explain me Liver function test frkom basic to clinical
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have all the material needed for a comprehensive answer. Let me compose the full explanation.
Liver Function Tests (LFTs): From Basic to Clinical
LFTs are a panel of blood tests used to detect liver injury, assess severity, monitor disease progression, and guide further workup. Despite the name, many of them reflect hepatocellular injury or cholestasis rather than true "function." True synthetic function is assessed by albumin, prothrombin time (PT/INR), and coagulation factors.
1. Basic Liver Physiology (Why These Tests Matter)
The liver performs hundreds of functions:
- Metabolism of carbohydrates, lipids, proteins
- Synthesis of albumin, clotting factors (I, II, V, VII, IX, X, XI), cholesterol
- Detoxification of drugs, alcohol, ammonia
- Bilirubin conjugation and excretion into bile
- Bile production for fat absorption
When the liver is damaged, its cellular constituents (enzymes) leak into blood, its synthetic capacity drops, and bile flow is disrupted. LFTs capture all three.
2. Bilirubin Metabolism (The Foundation)
Understanding bilirubin is key to understanding LFTs.
Step 1 - Production (Pre-hepatic):
- Heme from senescent RBCs is broken down → biliverdin → unconjugated (indirect) bilirubin
- Unconjugated bilirubin is lipid-soluble, bound to albumin in blood - it cannot be filtered by kidneys, so it does NOT appear in urine
Step 2 - Hepatic processing (3 steps):
- Uptake: The bilirubin-albumin complex reaches the hepatocyte; bilirubin dissociates and enters the cell
- Conjugation: Bilirubin + glucuronic acid (via UDP-glucuronosyltransferase) → conjugated (direct) bilirubin - now water-soluble
- Excretion: Hepatocyte pumps conjugated bilirubin into bile canaliculi - this is the rate-limiting step
Step 3 - Post-hepatic (intestinal):
- Conjugated bilirubin → duodenum → colon bacteria convert it to urobilinogen
- Urobilinogen: partly excreted in stool as stercobilin (makes stool brown), partly reabsorbed and excreted in urine (small amounts normal)
Clinical Rule:
- Conjugated (direct) hyperbilirubinemia → water-soluble → appears in urine → "dark urine" (bilirubinuria); pale/clay-colored stool (bile not reaching gut)
- Unconjugated (indirect) hyperbilirubinemia → albumin-bound → NOT in urine; normal stool color
- Jaundice becomes visible at the frenulum/sclera at serum bilirubin ≥ 2.5 mg/dL, and in skin at ≥ 5 mg/dL
Normal total bilirubin: < 1.2 mg/dL (normally >90% is unconjugated)
3. The Individual Tests
3a. Bilirubin (Total, Direct, Indirect)
| Fraction | Source | Key Conditions |
|---|---|---|
| Total bilirubin | Sum of both | Liver disease, hemolysis, obstruction |
| Direct (conjugated) | Processed by liver | Cholestasis, obstruction, hepatocellular disease |
| Indirect (unconjugated) | Not yet processed | Hemolysis, Gilbert syndrome, Crigler-Najjar, neonatal jaundice |
- Pre-hepatic (e.g., hemolysis): indirect ↑, direct normal
- Hepatocellular (e.g., hepatitis): both fractions elevated (liver can't take up, conjugate, or excrete)
- Post-hepatic/obstructive (e.g., choledocholithiasis): direct ↑ prominently
3b. Aminotransferases (AST and ALT) - Markers of Hepatocellular Injury
These enzymes are released when hepatocytes are damaged or die.
AST (Aspartate Aminotransferase)
- Found in: liver, heart, skeletal muscle, kidney, RBCs
- Less specific for liver - elevated also in MI, rhabdomyolysis
- Normal: 10-40 U/L
ALT (Alanine Aminotransferase)
- Found predominantly in: liver cytoplasm
- More specific for liver disease
- Normal: 7-56 U/L
Clinical Interpretation:
| Magnitude of elevation | Likely cause |
|---|---|
| >10x upper reference limit (URL) | Acute hepatitis (viral, ischemic, drug-induced) |
| 3-10x URL | Chronic hepatitis, alcoholic hepatitis |
| <3x URL with AST > ALT | Cirrhosis, alcoholic liver disease |
The AST:ALT Ratio:
- AST:ALT > 2:1 strongly suggests alcoholic liver disease (alcohol depletes pyridoxal phosphate needed for ALT synthesis; AST is also released from mitochondria in alcohol-damaged cells)
- AST:ALT < 1 is typical of viral hepatitis and NAFLD
- In cirrhosis, the ratio tends toward >1 even without alcohol
Important Pearl: In acute viral hepatitis, ALT rises significantly days before jaundice appears.
