Top 10 ecg disease findgs
Reading File
Finding Sources
Searching Images
ECG findings disease patterns electrocardiogram
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
STEMI ST elevation myocardial infarction ECG pattern
Searching Images
atrial fibrillation ECG irregular rhythm no P waves
Searching Images
Wolff-Parkinson-White delta wave ECG short PR interval
Searching Images
pulmonary embolism S1Q3T3 right heart strain ECG
Searching Images
complete heart block third degree AV block ECG P waves dissociated QRS
Searching Images
Brugada syndrome coved ST elevation V1 V2 right bundle branch block ECG
Searching Images
hyperkalemia peaked T waves ECG sine wave pattern
I now have excellent images and content for all 10 major ECG findings. Here is the comprehensive guide:
Top 10 ECG Disease Findings
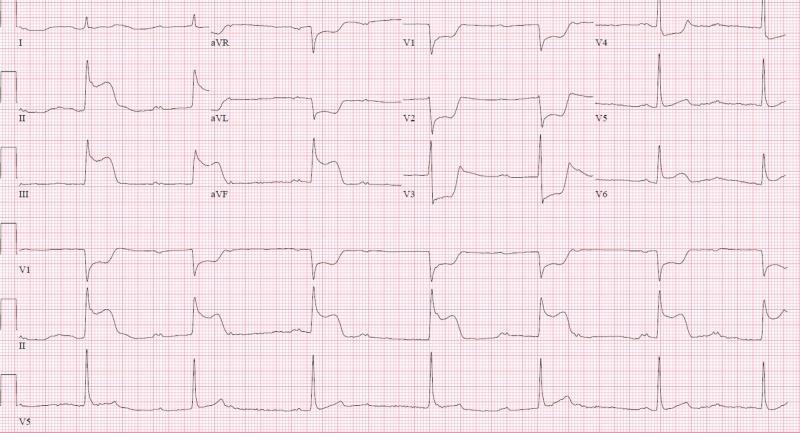
1. 🫀 STEMI — ST-Elevation Myocardial Infarction
Key ECG features:
- ST elevation ≥1 mm in ≥2 contiguous leads
- Convex (coved/tombstone) upward ST morphology
- Reciprocal ST depression in opposite leads
- Later: Q waves >0.04 s, T-wave inversions
Territories:
| Territory | Leads with STE | Culprit Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Inferior | II, III, aVF | RCA |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | V1–V3 depression (mirror) | RCA/LCx |

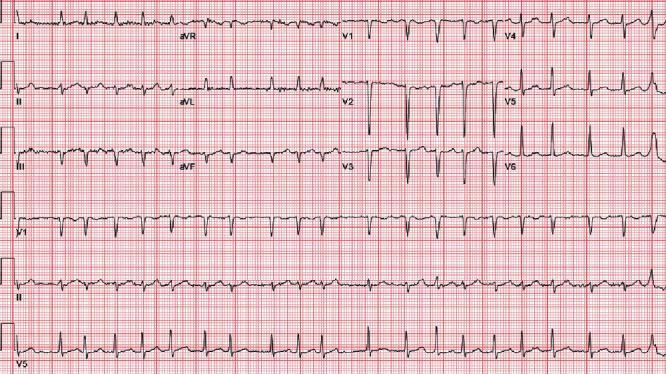
2. 🌀 Atrial Fibrillation (AF)
Key ECG features:
- Irregularly irregular R-R intervals (no pattern)
- Absent P waves — replaced by fine fibrillatory (f) waves, best seen in V1 and II
- Narrow QRS (unless aberrant conduction)
- Ventricular rate varies (60–170+ bpm if uncontrolled)
3. ⚡ Complete (3rd-Degree) AV Block
Key ECG features:
- Complete AV dissociation — P waves and QRS complexes are totally independent
- P waves march at their own rate (faster); QRS at a slower escape rate
- Wide QRS if ventricular escape (infra-nodal); narrow QRS if junctional escape
- Profound bradycardia; requires urgent pacing
4. 🔥 Brugada Syndrome
Key ECG features:
- Type 1 (diagnostic): Coved ST elevation ≥2 mm in V1–V2, descending into inverted T-wave — no isoelectric segment
- Incomplete or complete RBBB morphology in V1–V2
- Occurs spontaneously or unmasked by Na⁺-channel blockers (ajmaline, flecainide)
- Risk of sudden cardiac death from VF
5. 🌪️ Pulmonary Embolism (PE)
Key ECG features:
- Sinus tachycardia (most common finding)
- S1Q3T3 pattern: Deep S in lead I + Q wave in III + T-wave inversion in III
- Right heart strain: T-wave inversions V1–V4, incomplete RBBB
- Right axis deviation
- New RBBB

