Dural venous thrombosis
Reading File
Checking Date & Time
Finding Sources
Searching PubMed
"cerebral venous thrombosis"[MeSH Terms] AND ("diagnosis" OR "treatment")
Reading File
Finding Sources
Searching PubMed
"cerebral venous thrombosis"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content and images. Here is a thorough synthesis:
Dural Venous Sinus Thrombosis (Cerebral Venous Thrombosis)
Cerebral venous thrombosis (CVT) refers to thrombosis of the dural venous sinuses and/or cortical veins. It accounts for 0.5–1% of all strokes and has a mean age of presentation of ~39 years, with a strong female predominance.
Anatomy & Classification
Aseptic CVT is divided into three types:
- Dural venous sinus thrombosis — most common type
- Deep cerebral vein thrombosis (internal cerebral veins, vein of Galen)
- Superficial/cortical vein thrombosis
Most frequently thrombosed sinuses (in descending order):
- Superior sagittal sinus (most common)
- Transverse sinuses
- Sigmoid sinuses
- Deep sinuses (in neonates especially)
- Cavernous sinus (usually septic — see below)
Etiology & Risk Factors
The causes are protean; ~15–20% of cases remain idiopathic. Key categories:
| Category | Examples |
|---|---|
| Prothrombotic states | Oral contraceptive pills, pregnancy/puerperium, antiphospholipid syndrome, factor V Leiden, protein C/S deficiency, antithrombin III deficiency, polycythemia |
| Infection (septic) | Otitis media/mastoiditis → lateral sinus; facial/orbital cellulitis → cavernous sinus; skull osteomyelitis |
| Systemic disease | Behçet disease, SLE, malignancy, IBD, nephrotic syndrome |
| Local factors | Head trauma, neurosurgery, intracranial tumors (meningioma, metastases) |
| Metabolic | Dehydration |
| Viral | SARS-CoV-2 (COVID-19), varicella zoster — immune-mediated thrombotic process |
| Vaccine-induced | VITT (vaccine-induced immune thrombocytopenia and thrombosis) — anti-PF4 antibodies mimicking HIT |
| Idiopathic | ~15–20% |
Pathophysiology
Thrombosis of a dural sinus → ↑ venous pressure upstream → impaired CSF reabsorption → raised ICP. If venous hypertension is severe → reduced parenchymal drainage → venous infarction, which is characteristically:
- Hemorrhagic (~1/3 develop intracerebral hemorrhage)
- Multifocal and bilateral, crossing arterial territories
- Involving both gray matter and subcortical white matter
Clinical Presentation
Onset can be acute, subacute, or chronic — this variability is a diagnostic trap.
| Feature | Frequency |
|---|---|
| Headache (progressive, over days–weeks) | Most common |
| "Thunderclap" headache (mimicking SAH) | Less common but important |
| Papilledema / raised ICP symptoms | Common |
| Seizures (focal or generalized) | ~40% |
| Focal neurological deficit (hemiparesis, paraparesis, aphasia) | Variable, depends on sinus |
| Altered mental status / encephalopathy | Common |
| Coma | ~14% |
| Visual obscurations | Common |
Superior sagittal sinus thrombosis → bilateral leg weakness and sensory changes (parasagittal cortex)
Cavernous sinus thrombosis (usually septic) → proptosis, chemosis, painful ophthalmoplegia
Lateral sinus thrombosis → headache, fever, otalgia, vertigo, papilledema, CN VI palsy
CVT should always be considered in patients with unexplained raised ICP / pseudotumor cerebri, or any unexplained hemorrhagic infarction.
