Paracetamol 650 and levocetrizine dihydrocloride
Reading File
search_medical_text
paracetamol 650mg pharmacology indications dosage adverse effects
search_medical_text
levocetirizine dihydrochloride pharmacology indications antihistamine
GradeResponse
GradeResponse
Here is a comprehensive overview of both drugs and their combination:
Paracetamol 650 mg + Levocetirizine Dihydrochloride
This is a common fixed-dose combination (FDC) used in cold, flu, and allergic conditions presenting with fever, pain, and allergic symptoms simultaneously.
1. Paracetamol (Acetaminophen) 650 mg
Pharmacology
- Class: Non-opioid analgesic / Antipyretic
- Mechanism: Inhibits prostaglandin synthesis centrally (COX-3 pathway); also activates descending serotonergic pathways. Lacks significant peripheral anti-inflammatory action.
- Onset: 30–60 minutes (oral); Peak effect: 1–2 hours
Indications
- Fever (antipyretic)
- Mild to moderate pain — headache, myalgia, dental pain, post-operative pain
- Symptomatic relief in dengue, chikungunya, influenza (preferred over NSAIDs in these viral conditions)
Dosage
| Population | Dose |
|---|---|
| Adults | 500–1000 mg every 4–6 hours |
| Max daily dose | 4000 mg/day (3000 mg/day in elderly, liver disease, alcohol users) |
| The 650 mg dose | A common extended-release or IR formulation given TID–QID |
The 650 mg dose is widely used in India and Asia as a higher unit dose for more effective analgesia/antipyresis while staying within daily limits.
Adverse Effects
- Generally well tolerated at therapeutic doses
- Hepatotoxicity is the major concern — dose-dependent; risk increased with alcohol use, malnutrition, liver disease
- Rare: allergic skin reactions, thrombocytopenia
Contraindications
- Severe hepatic impairment
- Known hypersensitivity to paracetamol
- Chronic alcoholism (relative)
2. Levocetirizine Dihydrochloride
Pharmacology
- Class: Second-generation antihistamine (H₁-receptor antagonist)
- Mechanism: Levocetirizine is the active R-enantiomer of cetirizine. It selectively and competitively blocks peripheral H₁ receptors, reducing histamine-mediated effects. It is less lipophilic than first-generation antihistamines, resulting in minimal CNS penetration and low sedation.
- Onset: ~1 hour; Half-life: ~6–10 hours
- Protein binding: ~91–92%
- Excretion: Primarily renal (~85% unchanged in urine)
Indications
(Per Harrison's Principles of Internal Medicine)
- Allergic rhinitis (seasonal and perennial)
- Chronic urticaria / idiopathic urticaria
- Allergic conjunctivitis (itching, tearing, erythema)
- Sneezing, nasal/ocular pruritus, watery rhinorrhea
Dosage
| Population | Dose |
|---|---|
| Adults & children ≥12 yr | 5 mg once daily (evening) |
| Children 6–11 yr | 2.5 mg once daily |
| Renal impairment | Dose reduction required (renally cleared) |
Adverse Effects
- Somnolence (less than older antihistamines, but possible)
- Dry mouth, fatigue, headache
- Rare: QT prolongation (at very high doses)
Contraindications
- Severe renal failure (CrCl <10 mL/min)
- End-stage renal disease on dialysis
- Known hypersensitivity to cetirizine or hydroxyzine
3. The Combination — Rationale
| Component | Role in Combination |
|---|---|
| Paracetamol 650 mg | Treats fever and body pain |
| Levocetirizine 5 mg | Controls sneezing, runny nose, watery eyes, and allergic itch |
Common brand names (India): Levorid-P, Allercet-P, Lcz-P, Alenex-P, etc.
Typical indication: Upper respiratory tract infections (URTI) / common cold with allergic component — presenting with fever, headache, myalgia + sneezing, rhinorrhea, nasal itching.
4. Key Clinical Points
- Preferred over NSAIDs in viral fevers (dengue, flu) because paracetamol does not inhibit platelet function
- Levocetirizine does not treat nasal congestion well; a decongestant (e.g., pseudoephedrine) may be added if congestion is prominent
- Avoid alcohol with this combination (hepatotoxicity risk from paracetamol; additive CNS depression from levocetirizine)
- Renal caution: Levocetirizine dose must be adjusted in renal impairment
- Not first-line in pregnancy — consult before use; paracetamol is generally considered safer than NSAIDs in pregnancy but prolonged use has been debated
Disclaimer: This information is for educational purposes. Clinical decisions should be made by a qualified healthcare professional based on individual patient assessment.
