the full FCPS-level answer on Squamous Cell Carcinoma.
Squamous Cell Carcinoma (SCC) - FCPS Exam Prep
Based on Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease
Overview
SCC is a malignant tumor of squamous epithelial cells. It arises at multiple sites - skin, oral cavity/oropharynx, lung, esophagus, cervix, and vulva. The skin is the most common site.
CUTANEOUS SCC
Epidemiology
- Second most common skin malignancy (after BCC)
- Higher incidence in males (except lower leg lesions)
- Arises on sun-exposed sites in older adults with lighter skin types
- Responsible for ~8,000 deaths/year from metastatic disease (roughly equal to metastatic melanoma)
Risk Factors / Etiology
| Factor | Notes |
|---|---|
| UV light (most important) | DNA damage, high mutational load; proportional to lifetime sun exposure |
| Xeroderma pigmentosum | Defective nucleotide excision repair of pyrimidine dimers - exceptionally high risk |
| Immunosuppression | Organ transplant recipients, chemotherapy - reduces immune surveillance |
| HPV (subtypes 5, 8, 16) | Genital skin (HPV-16); rare epidermodyplasia verruciformis (HPV-5/8) |
| Industrial carcinogens | Tars, oils, arsenicals |
| Chronic non-healing ulcers | Marjolin's ulcer - SCC in burn scars, draining osteomyelitis |
| Ionizing radiation | |
| Actinic keratosis | Premalignant precursor lesion |
Pathogenesis / Molecular Genetics
- TP53 mutations - most common; found in actinic keratoses (early event); occur at pyrimidine dimer sites (UV signature)
- RAS activating mutations - increase proliferation
- NOTCH loss-of-function - Notch receptors normally regulate squamous differentiation; loss promotes uncontrolled growth
- UV light also causes transient defect in cutaneous innate immunity
Morphology
Gross:
- In situ: sharply defined, red, scaly plaques (Bowen's disease)
- Invasive: nodular, keratotic/scaly, may ulcerate; raised indurated borders
Microscopy:
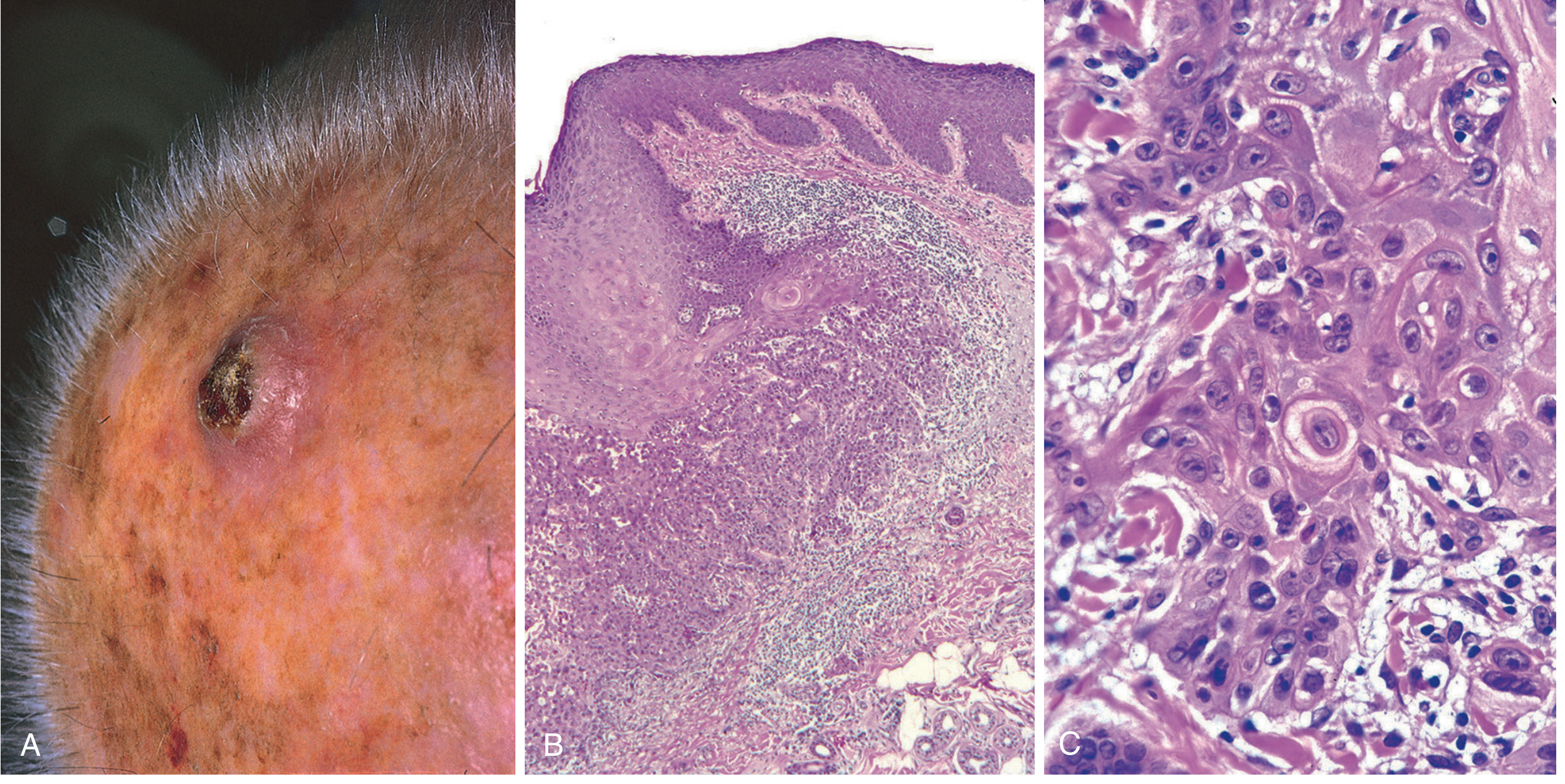
Fig. 25.13 Invasive squamous cell carcinoma. (A) Nodular ulcerated scalp lesion. (B) Atypical squamous epithelium transgressing basement membrane with a keratin pearl at center. (C) High-power showing keratin pearls and individual cell dyskeratosis. (Robbins, Cotran & Kumar)
- In situ: atypical hyperchromatic nuclei at ALL levels of epidermis (full-thickness atypia)
- Invasive (well-differentiated): polygonal cells in orderly lobules, abundant keratinization, keratin pearls (whorled concentric lamellae of keratin - pathognomonic)
- Invasive (poorly differentiated): highly anaplastic cells, foci of necrosis, only abortive single-cell keratinization (dyskeratosis); may need IHC for keratins to confirm
