what are the extra nasopharyngeal manifestations of nasopharyngeal angiofibroma? Discuss various surgical options available for complete excision of tumor in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
"juvenile nasopharyngeal angiofibroma" AND surgery
Searching the Web
nasopharyngeal angiofibroma extranasopharyngeal extension surgical approaches RGUHS ENT 20 marks
Reading File
Finding Sources
Searching PubMed
"nasopharyngeal angiofibroma" AND "endoscopic" AND excision
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC3431533
JUVENILE NASOPHARYNGEAL ANGIOFIBROMA (JNA)
Extranasopharyngeal Manifestations and Surgical Options for Complete Excision
20-Mark Answer - RGUHS Pattern
INTRODUCTION
Juvenile Nasopharyngeal Angiofibroma (JNA) is a benign but locally aggressive, highly vascular fibrous tumor occurring almost exclusively in adolescent males between 10-25 years. It arises from the fibrovascular stroma at the pterygopalatine fossa / sphenopalatine foramen at the base of the medial pterygoid plate. Though histologically benign, its aggressive growth through foramina and fissures of the skull base makes it a surgical challenge of the highest order.
(Sources: Cummings Otolaryngology, 7th ed.; Scott-Brown's Otorhinolaryngology, Vol.1; KJ Lee's Essential Otolaryngology)
PART I: EXTRANASOPHARYNGEAL MANIFESTATIONS (8 Marks)
A. Pathways of Spread
The tumor originates at the sphenopalatine foramen and spreads along pre-formed pathways following foramina and fissures:
ORIGIN: Sphenopalatine Foramen / Pterygoid Process Base
|
┌───────────────┼───────────────────────┐
↓ ↓ ↓
MEDIAL SUPERIOR LATERAL
SPREAD SPREAD SPREAD
↓ ↓ ↓
Nasopharynx Sphenoid Sinus Pterygopalatine
Nasal Cavity Floor of Sphenoid Fossa (PPF)
(via SPF) (via Vidian Canal) ↓
↓ Pterygomaxillary
Sella Turcica Fissure
(advanced) ↓
Infratemporal Fossa
↓
┌──────────┴──────────┐
↓ ↓
Orbit (via Parapharyngeal
IOF/SOF) Space
↓
Middle Cranial Fossa
(via IFS / Maxillary N.)
Cavernous Sinus
Anterior Cranial Fossa
(via Ethmoid - rare)
(Cummings Otolaryngology, 7th ed., Fig. 50.7)
B. Extranasopharyngeal Manifestations by Region
1. PARANASAL SINUSES
- Maxillary sinus - most common extranasopharyngeal site; anterior bowing of posterior wall = Holman-Miller sign (pathognomonic on X-ray/CT)
- Sphenoid sinus - via floor erosion or vidian canal
- Ethmoid sinus - uncommon; indicates anterior skull base encroachment
- Frontal sinus - rare, via anterior ethmoid spread
Clinical features: Facial fullness, cheek swelling, sinusitis, nasal discharge
2. INFRATEMPORAL FOSSA (ITF)
- Via pterygomaxillary fissure - most important lateral extension
- Tumor may completely fill the ITF in advanced cases
- Clinical features: Cheek swelling/bulge, trismus (pterygoid muscle involvement), palpable mass in temporal fossa
- Bone: permeative intraosseous growth within cancellous bone of greater wing of sphenoid
(Cummings, Fig. 50.7C,E)
3. ORBIT
- Via inferior orbital fissure (IOF) - from PPF
- Via superior orbital fissure (SOF) - advanced spread
- Clinical features: Proptosis, diplopia, visual disturbance, chemosis