SWD in physical therapy is it that much effective or there are side effects thyas why some country ban it and what are the best 2 alternative of this and same or more beneficial for patient
Pain below lateral malleolus posterolateral border of foot reason tests physiotherapy treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching Images
peroneal tendon subluxation lateral malleolus anatomy
Now I have sufficient data. Let me compile a comprehensive answer from both library findings and clinical knowledge.
PART 1: Shortwave Diathermy (SWD) in Physiotherapy
What Is SWD?
Shortwave Diathermy uses high-frequency electromagnetic waves (27.12 MHz) to generate deep tissue heat. It penetrates 3–5 cm into tissue — reaching muscles, joints, and deep soft tissue — unlike superficial heat modalities (hot packs, IRR).
Two modes:
- Continuous SWD (CSWD) — thermal effects (heat)
- Pulsed SWD (PSWD) / PEMF — non-thermal, biostimulatory effects
Is SWD Effective?
| Condition | Evidence |
|---|---|
| Osteoarthritis (knee, hip) | Moderate evidence for short-term pain relief & improved ROM |
| Chronic low back pain | Weak-to-moderate evidence; thermal effect provides temporary relief |
| Pelvic inflammatory pain | Some benefit in chronic cases |
| Soft tissue injuries | Pulsed SWD shows benefit in reducing edema and inflammation |
| Post-surgical recovery | Limited evidence; pulsed form used for wound healing |
Honest assessment: SWD has been used for decades but its evidence base is considered weak to moderate by current standards (Cochrane reviews rate evidence as low quality). It provides temporary symptomatic relief, but few studies demonstrate long-term superiority over other modalities or placebo. Many physiotherapy bodies have downgraded its routine clinical use.
Side Effects of SWD
| Side Effect | Details |
|---|---|
| Burns | Most serious risk — if metal implants, wet dressings, or improper technique used |
| Skin irritation / erythema | Due to excessive heating |
| Superficial burns | If patient has impaired sensation or is unable to report heat |
| Eye damage | Eyes must be kept out of the field; cataracts risk with chronic exposure |
| Potential genotoxicity | Concerns about DNA damage at cellular level from prolonged exposure |
| Operator hazard | Therapists exposed chronically — WHO has raised concerns about occupational EMF exposure |
| Pacemaker/implant interaction | Absolute contraindication — SWD can permanently damage pacemakers, cochlear implants, neuro-stimulators (e.g., InterStim) — Harrison's 22E; Hinman's Urologic Surgery |
| Fetal risk | Contraindicated over pregnant uterus — possible teratogenic effects |
Why Some Countries Have Banned or Restricted SWD
Several countries and regulatory bodies have restricted or phased out SWD based on:
- WHO/ICNIRP guidelines on non-ionizing radiation exposure — chronic EMF exposure at 27 MHz poses occupational health concerns for treating physiotherapists
- Weak clinical evidence — insufficient RCT support for many indications
- Safety profile — risk of burns especially in sensory-impaired patients
- Device regulations — strict EMF emission standards in the EU (EU Directive 2013/35/EU on occupational EMF exposure) effectively restricted SWD use in many European clinical settings
- Australia — Therapeutic Goods Administration (TGA) requires strict regulation; some hospitals have removed SWD units
- USA — FDA has not banned it but many insurance providers no longer reimburse for SWD due to weak evidence
The core issue: risk-to-benefit ratio is unfavorable when better, safer alternatives exist.
Absolute Contraindications for SWD
- Metal implants in the treatment area
- Cardiac pacemakers / implanted electronic devices
- Pregnancy (over the uterus/gonads)
- Active malignancy
- Impaired sensation (high burn risk)
- Active bleeding / acute inflammation
- Thrombosis / DVT
Best 2 Alternatives to SWD — Equal or Greater Benefit
✅ 1. Therapeutic Ultrasound (US Therapy)
Frequency: 1 MHz (deep) or 3 MHz (superficial) | Penetration: up to 5 cm
| Feature | Details |
|---|---|
| Mechanism | Thermal + non-thermal (cavitation, acoustic streaming) |
| Effects | Increases collagen extensibility, accelerates tissue repair, reduces inflammation, improves blood flow |
| Modes | Continuous (thermal) / Pulsed (non-thermal) |
| Indications | Tendinopathies, bursitis, muscle tears, joint contractures, scar tissue, ligament injuries |
| Advantages over SWD | Better depth specificity, more targeted, no occupational EMF hazard, usable over most implants (away from area), more evidence-based |
| Evidence | Good evidence for soft tissue healing, tendinopathy, and post-injury rehabilitation |
| Side effects | Minimal — periosteal pain if bone contacted, burns if stationary head, avoid over growth plates in children |
Why better? More targeted, thermal + mechanical effects, safer occupational profile, and clinically better supported than SWD for most musculoskeletal conditions.