- Variable degrees of differentiation between these extremes
Actinic keratosis (precursor):
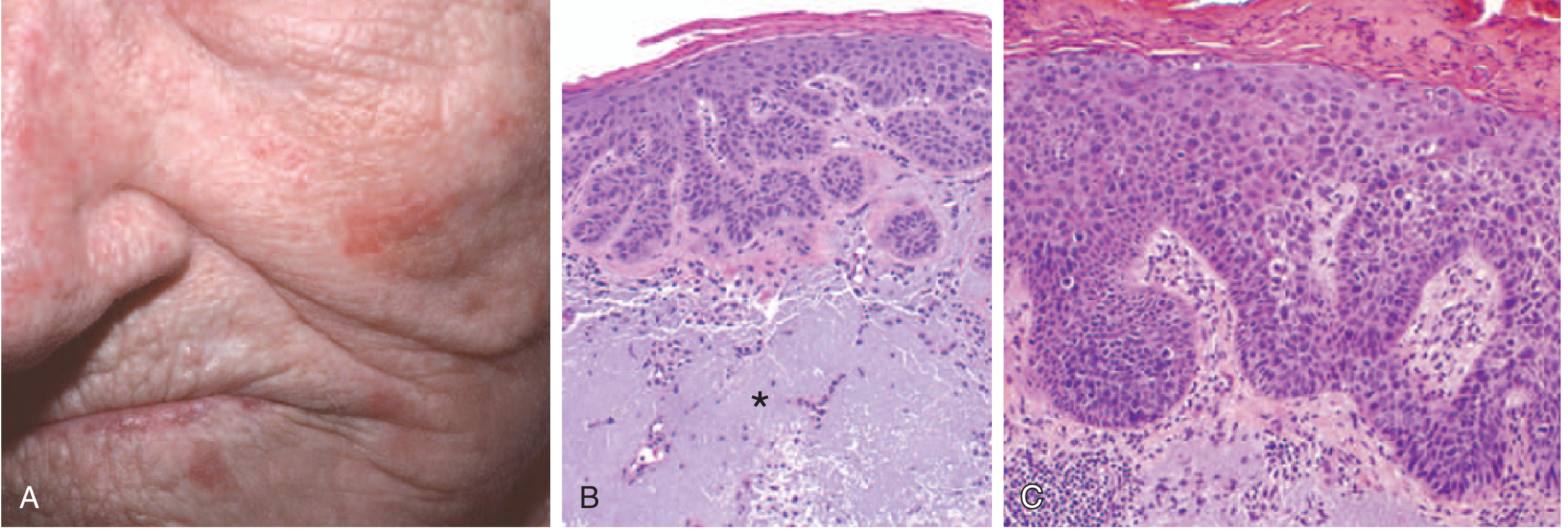
Fig. 22.15 Actinic keratosis and SCC in situ. (A) Red-rough sandpaper lesions on cheek/nose. (B) Basal atypia with hyperkeratosis and dermal solar elastosis (asterisk). (C) Full-thickness epithelial atypia = SCC in situ. (Robbins Basic Pathology)
Clinical Features & Prognosis
- Most discovered small and easily resectable
- ~4-5% have regional lymph node metastases at diagnosis
- Metastasis risk increases with: greater thickness, deeper invasion into subcutis, location near ear/lips
- Actinic keratosis-derived SCC: locally aggressive but slow to metastasize
- Burn scar/ulcer/non-sun-exposed SCC: more aggressive biologically
- Treatment of metastatic disease: high mutational burden → responds well to immune checkpoint inhibitors (first-line for metastatic disease); also sensitive to radiotherapy
HEAD & NECK SCC (HNSCC)
- ~95% of all head and neck cancers are SCC
- 6th most common neoplasm worldwide; >650,000 cases/year globally
Two Distinct Pathogenic Pathways:
1. Carcinogen-associated (tobacco/alcohol):
- Oral cavity (ventral tongue, floor of mouth, lower lip, soft palate, gingiva)
- Mutations: TP53, RAS, NOTCH (same as cutaneous)
- "Field cancerization" concept: multiple independent clones develop throughout mucosa due to chronic carcinogen exposure → risk of synchronous/metachronous second primaries
2. HPV-associated:
- Oropharynx: tonsillar crypts, base of tongue (~90% of tonsillar SCC = HPV+)
- HPV-16 most common subtype (high-risk)
- Spread via orogenital sex
- E6 oncoproteins inhibits p53; E7 inhibits RB
- Overexpress p16 (cyclin-dependent kinase inhibitor) - used as surrogate marker
- Far fewer somatic mutations than tobacco-associated
- Better prognosis than tobacco-associated HNSCC
Additional Regional Risk Factors
- India/SE Asia: betel nut/paan chewing (areca nut + slaked lime + tobacco in betel leaf)
- Lower lip: sunlight and pipe smoking
- In India: chewing tobacco
Morphology
- Early: raised firm pearly plaques or irregular verrucous mucosal thickening, surrounded by leukoplakia/erythroplakia
- Advanced: ulcerated, protruding masses with irregular indurated/rolled borders
- Histology: well-differentiated keratinizing to anaplastic/sarcomatoid
- Degree of keratinization does not correlate with biologic behavior
- Metastasis: cervical lymph nodes (regional); mediastinal lymph nodes, lungs, liver (distant)
LUNG SCC
- Second most common lung carcinoma subtype (after adenocarcinoma, which is now most common)
- Strongly associated with smoking
