Recent acls guidelines
Reading File
Finding Sources
Searching PubMed
"advanced cardiovascular life support" AND "guidelines"
Searching the Web
ACLS guidelines 2025 2026 AHA updates advanced cardiovascular life support
Reading Web Page
https://cpr.heart.org/-/media/CPR-Files/2025-documents-for-c…
Reading File
Searching PubMed
"cardiac arrest" AND "advanced life support" AND "2025 guidelines"
Loading Image
Searching the Web
2025 AHA ACLS adult advanced life support key changes epinephrine amiodarone airway defibrillation post arrest
Here is a comprehensive summary of the 2025 AHA ACLS Guidelines (published October 2025 in Circulation, Vol. 152, Suppl. 2) - the most current version as of mid-2026.
2025 AHA ACLS Guidelines - Key Updates
The 2025 guidelines represent a full comprehensive revision of all AHA resuscitation guidelines, replacing the 2020 edition. A total of 760 specific recommendations were made, including 233 Class I and 451 Class II recommendations.
The official guideline is published as: Part 9: Adult Advanced Life Support, Circulation 2025 (PMID: 41122884)
1. Unified Chain of Survival
- The 2020 guidelines had four separate chains of survival (adult OHCA, adult IHCA, pediatric OHCA, pediatric IHCA).
- 2025 change: A single, unified Chain of Survival framework now applies to all ages and settings (OHCA and IHCA combined).
- Each link now has a dedicated visual symbol; the symbol for high-quality CPR now includes lungs alongside chest compressions, reinforcing the role of breaths, particularly in pediatric and opioid-related arrests.
2. High-Quality CPR - Core Parameters (Unchanged but Reinforced)
| Parameter | Target |
|---|---|
| Compression rate | 100-120/min |
| Compression depth (adults) | 5-6 cm (2-2.4 in) |
| Chest recoil | Full recoil between compressions |
| Compression fraction | >60% (minimize pauses to <10 seconds) |
| Compression:ventilation ratio | 30:2 (without advanced airway) |
| With advanced airway | Continuous compressions at 100-120/min, 1 breath every 6 sec |
3. Defibrillation - New Recommendations
- Standard defibrillation: Early defibrillation remains top priority for shockable rhythms (VF/pVT). Start at 200 J biphasic (or max energy).
- Double Sequential Defibrillation (DSED): The 2025 guidelines state the usefulness of DSED for adults with persistent VF/pVT after 3 or more consecutive shocks has not been established - this is an important update given the DOSE VF trial.
- Vector Change Defibrillation (VCD): A new 2025 recommendation - usefulness of vector change defibrillation for refractory VF/pVT also has not been established (new literature added this as a distinct consideration).
- Resume CPR immediately after each shock, even if ROSC appears to occur.
4. Pharmacology - Updated Guidance
Epinephrine
- Shockable rhythms (VF/pVT): Give epinephrine after the first failed defibrillation attempt, then every 3-5 minutes.
- Non-shockable rhythms (PEA/asystole): Administer epinephrine as early as possible - 2025 explicitly labels early timing as critical (the 2020 guideline did not emphasize this as strongly).
- Dose: 1 mg IV/IO every 3-5 minutes (unchanged).
Antiarrhythmics
- Amiodarone or lidocaine for shock-refractory VF/pVT - used after failed shocks + epinephrine.
- Amiodarone dose: 300 mg IV/IO first dose, then 150 mg if needed.
- Lidocaine alternative: 1-1.5 mg/kg IV/IO.
- Vasopressin has been removed from the cardiac arrest algorithm in prior updates and this remains in 2025.
Opioid-Related Cardiac Arrest
- Expanded emphasis on rapid naloxone administration.
- New recommendation for public access to opioid emergency kits.
5. Airway Management
- No single airway modality is superior: BVM, supraglottic airway (SGA), and endotracheal intubation (ETI) are all acceptable during CPR - evidence shows similar patient outcomes.
- Do not interrupt compressions to place an airway.
- Once advanced airway is in place: continuous compressions + 1 breath every 6 seconds (10 breaths/min).
- Waveform capnography (EtCO2) now plays a central role in monitoring CPR quality - low EtCO2 signals poor compressions or prolonged arrest; target EtCO2 >10-20 mmHg during resuscitation.
- Do not use EtCO2 alone to terminate resuscitation (2025 explicit caution).
6. Monitoring During CPR
- EtCO2 monitoring recommended throughout.
- Arterial diastolic pressure monitoring (when arterial line available): target ≥25 mmHg (infants), ≥30 mmHg (children).
- Point-of-care ultrasound (POCUS): now has explicit guideline support for use in ALS to identify reversible causes.
7. Reversible Causes - The 5 H's and 5 T's
Remains a cornerstone. Search for and treat:
5 H's: Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hypo/hyperkalemia, Hypothermia
5 T's: Tension pneumothorax, Tamponade (cardiac), Thrombosis (coronary - ACS), Thrombosis (pulmonary - PE), Toxins/"Tablets"
8. Post-Cardiac Arrest Care (ROSC)
Updated bundles include:
- Targeted temperature management (TTM): Preventing fever (>37.7°C) remains recommended. The benefit of active cooling to 32-36°C is less certain after the TTM2 trial - 2025 guidelines reflect this uncertainty.