- Optic canal involvement can cause visual loss
(Cummings Fig. 50.7F)
4. INTRACRANIAL EXTENSION
- Via inferior/superior orbital fissure or foramen rotundum (along maxillary nerve) to parasellar/cavernous sinus region
- Via middle cranial fossa floor erosion of greater sphenoid wing
- Via anterior cranial fossa through ethmoid (rare)
- Transdural growth is very rare despite intracranial extension
- Clinical features: Headache, cranial nerve palsies (III, IV, V, VI), visual field defects, raised ICP signs
(Cummings, Scott-Brown)
5. PARAPHARYNGEAL SPACE
- Posterior extension from sphenopalatine region
- Clinical features: Unilateral tonsillar/pharyngeal mass bulge, dysphagia, change in voice (uncommon)
6. NASAL CAVITY (Extranasopharyngeal in same region)
- Anterior extension into nasal cavity, presenting as visible mass at anterior nares
- May present as bilateral involvement of maxillary sinuses and bilateral choanal involvement
7. CHEEK / SOFT TISSUE
- Anterior extension through posterior maxillary wall
- Clinical features: Facial swelling over cheek (Frog-face deformity in large tumors)
8. MIDDLE EAR / EUSTACHIAN TUBE
- Though not direct extension, tubal orifice involvement leads to serous otitis media / conductive hearing loss (seen in early primary nasopharyngeal tumor)
C. Staging Systems (Chandler, Sessions/Radkowski, Andrews/Fisch)
The extent of extranasopharyngeal spread forms the basis of all staging systems:
| Stage | Chandler (1984) | Andrews/Fisch | Radkowski |
|---|---|---|---|
| I | Nasopharynx only | Nasopharynx, nasal cavity | Nasopharynx, nasal cavity |
| II | Extends to nasal cavity, sphenoid | PPF, maxillary sinus, ethmoid, sphenoid | PPF/maxillary ± sphenoid |
| IIIa | Maxillary sinus, ethmoid, orbit, ITF, cheek, cavernous sinus | Orbit, ITF - no residual bone erosion | Orbit, ITF |
| IIIb | Same | Orbit, ITF - with residual bone erosion (sella, skull base) | As IIIa + intracranial extradural |
| IV | Intracranial | Intradural ± cavernous sinus | Intracranial with/without ICA encasement |
(Cummings Otolaryngology, 7th ed., Staging section)
MRI Diagram: Patterns of Growth
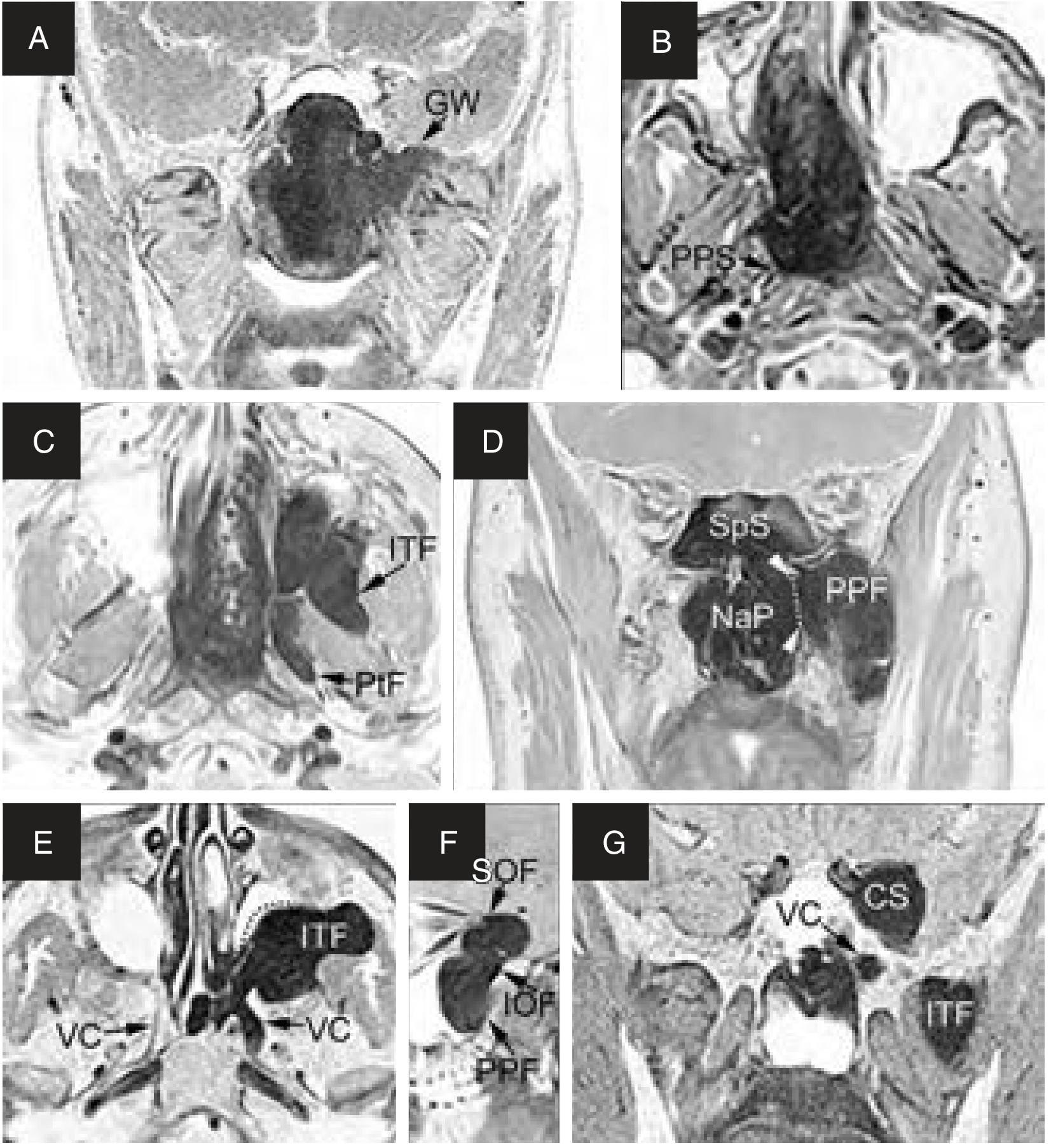
Fig. 50.7 from Cummings Otolaryngology - Patterns of growth of JNA: (A) Intraosseous growth in greater wing (GW), (B) Posterior extension to parapharyngeal space (PPS), (C) Pterygoid fossa (PTf) and ITF invasion, (D) Medial spread to NaP/SpS via SPF and lateral to PPF, (E) ITF filling with vidian canal (VC) involvement, (F) Orbital spread via IOF/SOF, (G) Cavernous sinus (CS) and ITF involvement.
CT showing Holman-Miller Sign

CT showing widening of left sphenopalatine foramen from a juvenile angiofibroma (Cummings Fig. 95.1)
PART II: SURGICAL OPTIONS FOR COMPLETE EXCISION (12 Marks)
A. General Principles of Surgery (applicable to ALL approaches)
"Selection of appropriate approach for adequate exposure, vascular control, and dissection in subperiosteal plane" - PMC 3431533
- Preoperative workup: CT (bone detail), MRI (soft tissue, intracranial), MRA/DSA (vascular supply)
- Preoperative embolization: 24-48 hours before surgery; PVA particles or NBCA/Onyx; reduces intraoperative hemorrhage
