Biomechanics of hip - 15 marks MPT level answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full MPT-level answer.
Biomechanics of the Hip Joint
1. Introduction
The hip joint is a multiaxial ball-and-socket (spheroidal) synovial joint formed between the head of the femur and the acetabulum of the pelvis. It is designed for both stability and mobility - bearing large forces during weight-bearing while allowing freedom of movement in three planes. Understanding its biomechanics is fundamental to clinical decision-making in conditions such as osteoarthritis, femoroacetabular impingement, fracture management, and total hip arthroplasty.
2. Osteology and Joint Architecture
Acetabulum
The acetabulum faces anterolaterally and inferiorly (at approximately 45° of inclination and 15-20° of anteversion). It is formed by the fusion of the ilium (2/5), ischium (2/5), and pubis (1/5) at the triradiate cartilage.
- Lunate surface: the horseshoe-shaped hyaline cartilage-covered articulating portion
- Acetabular fossa: centrally placed, non-articular, filled with fat (Haversian fat pad) and the ligamentum teres
- Acetabular notch: inferior gap bridged by the transverse acetabular ligament
Femoral Head
The femoral head is approximately 2/3 of a sphere (radius ~22-25 mm). It articulates within the acetabulum via hyaline cartilage. The articular cartilage is thicker superiorly (up to 3-4 mm) where peak loads occur.
CCD (Centrum-Collum-Diaphysis) Angle
The angle between the femoral neck axis and the femoral shaft axis in the coronal plane:
- Normal: ~126° (range 120-135°)
- Coxa valga: >135°
- Coxa vara: <120°
This angle has profound biomechanical implications (see Joint Reaction Force section).
Angle of Anteversion
The femoral neck is twisted anteriorly relative to the femoral shaft in the transverse plane:
- Normal: 10-15° in adults (up to 30-40° at birth, reducing with growth)
- Increased anteversion causes a tendency for internal rotation gait ("toeing in")
- Retroversion predisposes to femoroacetabular impingement
3. Degrees of Freedom and Range of Motion
The hip moves around three axes, all passing through the center of the femoral head:
| Motion | Axis | Normal ROM |
|---|---|---|
| Flexion / Extension | Transverse (coronal) | 120° / 20° (with knee flexed) |
| Abduction / Adduction | Sagittal | 45° / 20° |
| Internal / External Rotation | Vertical (longitudinal) | 40° / 50° |
Thomas Test is used to measure the true range of extension by eliminating the compensatory anterior pelvic tilt and lumbar hyperlordosis. With the contralateral hip maximally flexed, normal hip extension is approximately 20°.
4. Static Stability of the Hip Joint
Stability is primarily provided by bony architecture - the deep acetabulum and femoral head congruence. Additional stabilizers include:
Acetabular Labrum
- Fibrocartilaginous rim attached to the bony acetabular margin
- Deepens the acetabular socket by 21% and increases surface area by 28%
- Functions: load transmission, maintenance of a fluid seal (negative intra-articular pressure), synovial fluid hydrodynamics, and resistance to femoral head translation
- Note: Unlike the glenohumeral labrum, the hip labrum does not produce significant suction-cup stability. The negative pressure effect mainly acts as a "vacuum seal"
- Peripheral 1/3 is vascularized; central 2/3 is avascular
Capsule and Ligaments
- Iliofemoral ligament (Y-ligament of Bigelow): strongest ligament in the body; attaches from AIIS to the intertrochanteric line in an inverted-Y configuration; primarily resists hyperextension and external rotation
- Pubofemoral ligament: resists abduction and extension
- Ischiofemoral ligament: spirals around the femoral neck; resists internal rotation and extension
- The capsule is tight in extension and internal rotation, relaxed in flexion and external rotation (the close-packed position is extension, abduction, and internal rotation)
Ligamentum Teres
- Intra-articular but extrasynovial
- Transmits a branch of the obturator artery (posterior division) to the femoral head - significant in children, minimal in adults
- Contributes modest stability, particularly against hip dislocation
5. Joint Reaction Force (JRF)
This is the most clinically important biomechanical concept for the hip.