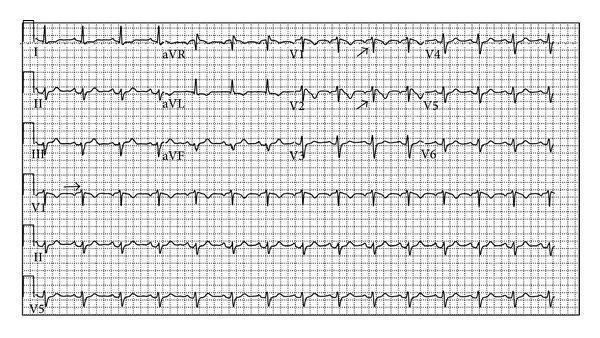
6. ⚠️ Hyperkalemia
Key ECG features (progression with rising K⁺):
| K⁺ Level | ECG Finding |
|---|---|
| 5.5–6.5 mEq/L | Tall, peaked (tented), narrow-based T waves |
| 6.5–7.5 mEq/L | PR prolongation, P-wave flattening/disappearance |
| 7.5–8.0 mEq/L | QRS widening, bundle branch block patterns |
| >8.0 mEq/L | Sine-wave pattern, VF/asystole risk |

7. 🏔️ Wolff-Parkinson-White (WPW) Syndrome
Key ECG features (classic triad):
- Short PR interval (<120 ms)
- Delta wave — slurred upstroke at start of QRS
- Wide QRS (>120 ms) due to pre-excitation
- Secondary ST-T changes (discordant from delta)
- Risk: AF with rapid conduction → VF (avoid AV nodal blockers)
Localizing the accessory pathway: dominant R in V1 = left-sided pathway; negative delta in inferior leads = posteroseptal

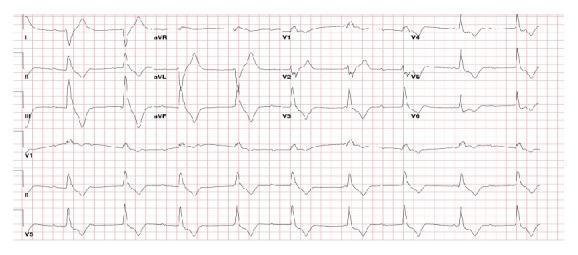
8. 🫁 Pericarditis
Key ECG features (evolve through 4 stages):
- Stage 1: Diffuse saddle-shaped (concave up) ST elevation in most leads (except aVR, V1); PR segment depression (most sensitive sign)
- Stage 2: ST normalizes, T waves flatten
- Stage 3: Diffuse T-wave inversions
- Stage 4: ECG normalizes
- Electrical alternans when pericardial effusion present → consider tamponade
9. 📈 Left Ventricular Hypertrophy (LVH)
Key ECG features:
- Sokolow-Lyon criterion: S in V1 + R in V5 or V6 ≥35 mm
- Cornell criterion: R in aVL + S in V3 >28 mm (men) / >20 mm (women)
- LV strain pattern: ST depression + T-wave inversion in lateral leads (I, aVL, V5–V6)
- Left axis deviation
- Associated with HTN, aortic stenosis, HCM
10. 🌊 Ventricular Tachycardia (VT)
Key ECG features:
- Wide complex tachycardia (QRS ≥120 ms) at rate >100 bpm
- AV dissociation (independent P waves) — pathognomonic
- Fusion beats and capture beats — confirm VT
- Concordance in precordial leads (all positive or all negative)
- Brugada criteria and Vereckei criteria help differentiate from SVT with aberrancy
| Feature | Favors VT | Favors SVT + Aberrancy |
|---|---|---|
| QRS width | >140 ms (RBBB), >160 ms (LBBB) | Narrower |
| Axis | Extreme right or NW (−90 to ±180°) | Normal/left |
| AV dissociation | Present | Absent |
| Precordial concordance | Present | Absent |
Quick Reference Summary
| # | Condition | Hallmark ECG Sign |
|---|---|---|
| 1 | STEMI | ST elevation + reciprocal depression in contiguous leads |
| 2 | Atrial Fibrillation | Irregularly irregular, no P waves |
| 3 | 3rd-Degree AV Block | Complete P-QRS dissociation |
| 4 | Brugada Syndrome | Coved ST elevation V1–V2 |
| 5 | Pulmonary Embolism | S1Q3T3 + RV strain |
| 6 | Hyperkalemia | Peaked T waves → sine wave |
| 7 | WPW | Short PR + delta wave + wide QRS |
| 8 | Pericarditis | Diffuse saddle ST elevation + PR depression |
| 9 | LVH | High voltage + lateral strain pattern |
| 10 | Ventricular Tachycardia | Wide complex tachycardia + AV dissociation |
Sources: ROSEN's Emergency Medicine; Harrison's Principles of Internal Medicine 22E; Tintinalli's Emergency Medicine; Goldman-Cecil Medicine — ECG findings sections
This is a shared conversation. Sign in to Orris to start your own chat.