- Controlled hypotension anesthesia: target MAP 60-70 mmHg
- Blood grouping and crossmatch: have blood ready
- Subperiosteal dissection plane throughout
- Primary vascular control before tumor delivery
B. Flowchart: Selection of Surgical Approach
JUVENILE NASOPHARYNGEAL ANGIOFIBROMA - CONFIRMED
|
↓
Staging (CT + MRI + MRA/DSA)
|
┌────────────────┴────────────────────┐
↓ ↓
Stage I / II Stage III / IV
(Limited to NP, (ITF, Orbit,
nasal cavity, Intracranial
PPF, sphenoid) extension)
| |
┌────┴────┐ ┌──────────┴──────────────┐
↓ ↓ ↓ ↓ ↓
Endoscopic Transpalatal Transmaxillary Midfacial Infratemporal
Endonasal (limited (Caldwell-Luc Degloving Fossa Approach
(Gold NP disease) + medial ± LeFort I (Fisch Type C)
Standard maxillectomy) + Neurosurgery
Stage I/II)
↓ ↓
Combined endoscopic Facial Translocation
+ Sublabial / Caldwell-Luc (Stage IV with ICA
for medial ITF extension involvement)
C. DETAILED SURGICAL APPROACHES
1. ENDOSCOPIC ENDONASAL APPROACH (EEA)
Indications: Stage I, II, and selected Stage IIIa (medial ITF extension)
Steps:
- Patient supine, head elevated 30°; topical decongestant (1:10,000 adrenaline) soaked pledgets
- Wide middle meatal antrostomy + posterior ethmoidectomy for exposure
- Sphenopalatine foramen identified posterior to middle turbinate
- Sphenopalatine artery clipped/coagulated lateral to tumor - critical first step
- Posterior maxillary wall removed (if needed) - Caldwell-Luc port
- Tumor dissected in subperiosteal plane using suction bipolar electrocautery, Freer elevators
- Vidian artery followed and clipped if tumor extends along vidian canal
- Tumor delivered through nasal cavity or mouth
Advantages (Scott-Brown, Cummings): No facial scar, direct visualization, lower morbidity, shorter hospital stay, better cosmesis
Disadvantages: Limited lateral access, steep learning curve, major hemorrhage risk without experience
Recurrence: ~8-15% (Cummings - Hofmann series, 21 patients, 52 months follow-up)
Recent advance: Three-surgeon, six-handed technique (Asian J Neurosurg, 2017) for extended endoscopic access
2. TRANSPALATAL APPROACH (Wilson's Approach)
Indications: Stage I - tumor confined to nasopharynx; older/historical approach
Steps:
- Patient supine, head extended; Dingman's mouth gag
- U-shaped palatal incision (Wilson) with base at soft palate OR transverse midline incision
- Hard palate mucoperiosteally elevated; palatine vessels preserved if possible
- Posterior hard palate and vomer may be removed for exposure
- Tumor visualized in nasopharynx, dissected under direct vision
- Hemostasis achieved; palate replaced and sutured in layers
Advantages: Direct access to nasopharynx, no facial scar
Disadvantages: Very limited exposure - cannot access PPF, ITF; risk of palatal fistula, palate shortening, VPI (velopharyngeal incompetence), dental injury in children
Note: Largely replaced by endoscopic approaches in modern practice; still used in resource-limited settings
(Source: Dhingra Diseases of Ear, Nose and Throat; Hazarika ENT; PMC 3431533 - 43 cases 1980-1990 → 8 cases 1990-2009)