Lever Arm Analysis
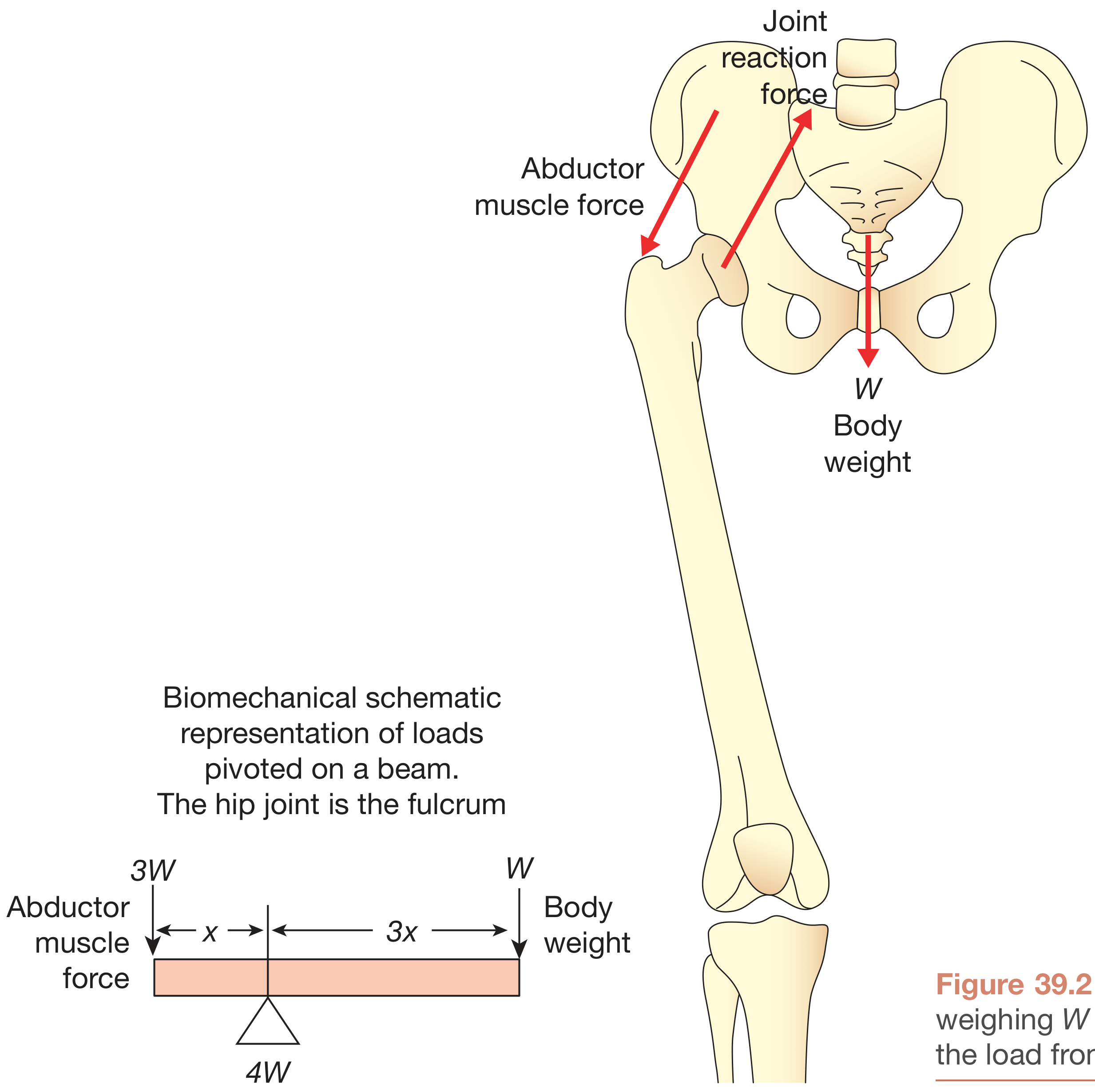
The pelvis acts as a class 1 lever with the hip joint as the fulcrum:
- The body weight (W) acts through the center of gravity, medial to the hip joint
- The hip abductors (gluteus medius, gluteus minimus, tensor fascia lata) act laterally via insertion at the greater trochanter
The lever arm of body weight is approximately 3× the lever arm of abductor muscle force. To maintain equilibrium (a level pelvis during single-leg stance):
Abductor force required = 3W (to balance body weight on the opposite side)
The Joint Reaction Force (JRF) = Body weight + Abductor force = W + 3W = 4W
JRF in Different Activities
| Activity | JRF (× Body Weight) |
|---|---|
| Lying supine | ~0.3 |
| Two-legged standing | ~0.3 |
| Lifting leg from bed | 1.5× |
| Single-leg standing / walking | 3-4× |
| Stair climbing | 5-6× |
| Running | 7-8× |
| Jumping / landing | 10× |
(Bailey & Love's Short Practice of Surgery, 28th Ed.; Miller's Review of Orthopaedics, 9th Ed.)
