Explain carcinoma of lungs especially squamous cell carcinoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"squamous cell carcinoma" AND "lung" AND "treatment"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have very rich content from multiple authoritative sources. Let me compile the comprehensive answer.
Carcinoma of the Lung - With Special Emphasis on Squamous Cell Carcinoma
Overview and Epidemiology
Lung carcinoma is the leading cause of cancer-related death in high-resource countries - accounting for roughly one-third of all cancer deaths in men and, since 1987, also the leading cancer killer in women. The American Cancer Society estimated ~237,000 new cases and ~130,000 deaths annually (2022 data). The peak incidence is in the fifties and sixties. At diagnosis, more than 50% of patients already have distant metastases, and an additional 25% have regional lymph node disease. The overall 5-year survival for all stages combined is approximately 20%, and even for localized disease it is only ~50%.
Roughly 95% of primary lung tumors are carcinomas; the remaining 5% include carcinoids, mesenchymal tumors, lymphomas, and rare benign lesions (the most common benign tumor is a "hamartoma").
Classification of Lung Carcinoma
The four major histologic types are:
| Type | Frequency | Key Features |
|---|---|---|
| Adenocarcinoma | ~50% | Peripheral, women/non-smokers, EGFR/KRAS mutations |
| Squamous cell carcinoma | ~20-25% | Central/hilar, strong smoking link, keratin pearls |
| Small cell carcinoma | ~13-15% | Neuroendocrine, TP53/RB mutations, early metastasis |
| Large cell carcinoma | ~5-10% | Diagnosis of exclusion, poor differentiation |
Historically, the most important clinical distinction was SCLC vs. NSCLC (NSCLC = adenocarcinoma + SCC + large cell). This division persists because SCLC is usually unresectable, spread is universal, and surgery does not help - whereas NSCLCs may be resected and have targetable molecular drivers.
- Robbins & Kumar Basic Pathology, p. 485-486
- Murray & Nadel's Textbook of Respiratory Medicine, p. 559
Etiology and Risk Factors
Tobacco smoking is the single most important risk factor for all types, but has the strongest association with squamous cell and small cell carcinoma. As tobacco use has declined in the U.S., adenocarcinoma has overtaken SCC as the most common type.
Other risk factors include:
- Radon gas (second most common cause of lung cancer)
- Occupational exposures: asbestos, arsenic, chromium, nickel, uranium
- Air pollution
- Prior lung fibrosis/scarring
- Genetic predisposition (mutations in RB, TP53 germline)
Squamous Cell Carcinoma (SCC) of the Lung - Detailed
Epidemiology
SCC accounts for approximately 25% of all lung cancers in the U.S. It is more common in men than women, and chronic smoking continues to be the dominant risk factor.
Location and Gross Pathology
- Classically arises centrally - in major bronchi, near the hilum (Fig. 11.44D in Robbins). Historically, up to two-thirds of SCC cases presented as central hilar tumors.
- Over the past 2 decades, peripheral SCC has become more frequent (possibly related to the shift from unfiltered to filtered cigarettes in the 1960s-70s).
- Large lesions often undergo central necrosis, producing cavitation - a key radiological feature.
- Tends to spread first to local hilar lymph nodes, and dissemination outside the thorax occurs later on average than with adenocarcinoma.
Histogenesis (Precursor Lesions)
Smoking promotes a stepwise transformation of bronchial epithelium:
Normal bronchial epithelium → Squamous metaplasia → Squamous dysplasia → Carcinoma in situ → Invasive SCC
During the carcinoma-in-situ phase, atypical cells may already be detectable in sputum cytology or bronchial lavage/brushings, even when imaging is normal. The lesion may remain asymptomatic for years at this stage.