- Coronary angiography: No longer routinely recommended immediately post-arrest without ST-elevation - selective approach based on clinical features.
- Hemodynamic optimization: Target MAP ≥65 mmHg, avoid hypoxia and hypocapnia.
- Neuroprognostication: Multimodal approach; do not make decisions earlier than 72 hours post-ROSC.
9. Team Dynamics and Human Factors
A standout new emphasis in 2025:
- Stronger focus on closed-loop communication.
- Enhanced guidance for the team leader role.
- Clinical debriefing: Both immediate ("hot") and delayed ("cold") debriefing after CPR events is now explicitly recommended.
- New recommendations on resuscitation team composition (in-hospital and out-of-hospital).
10. Terminology Updates
- "Rescue breaths" is no longer used - replaced with "breaths" (for assisted breathing during CPR).
- "Ventilation" is reserved for mechanical respiratory support by professionals.
ACLS Universal Algorithm Overview
The classic Primary-Secondary Survey approach remains the structural framework:
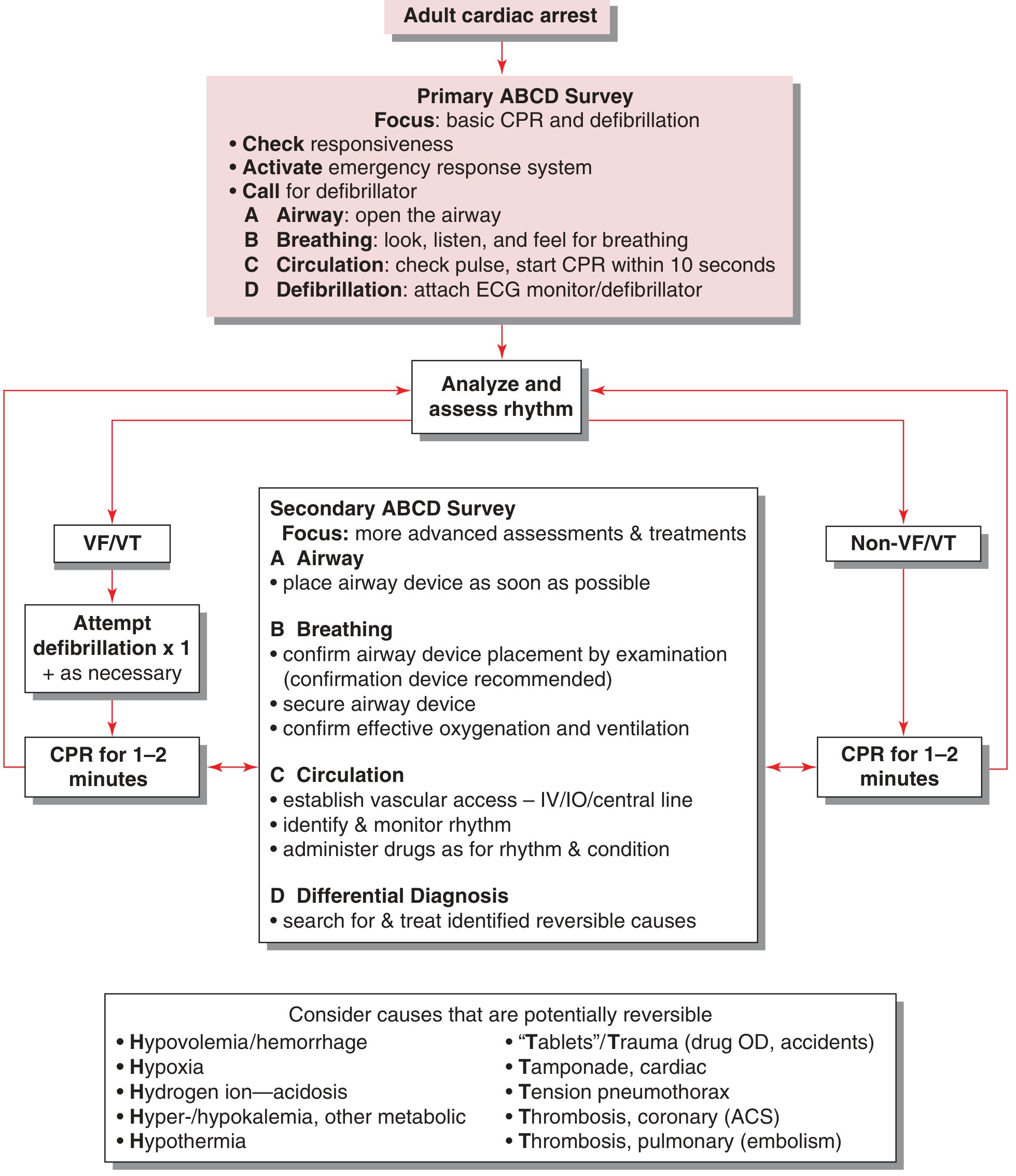
Universal ACLS Algorithm - Tintinalli's Emergency Medicine
Key References
- The full 2025 Adult ALS guidelines: Wigginton et al., Circulation 2025, PMID 41122884 (Part 9 of the 2025 AHA CPR/ECC guidelines)
- AHA 2025 Guidelines Highlights PDF - concise summary from the AHA
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, Chapter 24 (ACLS framework)
This is a shared conversation. Sign in to Orris to start your own chat.