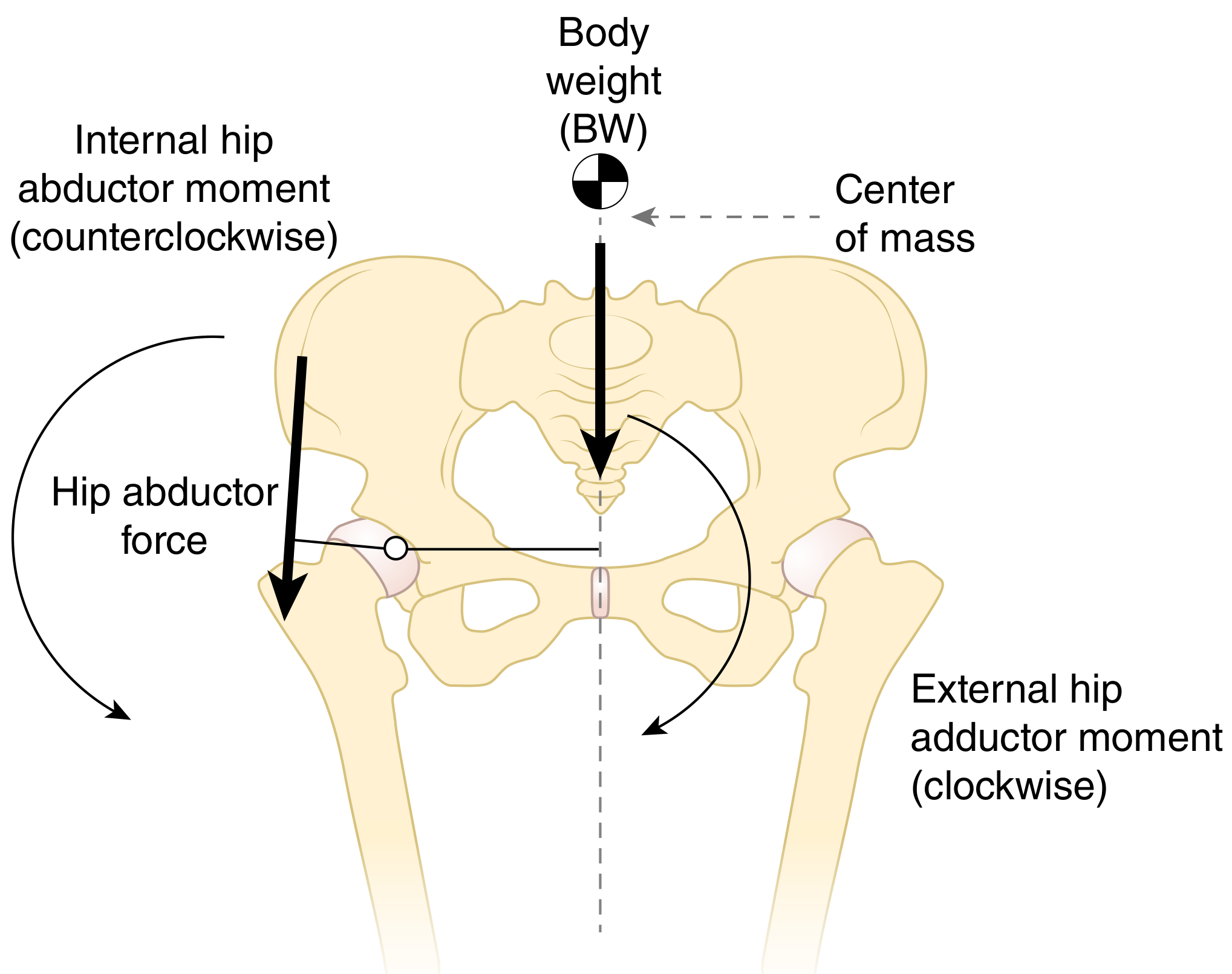
Ground Reaction Force (GRF) and Abductor Moment
During single-limb stance, the GRF passes medial to the hip joint axis. This creates an external hip adduction moment (clockwise rotation). The hip abductors must generate an equal and opposite internal abduction moment (counterclockwise) to keep the pelvis level.