3. LATERAL RHINOTOMY + MEDIAL MAXILLECTOMY
Indications: Stage II-IIIa; tumors with maxillary sinus, nasal cavity, limited ITF extension
Steps:
- Lynch incision - begins at medial canthus, curves down alongside nose to level of alar base
- Periosteum elevated; nasal bone, frontal process of maxilla, lacrimal bone exposed
- Anterior maxillary wall opened; medial maxillectomy performed
- Posterolateral nasal wall removed to expose pterygopalatine and infratemporal fossa
- Internal maxillary artery/sphenopalatine artery ligated
- Tumor excised under direct vision
- Wound closed; nasal packing
Advantages: Direct access to nasal cavity, maxillary sinus, PPF
Disadvantages: Facial scar (cosmetically unacceptable in teenagers), limited ITF access
Modifications: Weber-Ferguson incision (adds sublabial extension) for greater access
4. MIDFACIAL DEGLOVING APPROACH
Indications: Stage IIIa - large tumors with maxillary, PTF, limited ITF extension; avoids facial scars
Steps (as described in PMC 3431533 and Cummings):
- Bilateral intercartilaginous incisions in nasal vestibule + bilateral sublabial incisions connected across the midline
- Facial soft tissue (cheek flap) elevated off maxilla bilaterally - complete facial degloving
- Rhinoplasty incisions and lateral osteotomies NOT required (modification of Casson)
- Excellent bilateral access to nasal cavities, maxillary sinuses, pterygopalatine fossa
- Posterior maxillary wall removed; tumor dissected
- Combined with medial maxillectomy if needed (Fig. 21 - Atlas of Otolaryngology)
- Facial flap replaced; no skin sutures needed (intranasal and sublabial only)
Advantages: No facial scar, excellent bilateral access, good for large tumors, easy to combine with other approaches
Disadvantages: Hypoesthesia of upper lip (infraorbital nerve), temporary alar stenosis, limited lateral ITF access
Author's note (PMC 3431533): "Most useful considering surgical exposure, duration, cosmetic outcome and morbidity"
5. TRANSMAXILLARY / CALDWELL-LUC APPROACH
Indications: Stage IIIa tumors with lateral infratemporal extension; good complementary approach
Steps:
- Sublabial incision in upper buccal sulcus above upper canine
- Anterior maxillary wall opened (canine fossa)
- Posterior maxillary wall removed to access pterygopalatine and infratemporal fossa
- Tumor dissected laterally; internal maxillary artery approached and ligated
- Combined with endoscopic or transpalatal for comprehensive access
Advantages: No skin scar, good lateral access
Disadvantages: Limited superiorly, risk of dental injury in growing maxilla
6. INFRATEMPORAL FOSSA APPROACH (FISCH TYPE C)
Indications: Stage IIIb / IV - large tumors with extensive ITF, skull base, parasellar involvement; ICA encasement
Description by Andrews, Fisch, and colleagues (Laryngoscope, 1989):
Steps:
- Pre-auricular (hemicoronal) + temporal incision
- Zygomatic arch osteotomy + temporalis muscle elevation
- Infratemporal fossa exposed widely; mandibular condyle may be displaced
- Middle fossa dura exposed; internal carotid artery identified and controlled in petrous segment