✅ 2. TENS (Transcutaneous Electrical Nerve Stimulation)
Frequency: Typically 80–100 Hz (conventional) or 1–4 Hz (acupuncture TENS)
| Feature | Details |
|---|---|
| Mechanism | Gate control theory (high-freq TENS) + endorphin release (low-freq TENS) |
| Effects | Analgesia, muscle relaxation, reduces central sensitization |
| Modes | Conventional, burst, acupuncture-like, modulated |
| Indications | Chronic and acute pain — arthritis, neuropathic pain, post-op pain, sports injuries, low back pain, ankle/foot pain |
| Advantages over SWD | Non-thermal (no burn risk), portable (home use), excellent safety profile, strong evidence for pain management |
| Evidence | Strong evidence for pain relief in osteoarthritis, chronic musculoskeletal pain, neuropathic pain |
| Side effects | Skin irritation under electrodes, contraindicated over pacemaker/epilepsy/carotid sinus |
Why better? Exceptional pain control with virtually no thermal risk, can be used at home, WHO-endorsed for pain management, and avoids all EMF occupational concerns.
Bonus mention: Laser Therapy (LLLT/Class IV laser) is emerging as a strong third alternative with strong anti-inflammatory and tissue healing evidence, especially for tendinopathies.
PART 2: Pain Below Lateral Malleolus — Posterolateral Border of Foot
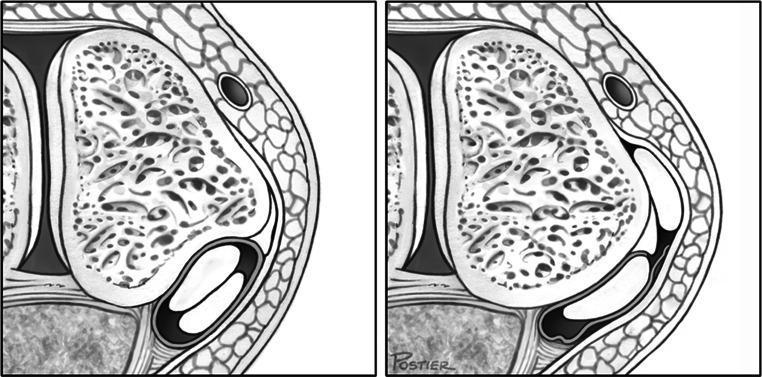
Anatomy of the Region
The structures at risk posterior and inferior to the lateral malleolus include:
| Structure | Location |
|---|---|
| Peroneus brevis tendon | Runs directly posterior to lateral malleolus → inserts at 5th metatarsal base |
| Peroneus longus tendon | Runs with brevis → curves under foot |
| Superior peroneal retinaculum (SPR) | Holds tendons in retromalleolar groove |
| Sural nerve | Lateral border of ankle and foot |
| Calcaneofibular ligament (CFL) | Below lateral malleolus to calcaneus |
| Subtalar (posterior facet) joint | Just inferior/posterior |
Common Causes of Posterolateral Foot Pain (Below Lateral Malleolus)
| Condition | Key Feature |
|---|---|
| Peroneal tendon tear/tendinopathy | Most common cause of chronic pain after ankle sprain — Miller's Review of Orthopaedics |
| Peroneal tendon subluxation/dislocation | Snap/click with pain; forced dorsiflexion-eversion mechanism |
| Calcaneofibular ligament (CFL) sprain | Lateral ankle instability + posterolateral pain |
| Sural nerve entrapment | Burning, tingling along lateral foot border |
| Os peroneum fracture | Sharp pain with acute peroneus longus rupture; seen on X-ray |
| Subtalar joint pathology | Deep diffuse pain, worsened by uneven surfaces |
| Posterior ankle impingement | Pain behind ankle, worse in plantarflexion |
| Calcaneal fracture | Post-trauma heel and lateral foot pain |
Clinical Tests
For Peroneal Tendon Pathology
| Test | Method | Positive Sign |
|---|---|---|
| Peroneal Tendon Palpation | Direct palpation along posterior border of fibula to 5th MT | Tenderness, thickening, or crepitus along the tendon |
| Resisted Eversion Test | Patient everts foot against resistance | Pain/weakness posterior to lateral malleolus |
| Single Limb Heel Rise | Patient stands on one foot and raises heel | Inability or pain = peroneal/PTT dysfunction |