Diagnosis
CT (non-contrast)
- Hyperdense cord/string sign — acutely thrombosed cortical vein or sinus
- Hemorrhagic infarction not conforming to an arterial territory
- Small ventricles
CT Venography (CTV)
- "Empty delta sign" — hypodense centre (thrombus) within an enhancing sinus wall on post-contrast CT
- Optimal for major dural sinus thrombosis
MRI + MR Venography (MRV)
- Gold standard — has replaced conventional angiography
- Loss of normal flow void in the sinus
- Thrombus may be hyperintense on T1 and T2 (subacute)
- SWI: "blooming" of thrombosed vein + prominent serpiginous collateral veins = venous congestion
- MRV: loss of flow signal / filling defect
Caution: very acute thrombus can appear hypointense on T2 (mimicking flow void); hypoplastic sinuses can also mimic thrombosis.
LP
- Elevated opening pressure supports the diagnosis in the right clinical setting
- LP can be safely performed in CVT
Workup
- All patients should undergo thrombophilia screen (protein C, S, antithrombin III, factor V Leiden, antiphospholipid antibodies, homocysteine, JAK2 mutation in suspected myeloproliferative disorders)
Imaging Gallery
Fig. 1 — Sagittal T1 MRI: Increased signal and enlargement of the superior sagittal sinus throughout most of its course = superior sagittal sinus thrombosis
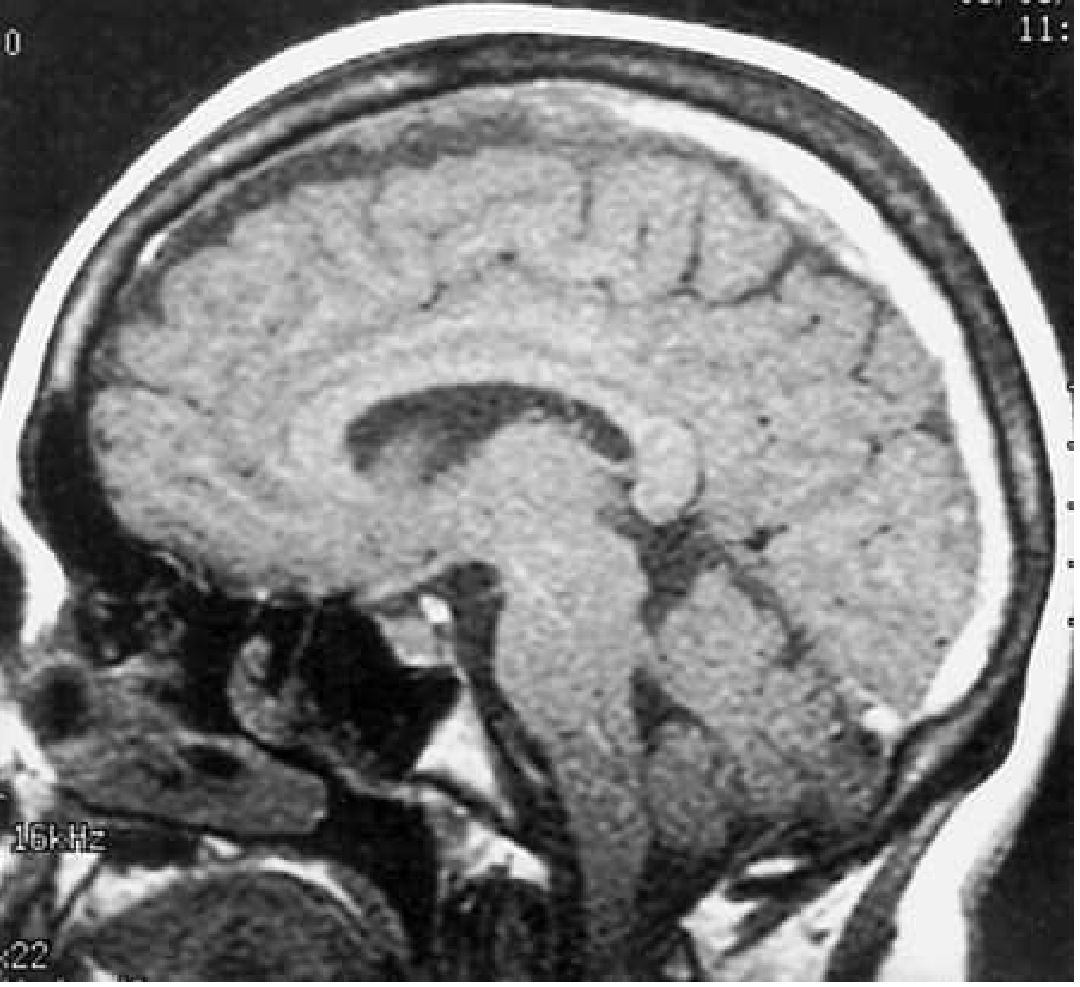
Unenhanced sagittal T1 MRI: area of increased signal and enlargement of the superior sagittal sinus consistent with thrombosis extending to the torcula. — Bradley & Daroff's Neurology, Fig. 65.35
Fig. 2 — Multimodal imaging of CVT: cortical vein thrombosis (right vein of Labbé) with string sign on CT (A–B), T2 venous ischaemia (C); left lateral sinus thrombosis with large parenchymal haemorrhage (D–F), T2/FLAIR sinus signal loss (G–H), CT venogram filling defect (I), and absent MRV flow signal (J)
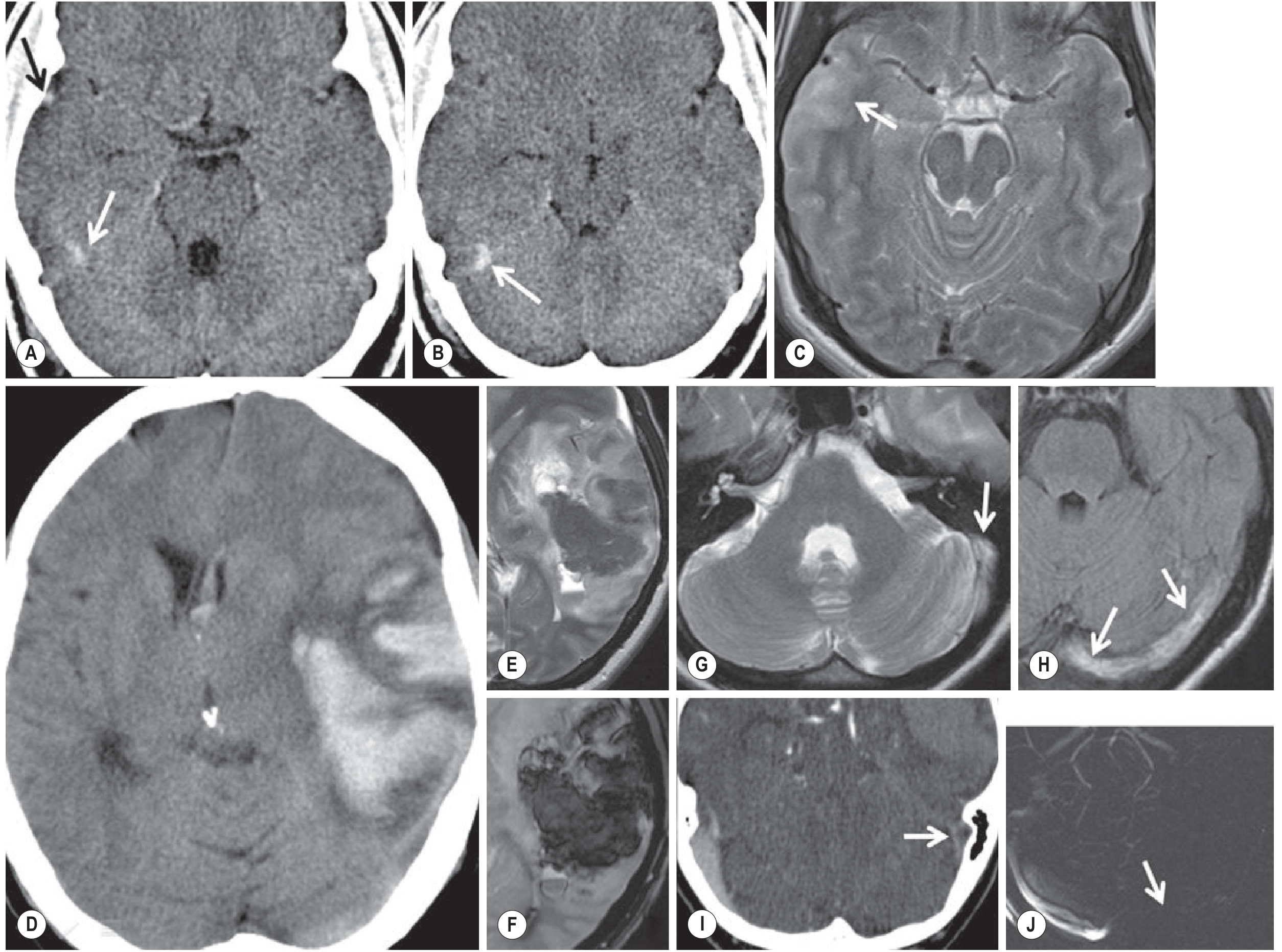
Fig. 56.28 — Grainger & Allison's Diagnostic Radiology: (A–C) cortical venous thrombosis of right vein of Labbé; (D–J) left lateral sinus thrombosis with haemorrhagic venous infarction, confirmed on CTV and MRV.
