Conization
Reading File
Finding Sources
Finding Sources
Searching PubMed
cervical conization CIN treatment outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete overview of cervical conization drawn from authoritative gynecology and surgical textbooks.
Conization of the Cervix
Definition
Conization is the surgical excision of a cone-shaped wedge of tissue from the cervix uteri. To be considered adequate, the specimen must include the entire transformation zone with the squamocolumnar junction (SCJ) and the entire lesion surrounded by uninvolved margins. It serves as both a diagnostic and therapeutic procedure.
- Pfenninger and Fowler's Procedures for Primary Care, p. 935-937
- Berek & Novak's Gynecology, p. 865
Types of Conization
| Method | Setting | Notes |
|---|---|---|
| Cold-Knife Conization (CKC) | Operating room (general/regional anesthesia) | Gold standard; least tissue artifact; best histologic quality |
| LEEP Conization | Office/outpatient | Simpler, faster; uses heated wire loop; equivalent short- and long-term outcomes |
| Laser Conization | Specialized centers | Less common; tissue quality intermediate |
CKC is the reference standard against which all outpatient techniques are compared. A "cold knife" refers to a surgical blade, distinguishing it from the older "hot-wire" cone or the LEEP.
Indications
Diagnostic Indications
- Inadequate colposcopic evaluation (entire lesion or TZ/SCJ not visualized)
- Lesion extends into the endocervical canal beyond colposcopic view
- Positive endocervical curettage (ECC) - dysplasia or cancer found
- Significant discrepancy between cytology, colposcopic impression, and biopsy (e.g., Pap smear at least two grades worse than biopsy)
- Inability to exclude invasive cancer on colposcopy
- CIN 3 or AGC-AIS (adenocarcinoma in situ) confirmed on biopsy
Therapeutic Indications
- Cytology or biopsy suggests microinvasive carcinoma (to rule out frank invasion)
- High-grade dysplasia (CIN 2-3) >2 cm or involving more than 2 quadrants
- Lesion too large for cryotherapy or cryo is contraindicated
- Markedly irregular cervical surface crevices that cryotherapy cannot reach
- Glandular involvement on biopsy
- Lesion extends >5 mm into the os
- Patient unlikely to comply with follow-up after less definitive treatment
Contraindications
Absolute:
- Known frank invasive cervical/endocervical carcinoma (microinvasive cancer is NOT an absolute contraindication - conization is actually required to rule out frank invasion)
- Contraindications to general or regional anesthesia
- Unstable medical conditions
Relative:
- Unstable bleeding disorders / coagulopathy
- Active cervicitis / heavy menses (increased bleeding risk)
- Pregnancy (see note below)
- Diethylstilbestrol (DES) exposure in utero
- <12 weeks postpartum
- Preexisting short cervix (consider referral)
Pregnancy note: Not an absolute contraindication, but only a well-trained physician capable of managing complications should operate. Fetal loss rate is ~10% (from membrane rupture, preterm labor, hemorrhage), and postoperative hemorrhage rate is ~30%.
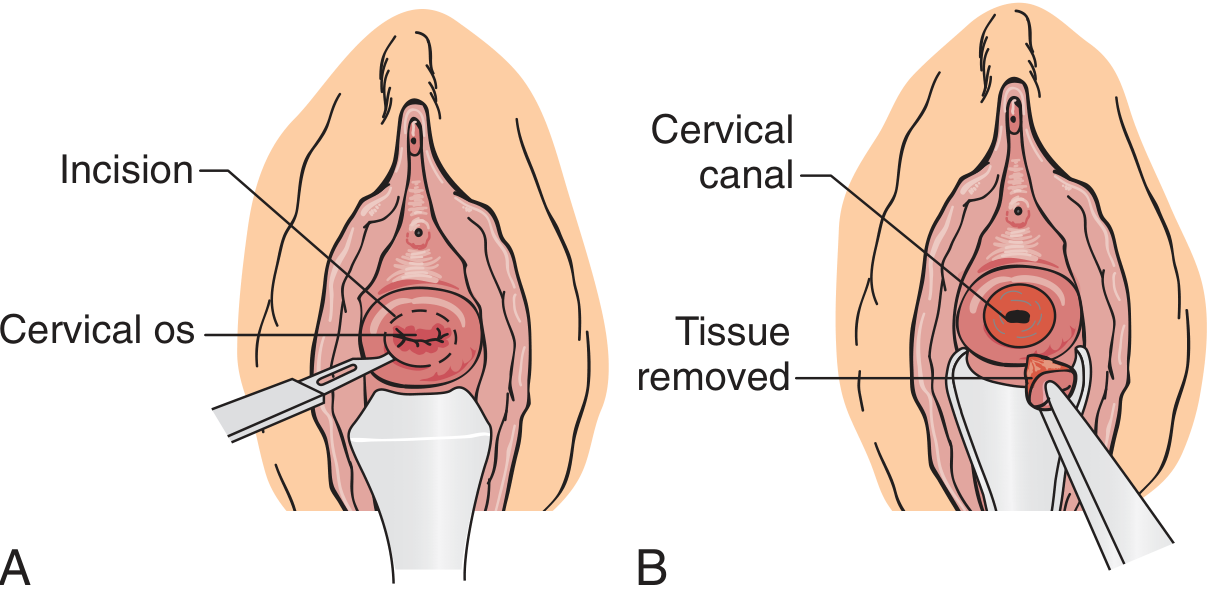
Procedure (Cold-Knife Conization)
Key steps:
- Anesthesia - general, regional, or local (intrastromal) anesthesia; drain bladder
- Lesion demarcation - apply full-strength Lugol's solution (iodine-negative areas = abnormal) or acetic acid + green filter colposcopy to outline the transformation zone