Histopathology - Defining Features
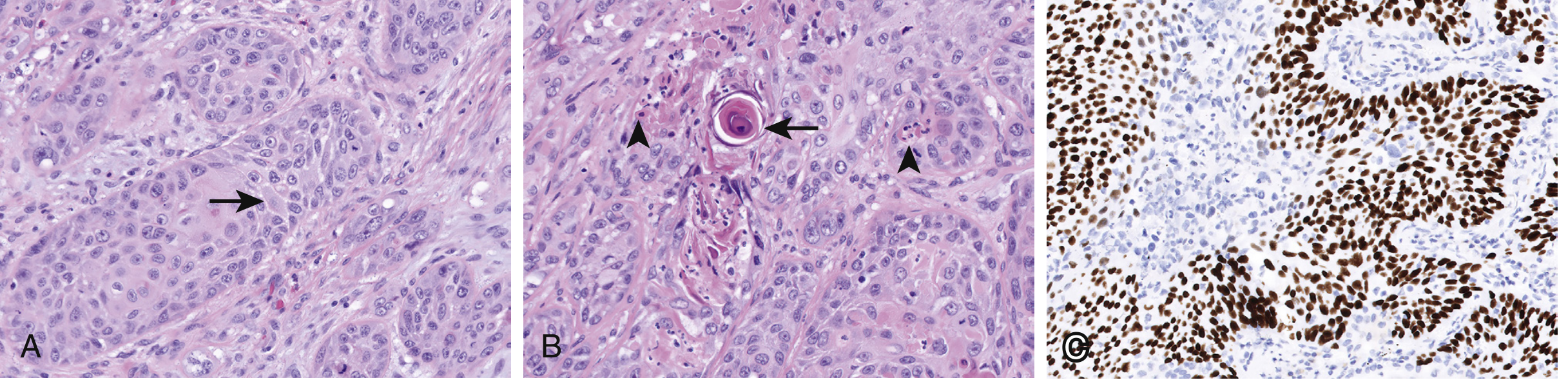
Figure: Squamous cell carcinoma. (A) Intercellular bridges (arrow). (B) Intracellular keratinization and keratin pearls (arrow). (C) p40 expression by IHC confirming squamous differentiation. (Murray & Nadel, Fig. 22.2)
Three classic morphologic markers of squamous differentiation:
- Intercellular bridges - prominent in well-differentiated tumors
- Individual cell keratinization - cells with eosinophilic cytoplasm and pyknotic nuclei
- Keratin pearls - concentric whorls of keratinized cells, pathognomonic
These features are readily apparent in well-differentiated tumors, subtle or focal in moderately differentiated tumors, and may be entirely absent in poorly differentiated tumors (where IHC becomes necessary).
Grading: Well-differentiated / Moderately differentiated / Poorly differentiated - though no universally accepted system exists.
WHO 2015 subtypes: Keratinizing, Non-keratinizing, and Basaloid - though these have little prognostic significance.
Immunohistochemistry
| Marker | SCC | Adenocarcinoma |
|---|---|---|
| p63 / p40 | Positive | Negative |
| TTF-1 | Negative | Positive |
| Napsin A | Negative | Positive |
| CK5/CK6 | Positive | Negative |
p40 (splice variant of p63) is more specific and is the preferred marker. Mucin is absent in SCC but present in adenocarcinoma.
Molecular Alterations in SCC
Next-generation sequencing identifies recurrent alterations:
- TP53 mutations: ~65%
- PIK3CA: ~30%
- CDKN2A (p16): ~25%
- SOX2 amplification: ~15%
- CCND1 amplification: ~15%
- FGFR1 amplification: up to ~20% - but FGFR inhibitors have been largely ineffective
- 3p deletions: ~80% (shared with SCLC)
- RB mutations: ~20%
Importantly, EGFR mutations and ALK fusions are absent or very rare in SCC. KRAS mutations are also uncommon. This means most targeted therapies used in adenocarcinoma (gefitinib, erlotinib, crizotinib) are not applicable to SCC.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 562
- Robbins & Kumar Basic Pathology, p. 488 (Table 11.6)
Clinical Presentation of Lung Carcinoma
Local/Locoregional Effects
- Cough (most common) - often productive or blood-tinged
- Hemoptysis - more common with central/endobronchial tumors (especially SCC)
- Wheezing/stridor - from bronchial obstruction
- Atelectasis and post-obstructive pneumonia - distal to the tumor
- Dyspnea - progressive
- Chest pain - pleural involvement or chest wall invasion
- Hoarseness - left recurrent laryngeal nerve compression
- SVC syndrome - from mediastinal involvement
- Pancoast (superior sulcus) syndrome - apical tumors invading T1 nerve root/brachial plexus → shoulder/arm pain, Horner syndrome (ptosis, miosis, anhidrosis)
- Pericardial effusion / tamponade - pericardial extension
Paraneoplastic Syndromes
Lung cancers produce a variety of paraneoplastic syndromes. The high mutation burden from tobacco carcinogens means these tumors express many neoantigens.
| Syndrome | Tumor Type | Mechanism |
|---|---|---|
| Hypercalcemia | SCC (most common) | PTH-related protein (PTHrP) secretion |
| SIADH (hyponatremia) | Small cell | Ectopic ADH |
| Cushing syndrome | Small cell | Ectopic ACTH |
| Lambert-Eaton myasthenic syndrome | Small cell | Anti-VGCC antibodies |
| Clubbing / HPOA | Adenocarcinoma, large cell | Unknown |
| Thrombophlebitis | Adenocarcinoma | Hypercoagulability |
SCC specifically causes hypercalcemia via ectopic PTHrP secretion - this is a high-yield paraneoplastic association. The serum PTH will be low (suppressed), but PTHrP will be elevated, and calcium will be high.