If this moment is insufficient, the pelvis drops on the swing side - this is Trendelenburg gait (contralateral pelvic drop). A positive Trendelenburg sign indicates dysfunction of the stance-side hip abductors.
6. Effect of CCD Angle on Biomechanics
The CCD (neck-shaft) angle directly affects the abductor moment arm and therefore the JRF:
| CCD Angle | Condition | Abductor Moment Arm | Abductor Force Required | JRF |
|---|---|---|---|---|
| ~126° | Normal | Moderate (d = ~5 cm) | 3W | ~4W |
| >135° | Coxa valga | Decreased | Higher (up to 7W moment) | Increased (~7W) |
| <120° | Coxa vara | Increased | Lower | Decreased (~3W) |
Clinical implication: Coxa valga (as in CDH or post-fracture malunion) increases JRF, accelerating cartilage wear. Valgus intertrochanteric osteotomy (converting coxa vara to normal) or varus osteotomy can reduce JRF when indicated. When coxa valga co-occurs with acetabular dysplasia, the stress across the joint (force per unit contact area) is dramatically increased, driving early OA.
7. Trabecular Architecture and Load Transmission
The femoral head and neck have organized trabecular systems adapted to load:
- Compressive trabeculae (medial group): arch from the medial femoral cortex to the superior femoral head; resist compressive loads
- Tensile trabeculae (lateral group): arc from the lateral cortex to the medial femoral head; resist bending/tensile forces
- Ward's triangle: a relatively sparse area between the two systems - the site of femoral neck stress fractures
- Calcar femorale: dense condensation of bone along the posteromedial femoral neck; key stress-bearing structure
8. Hip Biomechanics During Gait
Stance Phase
- At heel strike, the hip is in ~30° flexion, slight abduction
- At mid-stance (single-limb support): JRF peaks (~3-4× BW); abductors most active
- At terminal stance: hip moves into extension; iliopsoas is stretched, storing elastic energy
Swing Phase
- Hip flexors (iliopsoas, rectus femoris) initiate limb advancement
- At initial swing, hip flexion increases to clear the foot
- The hip reaches ~30° flexion by terminal swing in preparation for heel strike
Energy Considerations
- The hip acts as an energy absorber at loading response and energy generator during late stance/pre-swing
- The biarticular rectus femoris couples hip and knee mechanics
9. Muscle Mechanics at the Hip
| Muscle Group | Primary Action | Key Biomechanical Role |
|---|---|---|
| Gluteus medius / minimus | Abduction | Pelvic stabilization; most important for Trendelenburg |
| Gluteus maximus | Extension + ER | Power generation in stair climbing, running |
| Iliopsoas | Flexion | Hip flexion torque; stabilizes hip in flexion |
| Short external rotators (piriformis, obturators, gemelli, quadratus femoris) | External rotation | Fine control of femoral head within acetabulum |
| Adductors | Adduction, some flexion | Control of medial thrust; assist swing phase |
| Tensor fascia lata | Abduction, medial rotation | Hip stabilization via IT band |
10. Effect of a Walking Aid on JRF
Using a cane in the contralateral hand reduces JRF across the hip joint by approximately 30-40% (from ~4W to ~2-2.5W). The cane acts as a third lever arm, reducing the demand on the hip abductors and thus decreasing the overall JRF. This principle is directly applied in clinical rehabilitation after total hip replacement and in management of hip OA.