| Peroneal Compression Test | Compress peroneal tendon sheath against fibula | Pain or crepitus = tenosynovitis |
| Tendon Subluxation Provocation | Active dorsiflexion + eversion against resistance | Palpable/audible snap = subluxation |
For Lateral Ankle Ligament (CFL / ATFL)
| Test | Method | Positive Sign |
|---|---|---|
| Anterior Drawer Test | Anterior force on heel with foot in 10° plantarflexion | >10 mm translation = ATFL tear |
| Talar Tilt Test | Inversion stress to hindfoot | Excessive inversion = CFL tear |
| Squeeze Test | Compress tibia-fibula at mid-shaft | Distal pain = syndesmosis injury |
For Sural Nerve
| Test | Method |
|---|---|
| Tinel's Sign at lateral ankle | Tap posterior to lateral malleolus along sural nerve course — tingling/pain = nerve entrapment |
Investigations
| Investigation | Purpose |
|---|---|
| Weight-bearing X-ray | Fracture, os peroneum, calcaneal deformity |
| MRI (gold standard) | Peroneal tendon tears, retinaculum injury, ligament tears, bone edema |
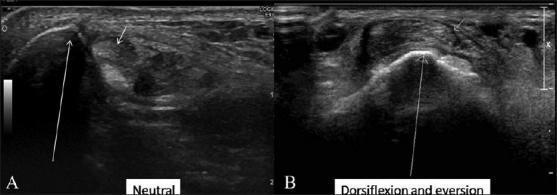
| Ultrasound (dynamic) | Peroneal tendon subluxation (assessed dynamically in dorsiflexion-eversion) — Miller's, Imaging Anatomy Atlas |
| Stress X-ray | Assess degree of ligament laxity |
Physiotherapy Treatment
Phase 1 — Acute (0–2 weeks)
- RICE (Rest, Ice, Compression, Elevation)
- TENS for pain control
- Offloading / protective splinting (moon boot or functional brace)
- Ultrasound therapy (pulsed) — reduce inflammation and edema
Phase 2 — Subacute (2–6 weeks)
- Manual therapy: Joint mobilization (subtalar, talocrural)
- Ultrasound therapy (continuous): Improve tendon healing and extensibility
- Stretching: Calf (gastrocnemius + soleus), Achilles
- Isometric eversion/inversion exercises: Pain-free range
- Taping: Peroneal tendon support taping or kinesio taping
Phase 3 — Strengthening (6–12 weeks)
- Progressive resistance exercises:
- Resisted eversion with theraband
- Single-leg calf raises
- Terminal knee extension
- Proprioception/balance training: Wobble board, BOSU ball, single-leg stance
- Neuromuscular re-education: Key to prevent recurrence
Phase 4 — Functional/Return to Activity
- Sport-specific drills, agility training
- Orthotic prescription (lateral heel wedge, arch support) if structural deformity
- Taping or bracing for return to sport
Surgical Consideration
- Peroneal tendon subluxation requiring SPR repair + fibular groove deepening
- Large tendon tears failing conservative management (tenosynovectomy, debridement, repair) — Miller's Review of Orthopaedics
Summary: SWD has significant safety concerns (burns, EMF occupational hazard, implant danger) and weak-to-moderate evidence, driving regulatory restrictions in Europe and declining use globally. Therapeutic ultrasound and TENS are superior alternatives — better evidence, safer profile, and equivalent or greater benefit. For posterolateral foot pain below the lateral malleolus, peroneal tendon pathology is the #1 cause and is managed with a structured physiotherapy program focusing on pain control, tendon healing, and progressive neuromuscular re-education.
This is a shared conversation. Sign in to Orris to start your own chat.