- Hemostasis - circumferentially infiltrate cervical stroma with vasopressin 20 U in 20 mL normal saline; figure-of-eight retention sutures at 3 and 9 o'clock to ligate descending branches of the uterine artery (CKC)
- Sound the uterus - assess canal position and size
- Incision - begin at 6 o'clock (so blood runs away from the incision line), angle the blade centrally toward the endocervical canal; excise outside the Lugol's-negative/acetowhite area
- Specimen orientation - place a marking suture at 12 o'clock; grasp with Allis clamps to maintain orientation
- Endocervical curettage (ECC) - performed above the cone biopsy
- Hemostasis - running locked suture, Sturmdorf stitch, or hemostatic agents (Surgicel, Gelfoam)
Cone shape varies by age:
- Premenopausal: broad base, wide angle at top (ectocervical lesions predominate)
- Postmenopausal: long and narrow, acute apex (SCJ has receded into the canal; endocervical lesions more likely)
Pathologic Assessment and Margins
- Positive margins significantly increase recurrence risk after conization
- Endocervical gland involvement is predictive of recurrence: 23.6% with gland involvement vs. 11.3% without
- If ectocervical margins show only dysplasia: follow closely; repeat cone not routinely indicated (lesion often resolves during healing)
- If ECC above the excisional site is positive with high-grade lesion: repeat conization should be considered
- Adenocarcinoma in situ (AIS): high rate of coexisting squamous lesions (~58% in one series); margins are less reliable and hysterectomy is often recommended after conization
Outcomes: CKC vs. LEEP vs. Laser
A prospective study comparing the three modalities showed no significant difference in recurrence of dysplasia or in pregnancy outcomes (Berek & Novak's). Short-term results are also equivalent. LEEP is the simpler technique and can be done in an office setting.
Complications
| Complication | Notes |
|---|---|
| Intraoperative / postoperative hemorrhage | Most common; managed with sutures, cautery, or hemostatic agents |
| Cervical stenosis | Risk of cervical incompetence (obstetric risk) |
| Infection | Pelvic cellulitis or cervicitis (rare) |
| Infertility | Loss of mucus-producing endocervical glands |
| Bladder/rectal injury | Rare; risk increases with vaginal atrophy and shallow fornices |
| Positive margins / positive ECC | Management as above |
| Missing the lesion | Rare |
| Pregnancy-specific | Fetal loss ~10%, postoperative hemorrhage ~30% |
Post-Procedure Management
-
Follow-up at 4-6 weeks
-
Avoid intercourse, douching, and tampons until healing confirmed
-
Report fever, excessive bleeding, or purulent discharge
-
First follow-up Pap smear at 3-4 months if margins are clear
-
Pfenninger and Fowler's Procedures for Primary Care, p. 937
-
Berek & Novak's Gynecology, p. 865
-
Sabiston Textbook of Surgery, p. 2793
Recent Evidence (2024-2026)
A 2025 Cochrane systematic review on HPV vaccination after conization (PMID: 40919695) examined whether post-conization HPV vaccination reduces recurrence - this is an active area of research that may influence post-procedure protocols. A 2024 systematic review on high-grade CIN treatment in Europe (PMID: 39002399) also provides updated data on recurrence risk and HPV genotype distribution following excisional treatments.
This is a shared conversation. Sign in to Orris to start your own chat.