Landmark guided blind axillary block techniques
Reading File
Finding Sources
Finding Sources
Searching PubMed
"axillary block" AND "landmark" AND technique
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough, well-structured answer.
Landmark-Guided (Blind) Axillary Brachial Plexus Block
Anatomical Basis
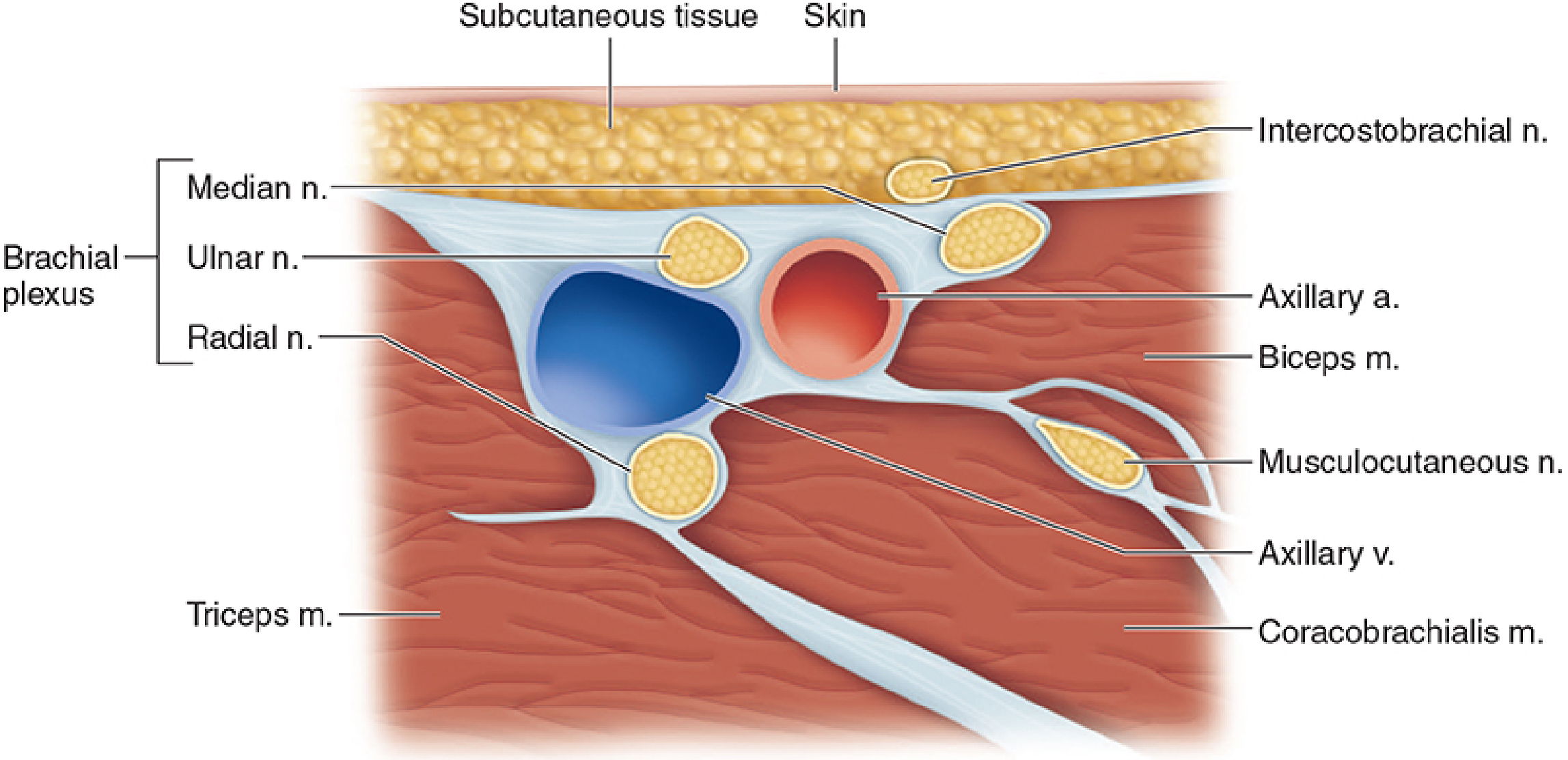
At the axilla, the brachial plexus has already divided into its terminal branches, which travel in close proximity to the axillary artery within a fascial sheath. The axillary artery is the single reliable palpable landmark that anchors all blind techniques. The positions of the nerves relative to the artery are as follows:
- Median nerve - anterior and medial (superior/superficial surface)
- Ulnar nerve - posterior and medial (inferior surface, behind artery)
- Radial nerve - posterior and lateral (posterior to artery, deep)
- Musculocutaneous nerve - anterior and lateral (has typically already left the sheath, running within the coracobrachialis muscle)
A key anatomical challenge is that fascial septa frequently partition the axillary sheath into separate compartments, meaning a single-injection technique often fails to block all nerves reliably. This is the fundamental reason multiple injection approaches were developed.