11. Biomechanics of Total Hip Arthroplasty (THA)
Restoring normal hip biomechanics in THA requires:
- Restoring the center of rotation (medialization and verticalization affect abductor moment arm)
- Restoring femoral offset (horizontal distance from femoral shaft to head center) - reduced offset weakens abductors and increases JRF
- Leg length restoration - alters abductor tension and functional lever arm
- Excess medialization of the acetabular component reduces the abductor lever arm, mimicking coxa valga
12. Pathomechanics - Clinical Correlations
| Pathology | Biomechanical Fault |
|---|---|
| Hip OA | Reduced joint space; articular cartilage unable to distribute JRF; subchondral sclerosis |
| Femoroacetabular impingement (FAI) | Cam (non-spherical femoral head) or Pincer (over-coverage) lesions cause impingement at extremes of motion, leading to labral and chondral damage |
| CDH / Dysplasia | Reduced acetabular coverage increases contact stress; hip abductor moment arm reduced |
| AVN femoral head | Disruption of blood supply → bone death → head collapse → altered load distribution |
| Neck of femur fracture | Ward's triangle is the zone of stress riser; compressive vs. tensile trabecular disruption determines Garden classification and vascular injury risk |
| Trendelenburg gait | Abductor weakness → inadequate internal abduction moment → pelvis drops contralaterally |
Summary Points for Examination
- Hip joint is a multiaxial ball-and-socket joint - primary stability from bony architecture
- JRF = 4× BW in single-leg stance; up to 10× BW during jumping
- The hip joint acts as a class 1 lever; abductor force must be 3W to balance body weight of W on the opposite side
- CCD angle determines abductor lever arm: coxa valga increases JRF; coxa vara decreases it
- Acetabular labrum deepens socket by 21%, provides fluid seal - not suction stability
- Trendelenburg sign = positive (pelvis drops contralateral side) when stance-side abductors are weak or the lever arm is reduced
- Contralateral cane reduces JRF by 30-40%
- Trabecular systems (compressive + tensile) are oriented along principal stress lines; Ward's triangle is the vulnerable zone
- Femoral anteversion (normal 10-15°) influences rotational mechanics and impingement risk
- THA must restore offset, leg length, and center of rotation to normalize biomechanics
Sources: Bailey and Love's Short Practice of Surgery (28th Ed.); Firestein & Kelley's Textbook of Rheumatology; Miller's Review of Orthopaedics (9th Ed.); Thieme Atlas of Anatomy - General Anatomy and Musculoskeletal System; Imaging Anatomy - Bones, Joints, Vessels and Nerves
explain me in simple language
Biomechanics of the Hip - Simple Explanation
Let me break this down like a story, piece by piece.
1. What Kind of Joint is the Hip?
Think of a ball and socket - like a joystick in a cup. The ball is the rounded top of your thigh bone (femur), and the cup is the acetabulum in your pelvis.
Because it's a ball-in-cup design, you can move your leg in all directions - forward, backward, sideways, and rotate it. That's why it's called a "multiaxial" joint.
2. How Does the Hip Stay Stable?
Three main things hold it in place:
a) The deep cup (bony fit)
The cup is deep enough to hold the ball firmly. This is the most important stabilizer.
b) The rubber ring (labrum)
Around the rim of the cup, there's a rubbery ring called the labrum. Think of it like the rubber seal on a jar lid - it:
- Makes the cup 21% deeper
- Creates a vacuum/suction effect to keep the ball inside
- Distributes pressure evenly
c) Ligaments (strong ropes)
- The Y-ligament (Iliofemoral) is the strongest ligament in the entire body. It stops you from falling backward when you stand upright.
- Think of it as a seat belt for your hip.
3. How Much Force Goes Through the Hip? (The Most Important Part!)
This surprises most people.
Your hip doesn't just carry your body weight - it carries MUCH more.
Here's why:
The See-Saw Analogy
Imagine a see-saw (lever). The hip joint is the pivot point in the middle.
- On one side: your body weight pushing down (acts far from the pivot - about 3 units away)
- On the other side: your hip muscles (abductors) pulling up (act close to the pivot - only 1 unit away)
Because the body weight arm is 3× longer than the muscle arm, the muscles must pull with 3× body weight just to keep the pelvis level.