- Tumor dissected from cavernous sinus, parasellar region, ICA
- Combined neurosurgical craniotomy if transdural extension present
Advantages: Best access for advanced Stage IIIb-IV; ICA control possible
Disadvantages: Complex surgery, long operative time, risk of facial nerve injury, CN deficits, trismus (temporal muscle atrophy), significant morbidity
Fisch classification indication: Class IIIb-IV
(Source: Scott-Brown Vol.2 - Infratemporal Fossa chapter; Andrews JC, Fisch U, Laryngoscope 1989)
7. LEFORT I OSTEOTOMY APPROACH
Indications: Stage III with posterior maxillary/pterygopalatine/inferior skull base extension; good alternative to midfacial degloving for deep lesions
Steps:
- Sublabial incision; maxillary osteotomy at LeFort I level
- Maxilla down-fractured and displaced anteriorly - "trapdoor" access
- Excellent exposure of nasopharynx, posterior choanae, pterygopalatine fossa
- Tumor excised; maxilla plated back in anatomical position
Advantages: Excellent posterior exposure, no facial scar, rigid plate fixation allows predictable outcome
Disadvantages: Dental occlusion disruption, growth disturbance in young children, maxillary devascularization risk
de Mello-Filho series: 40 patients - effective even with CNS invasion
8. FACIAL TRANSLOCATION APPROACH
Indications: Stage IV - tumors requiring access to middle/anterior cranial fossa, cavernous sinus, ICA, and orbit simultaneously
Steps (as described by Cummings):
- Weber-Ferguson incision + coronal extension for frontotemporal craniotomy
- Midface osteotomies - nasal, orbital-maxillary, zygomatic arch
- Facial soft tissue rotated laterally as single osteoplastic unit
- Underlying maxilla rotated laterally after osteotomies
- Complete exposure of orbit, anterior/middle skull base, cavernous sinus, ICA
- Tumor excised; osteotomies plated; facial flap replaced
Advantages: Unparalleled exposure for Stage IV; hemostatic options for catastrophic ICA bleeding
Disadvantages: Maximal morbidity, CSF leak risk, CN palsies, lengthy surgery
9. TRANSCERVICAL APPROACH
Indications: Parapharyngeal extension, inferior extension into neck
Rare approach: Used in conjunction with others; reported in 2 cases (PMC 3431533)
D. Summary Table: Approach vs. Stage
┌─────────────────────────────────────────────────────────────────────┐
│ SURGICAL APPROACH SELECTION TABLE FOR JNA │
├─────────────────────────┬──────────────────┬────────────────────────┤
│ APPROACH │ STAGE │ ACCESS PROVIDED │
├─────────────────────────┼──────────────────┼────────────────────────┤
│ Endoscopic Endonasal │ I, II, IIIa* │ NP, NC, PPF, SpS, │
│ (EEA) │ (*medial ITF) │ medial ITF │
├─────────────────────────┼──────────────────┼────────────────────────┤
│ Transpalatal │ I │ NP only │
├─────────────────────────┼──────────────────┼────────────────────────┤
│ Lateral Rhinotomy │ II-IIIa │ NC, Maxillary, PPF │
├─────────────────────────┼──────────────────┼────────────────────────┤
│ Midfacial Degloving │ II-IIIa │ Bilateral NC, Maxillary│
│ ± Medial Maxillectomy │ │ PPF, limited ITF │
├─────────────────────────┼──────────────────┼────────────────────────┤