- Arises centrally near major bronchi from areas of squamous metaplasia → squamous dysplasia → SCC in situ → invasive SCC
- Associated with TP53 and RB mutations
- Often presents with obstructive symptoms, hemoptysis, post-obstructive pneumonia
ESOPHAGEAL SCC
- Common in developing countries and high-risk geographic areas (esophageal cancer belt: Iran, China, parts of Africa)
- Risk factors: alcohol, tobacco, achalasia, Plummer-Vinson syndrome, hot beverages, nitrosamines
- Histology: nests of malignant keratinocytes, glassy cytoplasm, nucleoli, keratin pearls
SUMMARY TABLE - SCC across Sites
| Site | Key RF | HPV? | Key Mutation | Special Feature |
|---|---|---|---|---|
| Skin | UV, immunosuppression | HPV-16 (genital) | TP53, RAS, NOTCH | Keratin pearls; Marjolin's ulcer in scars |
| Oral/Oropharynx | Tobacco, alcohol (carcinogen-assoc); sex (HPV-assoc) | HPV-16 (90% tonsillar) | TP53, RAS, NOTCH | p16 overexpression in HPV+ |
| Larynx/Hypopharynx | Tobacco, alcohol | Variable | TP53 | Field cancerization |
| Lung | Smoking | No | TP53, RB | Central; squamous metaplasia precursor |
| Esophagus | Alcohol, tobacco, achalasia | Rare | TP53 | Geographic clustering |
| Cervix | HPV-16, 18 | HPV (causative) | E6/E7 (p53/RB) | Pap smear for screening |
| Vulva | HPV-16 (younger); lichen sclerosus (older) | HPV-16 | TP53 | Two pathways |
HIGH-YIELD FCPS POINTS
- Keratin pearls (whorled concentric lamellae of keratin) = pathognomonic of well-differentiated SCC
- UV light = most important cause of cutaneous SCC; mutations occur at pyrimidine dimer sites in TP53
- Xeroderma pigmentosum = defective nucleotide excision repair → exceptionally high risk
- Actinic keratosis = premalignant precursor; TP53 mutation is early event
- Marjolin's ulcer = SCC arising in chronic burn scars/ulcers - more aggressive than sun-induced SCC
- HPV-16 = key in oropharyngeal and genital SCC; E6 inhibits p53, E7 inhibits RB; p16 overexpression as IHC marker
- Field cancerization = multiple independent neoplastic clones from chronic mucosal carcinogen exposure
- SCC in situ = full-thickness epithelial atypia (cf. actinic keratosis = only basal layer atypia)
- Metastatic cutaneous SCC responds to immune checkpoint inhibitors (high mutational burden)
- Lung SCC = central, from squamous metaplasia; strongly smoking-associated
- p16 overexpression = surrogate marker for HPV-positive HNSCC; these have better prognosis
Sources: Robbins & Kumar Basic Pathology (Robbins Pathology), p. 891 | Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1057 | Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 685
This is a shared conversation. Sign in to Orris to start your own chat.