Staging (TNM System - IASLC 8th Edition)
Staging drives treatment decisions:
| Stage | Description | Treatment |
|---|---|---|
| Stage I (T1-2, N0, M0) | Localized, no nodes | Surgery (lobectomy) ± adjuvant chemo |
| Stage II (T1-2, N1 or T3, N0) | Local nodes or larger tumor | Surgery + adjuvant chemotherapy |
| Stage IIIA (T3-4, N1-2) | Mediastinal involvement | Concurrent chemoradiation ± surgery |
| Stage IIIB/C (N3 or T4, N2) | Extensive mediastinal | Definitive chemoradiation + immunotherapy |
| Stage IV (M1) | Distant metastases | Systemic therapy (immunotherapy/chemotherapy) |
FDG-PET/CT plays a central role in staging NSCLC - it identifies unsuspected metastatic disease and guides biopsy selection.
Diagnosis
- Chest X-ray / CT chest - initial imaging; may show hilar mass, cavitation (SCC), peripheral nodule
- Sputum cytology - especially useful in central SCC (sensitivity varies)
- Bronchoscopy with biopsy - for central lesions; brushings and lavage
- CT-guided percutaneous needle biopsy - for peripheral lesions
- PET-CT - staging
- Mediastinoscopy / EBUS - mediastinal node sampling
- Molecular testing - all NSCLC cases require reflex testing for EGFR, ALK, ROS1, KRAS, BRAF, MET, RET, NTRK, PD-L1 expression
Treatment
Surgery
Lobectomy or pneumonectomy is the preferred approach for resectable (Stage I-IIIA) disease. SCC responds to surgery similarly to other NSCLC types.
Chemotherapy
- Platinum-based doublets (cisplatin/carboplatin + paclitaxel or gemcitabine) remain the backbone for SCC.
- SCC does not respond to pemetrexed (an antifolate effective only in non-squamous NSCLC).
Immunotherapy (Immune Checkpoint Inhibitors)
Because lung cancers carry a high mutational burden from tobacco carcinogens, they express many tumor neoantigens and respond well to immune checkpoint blockade. Key agents:
- Pembrolizumab (anti-PD-1) - first-line for high PD-L1 expressors
- Nivolumab + ipilimumab combinations
- Even tumors without PD-L1 expression may respond (due to PD-L1 on infiltrating macrophages)
A 2025 systematic review (PMID 40913837) shows that neoadjuvant/perioperative immunotherapy followed by surgery is superior to surgery-first approaches in resectable NSCLC.
Targeted Therapy
SCC has no currently actionable targeted therapies in routine use - unlike adenocarcinoma (EGFR inhibitors, ALK/ROS1 inhibitors, etc.). FGFR inhibitors are under investigation but have not shown consistent benefit despite FGFR1 amplification in ~20% of SCC.
Prognosis
- Overall 5-year survival: ~20% for all stages combined
- SCC tends to disseminate later than adenocarcinoma, giving a slightly better window for surgical resection in centrally located tumors
- However, at the time of diagnosis, central SCC often causes obstructive symptoms earlier, which can paradoxically lead to earlier detection
- Cavitating lesions and extensive mediastinal involvement worsen prognosis
Key Comparison: SCC vs. Other Major Subtypes
| Feature | SCC | Adenocarcinoma | Small Cell |
|---|---|---|---|
| Location | Central (hilar) | Peripheral | Central |
| Smoking link | Very strong | Moderate | Very strong |
| Cavitation | Yes | Rare | No |
| Paraneoplastic | Hypercalcemia (PTHrP) | HPOA, clubbing | SIADH, Cushing, LEMS |
| Precursor | Squamous dysplasia → CIS | AAH → AIS | None identified |
| IHC | p63/p40 + | TTF-1/Napsin A + | CD56/Chromogranin + |
| Targetable mutations | Rare/None | EGFR, ALK, KRAS, ROS1 | None |
| Checkpoint inhibitors | Responsive | Responsive | Less responsive |
| Surgery | Possible (early stage) | Possible (early stage) | Not curative |
Sources:
- Robbins & Kumar Basic Pathology (10th Ed.), pp. 485-492
- Murray & Nadel's Textbook of Respiratory Medicine, pp. 559-563
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Table 15.9 and Classification
- Recent evidence: Neoadjuvant immunotherapy in resectable NSCLC - PMID 40913837 (ESMO Open, 2025 - Systematic Review & Meta-Analysis)
This is a shared conversation. Sign in to Orris to start your own chat.