│ Transmaxillary │ IIIa │ Maxillary, lateral PPF │
│ (Caldwell-Luc) │ │ ITF │
├─────────────────────────┼──────────────────┼────────────────────────┤
│ LeFort I Osteotomy │ II-IIIb │ NP, posterior PPF, │
│ │ │ inferior skull base │
├─────────────────────────┼──────────────────┼────────────────────────┤
│ Infratemporal Fossa │ IIIb-IV │ Extensive ITF, skull │
│ Approach (Fisch Type C) │ │ base, parasellar, ICA │
├─────────────────────────┼──────────────────┼────────────────────────┤
│ Facial Translocation │ IV │ Complete skull base, │
│ │ │ cavernous sinus, orbit │
└─────────────────────────┴──────────────────┴────────────────────────┘
NC=Nasal Cavity; NP=Nasopharynx; PPF=Pterygopalatine Fossa;
SpS=Sphenoid Sinus; ITF=Infratemporal Fossa
(Sources: KJ Lee's Essential Otolaryngology; Cummings; Atlas of Otolaryngology)
E. PREOPERATIVE EMBOLIZATION - Important Surgical Adjunct
Embolization is performed 24-48 hours before surgery.
Agents used:
- Polyvinyl alcohol (PVA) particles - transarterial
- NBCA (N-butyl cyanoacrylate) liquid embolic
- Onyx - direct percutaneous puncture technique; best devascularization
- Coils, balloons
Benefits (Scott-Brown; Diaz et al., Laryngoscope 2023 - meta-analysis PMID 36789781):
- Reduces intraoperative blood loss significantly
- Improves tumor border delineation
- Facilitates complete resection
Caution: ICA supply in 35.6% of advanced lesions (systematic review, 828 cases); increases risk of neurological complications with transarterial embolization → direct puncture/Onyx preferred
Controversy: Some centers now omit preoperative embolization for Stage I/II endoscopic cases, citing adequate hemostasis with suction bipolar and sphenopalatine artery ligation
F. POSTOPERATIVE CONSIDERATIONS
- Recurrence rate: 6-35% depending on stage; higher with intracranial extension
- Follow-up: MRI with contrast (preferred over CT for follow-up - Cummings)
- Spontaneous regression reported post-puberty (androgen-dependent growth)
G. NON-SURGICAL MODALITIES
Radiotherapy:
- Dose: 30-36 Gy (external beam)
- Indications: Unresectable Stage IV, residual disease post-surgery, recurrence with intracranial ICA involvement
- Concerns: Malignant transformation (rare), growth plate disruption in children, radiation-induced malignancy
Anti-androgen therapy (Flutamide):
- Neoadjuvant to reduce tumor volume before surgery
- Used pre-pubertally or in early puberty (Sitenga et al., Int J Dermatol, 2022 - PMID 34748211)
- Evidence: Limited; not standard of care
RECENT ADVANCES (2021-2026)
Based on the most recent literature:
- Expanded Endoscopic Endonasal Approach (EEA) - now the standard for Stage I-IIIa; even medial infratemporal fossa invasion is no longer a contraindication (Cummings, Hofmann series)
- Coblation-assisted endoscopic excision - reduces bleeding, improves visualization (Chen F et al., 2024, PMID 38858116)
- Preoperative embolization - meta-analysis evidence (Diaz et al., Laryngoscope 2023, PMID 36789781; Segal et al., J Laryngol Otol 2026, PMID 42087760): Embolization beneficial in advanced-stage disease; benefit in early stage remains debated