Now add them both together at the pivot point (hip joint):
Joint force = body weight (1W) + muscle force (3W) = 4W
So just standing on one leg puts 4× your body weight through your hip!
Real numbers for a 70 kg person:
| Activity | Force through hip |
|---|---|
| Lying in bed | ~20 kg |
| Standing on both legs | ~20 kg |
| Lifting your leg | ~105 kg |
| Walking | ~280 kg |
| Climbing stairs | ~350-420 kg |
| Running | ~490-560 kg |
| Jumping | ~700 kg |
4. The Neck-Shaft Angle (CCD Angle) - Why it Matters
The thigh bone doesn't go straight up - it has a neck that sticks out at an angle (~126°). This angle controls how well the hip muscles work.
Think of it like a crane arm:
- Normal angle (126°) = crane arm at a good angle = muscles work efficiently = moderate force = 4W through joint
- Too steep angle - Coxa Valga (>135°) = crane arm too vertical = muscles have a short lever = must pull harder = 7W through joint (bad!)
- Too flat angle - Coxa Vara (<120°) = crane arm angled out more = muscles have a longer lever = pull less hard = 3W through joint (better for the joint)
Bottom line: A steeper neck angle = more force on the joint = more wear and tear.
5. The Trendelenburg Sign - Explained Simply
When you stand on one leg, the muscles on the same side (hip abductors = gluteus medius) must contract hard to stop your pelvis from tilting.
If these muscles are weak or not working:
- The pelvis drops down on the opposite side
- You lean your body toward the bad side to compensate
- This is called Trendelenburg gait - the typical "waddling" walk
Simple test: Ask the patient to stand on one leg. If the opposite hip drops, that's a positive Trendelenburg sign - abductors are weak on the standing side.
6. Why a Walking Stick Helps So Much
If you hold a walking stick in the hand opposite to the bad hip, it acts like a third leg.
- The stick takes some of the body weight
- The muscles don't need to work as hard
- Force through the hip joint drops by ~30-40% (from 4W to about 2.5W)
This is why we always say: "cane in the opposite hand" - not the same side.
7. The Bone Architecture of the Femoral Neck
Inside the femoral neck, the bone is arranged in two crossing patterns (like a crossed arch):
- Compression trabeculae - arches that carry squeezing forces (like the arch of a bridge)
- Tension trabeculae - fibers that resist pulling/bending forces
Where these two systems cross, there's a weak zone called Ward's Triangle - this is exactly where femoral neck stress fractures happen in runners and osteoporotic patients.
8. Hip Biomechanics During Walking
Think of the hip like a pendulum + spring:
| Phase | What Happens | Hip's Role |
|---|---|---|
| Heel strike | Leg hits ground, hip at 30° bend | Absorbs the impact |
| Mid-stance | Full weight on one leg | Hardest moment - peak muscle work |
| Toe-off | Pushing forward | Generates power |
| Swing | Leg lifts and swings forward | Hip flexors pull leg through |
9. How All This Applies Clinically
| Patient Complaint | Biomechanical Reason |
|---|---|
| Hip wears out faster in tall/heavy people | More body weight = more JRF = more cartilage stress |
| Waddling gait after hip replacement | Abductor muscles disturbed during surgery |
| Surgeon advises walking stick after hip surgery | Reduces joint force by 30-40% |
| Stress fractures in runners | Repetitive forces through Ward's triangle |
| Hip dysplasia causes early arthritis | Small cup = small contact area = high stress per cm² |
Quick Summary (One-liners to Remember)
- Hip = ball in a deep cup - stability from shape first, ligaments second
- JRF = 4× body weight during single-leg stance (3× from muscles + 1× from body weight)
- Steeper neck angle = more joint force (coxa valga is bad, coxa vara is better)
- Gluteus medius = the most important muscle for keeping pelvis level while walking
- Trendelenburg = pelvis drops opposite side when abductors are weak
- Cane in opposite hand reduces hip force by ~30-40%
- Ward's triangle is the weak zone where femoral neck fractures occur
- Labrum = rubber seal that deepens the cup and creates a fluid seal
This is a shared conversation. Sign in to Orris to start your own chat.