Patient Positioning
All techniques share the same setup:
- Patient supine
- Arm abducted to 70-90 degrees, externally rotated
- Elbow flexed to 90 degrees, hand resting behind the head or beside the head
- Head turned to the contralateral side
- Axillary artery pulse palpated and marked as high in the axilla as possible, at the level where it emerges from under the pectoralis major
The Four Classical Landmark (Blind) Techniques
1. Perivascular (Single-Injection / Sheath) Technique
The simplest approach. The index finger palpates the axillary artery pulse. A short-bevel needle (22-25G) is inserted at a 30-45° angle just above (superior to) the pulsation, aiming to enter the perivascular sheath. A "fascial click" may be felt as the needle pierces the sheath, and the needle may visibly pulsate with the artery.
- After negative aspiration, inject 20-40 mL of local anesthetic in a single bolus
- Digital compression distally (with a rubber tourniquet or fingers) for 2-3 cm distal to the injection site encourages proximal spread within the sheath toward more proximally branching nerves
- Success depends heavily on recognizing sheath entry and on volume
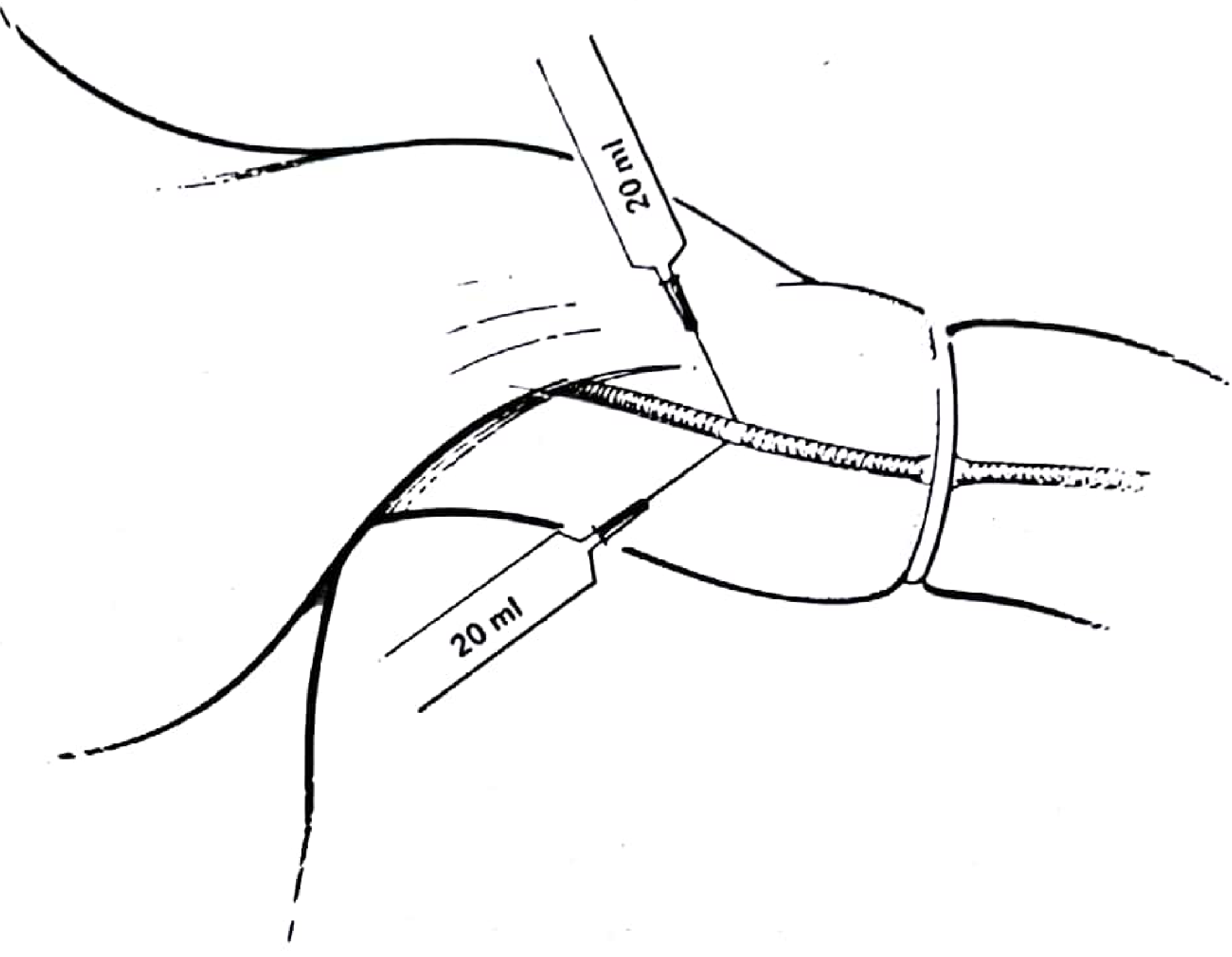
The classic Pye's Surgical-Handicraft technique uses a rubber tourniquet (e.g., Sterivac tubing) applied 2-3 cm distal to the pectoralis major insertion, with two injections of 20 mL each - one immediately above the arterial pulse, and one immediately below it:
2. Transarterial Technique
A reliable blind technique that uses the artery itself as the target landmark.
Steps:
- Palpate and fix the axillary artery between two fingers
- Advance the needle through the skin over the pulse until bright red blood is aspirated freely - confirming arterial entry
- Advance the needle further until blood can no longer be aspirated (needle tip is now posterior to the artery, in proximity to the radial nerve and posterior sheath)
- Inject 15-20 mL of local anesthetic posteriorly
- Withdraw slowly until just anterior to the artery (no blood on aspiration)
- Inject a further 15-20 mL anteriorly (in proximity to the median and ulnar nerves)
The transarterial approach gives reliable two-compartment delivery and was one of the most widely used blind techniques. However, it carries a risk of hematoma, and both Barash and Miller's now note it has been "largely replaced by nerve stimulator (NS) and ultrasound (US)" techniques.
3. Paresthesia Technique
Before nerve stimulators became routine, eliciting paresthesia was the primary method of nerve localization.
Steps:
- Fix the artery and insert the needle above it
- Advance slowly, directing toward each nerve quadrant in turn
- A paresthesia (electric shock-like sensation radiating distally into the hand/fingers) confirms proximity to a specific nerve
- Withdraw very slightly before injecting - never inject into a nerve
- Inject 5-10 mL per nerve
- Redirect to elicit paresthesia from other nerves
Important: Paresthesia-seeking risks direct nerve injury and intraneural injection. Miller's Anesthesia explicitly states this technique "should no longer be used" as a routine approach, given evidence of associated neuropathy.