- Onyx direct percutaneous puncture - superior devascularization vs. transarterial PVA, especially for ICA feeders
- Image-guided surgery (IGS) with neuronavigation for skull base cases
- Molecular targeting - VEGF pathway upregulation documented; FGFR pathway implicated; potential for antiangiogenic therapy (Liu et al., Curr Oncol 2026, PMID 41892175)
- Extranasopharyngeal angiofibroma - recognized as distinct entity arising in sinonasal tract (not nasopharynx); [systematic review - Gazmenga et al., Eur Arch Otorhinolaryngol 2026, PMID 41699246]
SUMMARY DIAGRAM: MANAGEMENT ALGORITHM FOR JNA
SUSPECTED JNA (Adolescent male, unilateral nasal obstruction + epistaxis)
↓
Endoscopy + CT/MRI
↓
Do NOT biopsy (risk of massive haemorrhage)
↓
Staging (Chandler/Fisch/Radkowski)
↓
┌──────────────┼──────────────────┐
↓ ↓ ↓
Stage I Stage II-IIIa Stage IIIb-IV
↓ ↓ ↓
Endoscopic Preop embolization Preop embolization
or (24-48 hrs) (DSA guided, Onyx)
Transpalatal ↓ Blood ready (4-6 units)
Endoscopic ± Caldwell ↓
Luc / MFD Midfacial Degloving +
ITF approach (Fisch)
or Facial Translocation
± Neurosurgery
↓
Postop MRI (3-6 months)
↓
Residual / Recurrent disease?
↓ ↓
Observation Revision surgery
(small volume) or Radiotherapy
REFERENCES
- Cummings Otolaryngology Head and Neck Surgery, 7th ed. - Chapter 50 (Juvenile Angiofibroma) and Chapter 95 - Comprehensive source for staging, surgical techniques, embolization
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol.1 - Embolization for JNA; histology; surgical decision-making
- Scott-Brown's Vol.2 - Infratemporal fossa approach (Fisch Type C) indications
- KJ Lee's Essential Otolaryngology - Surgical approach overview; radiation indications
- Dhingra - Transpalatal approach; clinical features
- Hazarika ENT - Clinical presentation; surgical principles
- Stell and Maran's Head and Neck Surgery - Advanced surgical approaches
- Andrews JC, Fisch U et al. - Laryngoscope 1989 - Infratemporal fossa approach for extensive JNA
- Diaz A et al. - Laryngoscope 2023 (PMID 36789781) - Meta-analysis: embolization in JNA surgery
- Segal AY et al. - J Laryngol Otol 2026 (PMID 42087760) - Embolization benefits in advanced JNA: meta-analytic comparison
- Gazmenga FP et al. - Eur Arch Otorhinolaryngol 2026 (PMID 41699246) - Extranasopharyngeal angiofibroma systematic review
- Liu X et al. - Curr Oncol 2026 (PMID 41892175) - Molecular mechanisms of JNA; VEGF/FGFR targeting
- PMC 3431533 - Changing trends in management: 150 cases, transmaxillary shift
- Atlas of Otolaryngology - Midfacial degloving + medial maxillectomy; endoscopic technique details
Total Word Count: ~2200 words | Suitable for 20-mark RGUHS answer paper
RGUHS Examiner Tip: For a 20-mark answer, the above structure covers: Introduction (1 mark) + Extranasopharyngeal manifestations with pathways (6 marks) + Staging (2 marks) + Surgical approaches in detail (8 marks) + Adjuncts/Recent advances (2 marks) + Diagrams (bonus). Use the flowcharts and tables to score maximum marks.
This is a shared conversation. Sign in to Orris to start your own chat.