Fig. 3 — MR Venogram: absent flow in the right transverse and sigmoid sinus (arrowhead) with intact left-sided flow (arrows)
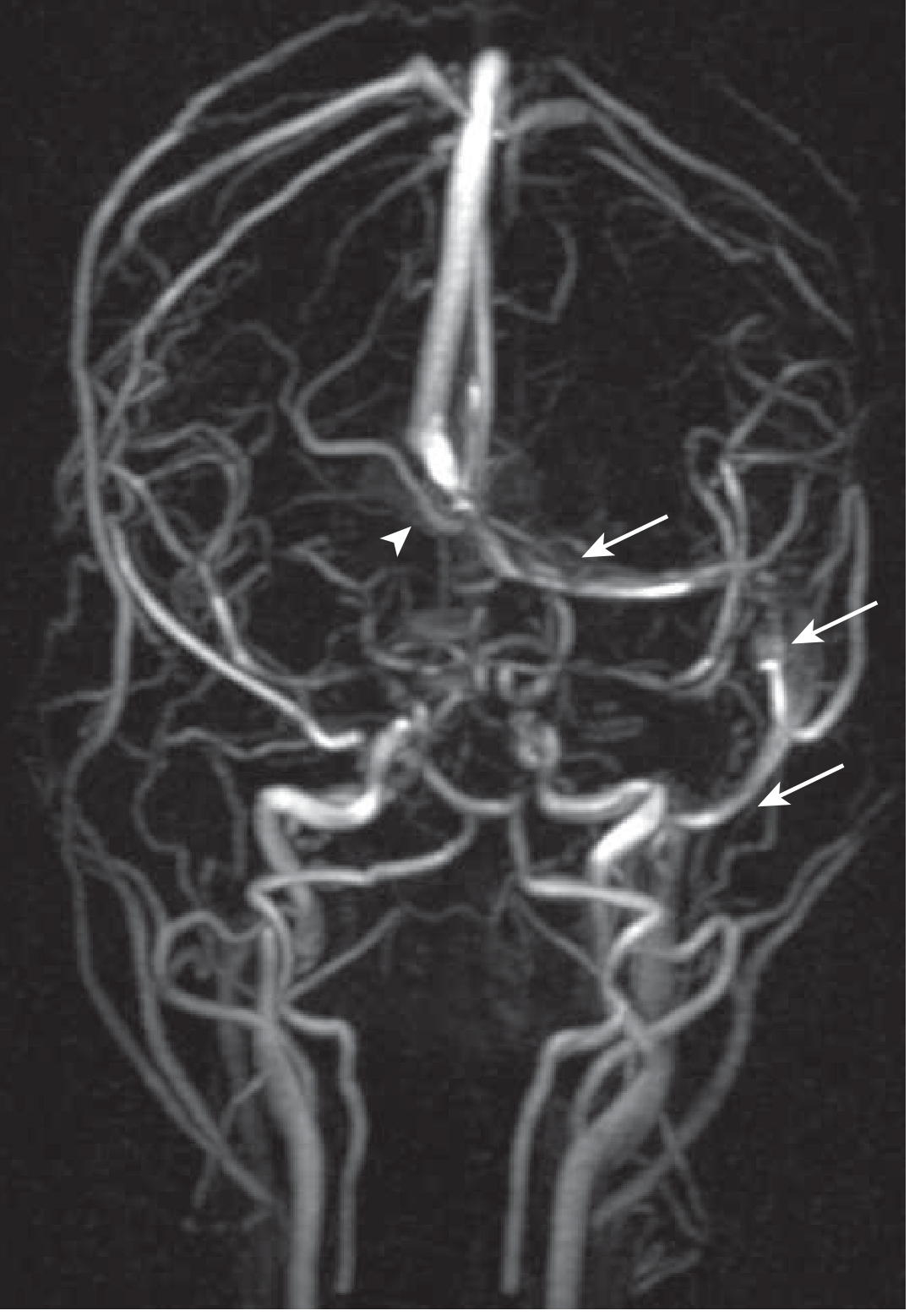
MR venogram: absent flow in right transverse sinus (arrowhead) and sigmoid sinus; intact left-sided flow (arrows). — Goldman-Cecil Medicine, Fig. 376-6
Treatment
Acute Anticoagulation
- IV unfractionated heparin or weight-adjusted subcutaneous LMWH — first-line
- Anticoagulation is indicated even in the presence of intracranial hemorrhage — evidence shows reduced thrombus propagation without increased bleeding risk
- One small RCT found LMWH associated with lower mortality vs. UFH
Duration of Anticoagulation
- Minimum 3 months; longer depending on underlying cause
- Transition to warfarin (INR 2.0–3.0) for oral anticoagulation
- DOACs (e.g., rivaroxaban): limited data in adults; a pediatric trial showed no significant difference vs. warfarin
Adjunctive Measures
- ICP management (acetazolamide, CSF diversion if severe)
- Antiepileptics — prophylactic in patients with seizures or at high risk
- Antibiotics — for septic CVT (e.g., cavernous sinus thrombosis)
Escalation / Refractory Cases
- Local thrombolytic infusion (intra-sinus tPA) and/or mechanical thrombectomy — reserved for clinical deterioration despite anticoagulation
- DSA catheter angiography used as a prelude to endovascular therapy
- Decompressive craniectomy — may be required in selective cases with malignant hemispheric edema and herniation risk
Prognosis
- Most patients have a favorable outcome with early anticoagulation
- Poor prognostic factors: deep sinus involvement, coma at presentation, large hemorrhagic infarction, male sex, older age, malignancy
- Recurrence risk is related to underlying thrombophilia; long-term anticoagulation is considered in those with persistent prothrombotic states
Sources:
- Bradley and Daroff's Neurology in Clinical Practice, Chapter 65
- Goldman-Cecil Medicine, Chapter 376
- Grainger & Allison's Diagnostic Radiology, Chapter 56
- Tintinalli's Emergency Medicine, Chapter 165
- Rosen's Emergency Medicine, Chapter 16
This is a shared conversation. Sign in to Orris to start your own chat.