4. Multiple-Injection Nerve Stimulator (NS) Technique
Although it uses a peripheral nerve stimulator, this is still a landmark-guided technique (the artery remains the primary spatial landmark, with stimulation confirming nerve proximity). This is the preferred "blind" method when ultrasound is unavailable.
Setup:
- 22G, 30-50 mm insulated stimulating needle
- Starting current: 1.0-1.5 mA at 1-2 Hz, 0.1-0.2 ms pulse width
- Reduce to <0.5 mA to confirm adequate proximity before injecting
Needle approach:
- The index and middle fingers of the non-dominant hand straddle the artery just below the intended injection site, both to locate the pulse and to compress the sheath distally
- Insert the needle in a slight cephalad direction
- Use a two-puncture, four-injection approach: above and below the artery
Nerve localization responses:
| Nerve | Motor Response | Location Relative to Artery |
|---|---|---|
| Median | Wrist/finger flexion, forearm pronation | Superior (above artery) |
| Musculocutaneous | Elbow flexion | Superior, lateral (in coracobrachialis) |
| Ulnar | Wrist/finger flexion + ulnar deviation | Inferior (below artery) |
| Radial | Wrist/finger extension, thumb extension | Posterior (behind artery) |
Inject 10-15 mL per nerve after confirming a response at <0.5 mA. The musculocutaneous nerve is often outside the sheath and must be sought separately in the coracobrachialis muscle.
The Musculocutaneous Nerve: Special Consideration
The musculocutaneous nerve departs from the lateral cord proximal to the usual injection site and is frequently NOT blocked by any of the above approaches. It runs within or between the coracobrachialis and biceps brachii muscles, far from the artery.
Blind technique for musculocutaneous block:
- Re-insert the needle into the belly of the coracobrachialis muscle (medial border of biceps, lateral to the artery)
- Fan 5-10 mL of local anesthetic through the muscle belly
- Stimulator response: elbow flexion
Without blocking this nerve, the lateral aspect of the forearm (lateral antebrachial cutaneous territory) will remain unanesthetized.
Intercostobrachial / Medial Brachial Cutaneous Nerves
These nerves are never inside the axillary sheath and must always be blocked separately for upper arm or tourniquet anesthesia. Technique: subcutaneous wheal of 5 mL across the medial aspect of the upper arm from the biceps to triceps.
Volumes and Local Anesthetics
| Approach | Total Volume |
|---|---|
| Perivascular single injection | 30-40 mL |
| Pye's two-injection technique | 40 mL (20 mL + 20 mL) |
| Transarterial (two compartments) | 30-40 mL |
| NS multiple injection | 10-15 mL per nerve (up to 40 mL total) |
Commonly used agents: lidocaine 1-1.5% (with epinephrine 1:200,000), bupivacaine 0.375-0.5%, ropivacaine 0.5%.
Contraindications and Complications
- Local infection at the axilla
- Coagulopathy (hematoma risk, especially with transarterial)
- Pre-existing neuropathy (relative contraindication)
- Hematoma - most common complication (self-limiting; artery is compressible)
- Local anesthetic systemic toxicity (LAST) - axilla is highly vascularized; aspiration before each injection is mandatory
- Neuropathy - risk is highest with paresthesia technique and intraneural injection
- Incomplete block - musculocutaneous and intercostobrachial nerves frequently missed
Indications and Limitations
Ideal for: Surgery distal to the elbow (hand, wrist, forearm), elbow surgery
Limitations:
- Does not block the shoulder or lateral upper arm
- Musculocutaneous, intercostobrachial, and medial brachial cutaneous nerves often spared
- Not ideal for tourniquet pain without supplemental intercostobrachial block
- Inferior to infraclavicular approach for perineural catheter placement (higher infection and dislodgement risk)
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 1890-1892 | Miller's Anesthesia, 10e, p. 6248-6250 | Barash Clinical Anesthesia, 9e, p. 2958-2961 | Pye's Surgical-Handicraft, 22e, p. 107
This is a shared conversation. Sign in to Orris to start your own chat.