3c. Alkaline Phosphatase (ALP) - Marker of Cholestasis
- Location: Expressed on bile duct epithelium (canalicular membrane), also bone osteoblasts, placenta, intestine
- Mechanism of elevation: In biliary obstruction/cholestasis, ALP synthesis increases and enzyme is released into serum
- Half-life: ~7 days - levels may lag behind resolution of obstruction
- Normal: 44-147 U/L (varies by age/sex)
Causes of elevated ALP:
- Hepatobiliary: bile duct obstruction (choledocholithiasis, cholangiocarcinoma, PSC), intrahepatic cholestasis, PBC, drug-induced cholestasis, liver metastases, space-occupying lesions
- Non-hepatic: bone disease (Paget's, bone metastases, fractures, hyperparathyroidism), pregnancy (placental isoform), growing children
How to confirm ALP is of liver origin: Check GGT (see below) or ALP isoenzyme fractionation. If GGT is elevated alongside ALP, the source is hepatobiliary.
3d. Gamma-Glutamyl Transferase (GGT) - Cholestasis Confirmatory Marker
-
Location: Liver (especially bile duct epithelium), kidney, pancreas
-
Sensitive for hepatobiliary disease but not specific
-
Key uses:
- Confirm hepatobiliary origin of elevated ALP
- GGT elevated in cholestasis with ALP = strongly cholestatic pattern
- GGT elevated without ALP elevation → suspect alcohol use or drug induction (GGT is a classic marker of chronic alcohol use)
- In suspected choledocholithiasis: sensitivity ~90%, specificity ~85%
-
Important: GGT levels increase earlier and persist longer than traditional LFTs in cholestatic disease
-
Also a prognostic marker - rising GGT over time is associated with type 2 diabetes, metabolic syndrome, and cardiovascular mortality
3e. Albumin - Marker of Chronic Synthetic Function
- Synthesized exclusively in the liver (~10 g/day)
- Half-life: 15-20 days - therefore a poor marker of acute liver dysfunction; reflects chronic impairment
- Normal: 3.5-5.0 g/dL
- Decreased in: cirrhosis, chronic hepatitis, malnutrition, nephrotic syndrome, protein-losing enteropathy, inflammatory states (albumin is a negative acute-phase reactant)
Clinical significance:
- Low albumin + prolonged PT = advanced/chronic liver disease with impaired synthetic capacity
- In the LFT diagnostic algorithm: decreased albumin in hepatocellular pattern = chronic hepatitis; normal albumin = acute hepatitis
3f. Prothrombin Time (PT) / INR - Marker of Acute Synthetic Function
- The liver synthesizes all clotting factors EXCEPT factor VIII
- Factor VII has the shortest half-life (~6 hours) - making PT/INR the most sensitive marker of acute hepatic synthetic failure
- PT/INR becomes abnormal only with significant hepatic impairment (the liver has large synthetic reserve)
- Normal PT: 11-13.5 seconds; Normal INR: 0.8-1.1
Critical distinction:
- Vitamin K deficiency also prolongs PT (factors II, VII, IX, X require vitamin K for γ-carboxylation) - can distinguish by giving IV vitamin K: a ≥30% improvement in PT = vitamin K deficiency, not liver failure
- In DIC, factor VIII is also low (unlike in liver disease where factor VIII is normal or increased, since it is made by endothelial cells)
Clinical uses:
- Prognostic scoring: INR is a component of MELD score (Model for End-Stage Liver Disease) along with creatinine and bilirubin - used to prioritize liver transplant allocation
- Prognosis in acute liver failure (acetaminophen toxicity, acute viral hepatitis)
- Prognosis in alcoholic hepatitis (part of Maddrey Discriminant Function)
3g. Total Protein and Globulins
- Total protein = albumin + globulins
- Increased globulins with decreased albumin = chronic liver disease (liver makes less albumin; plasma cells produce more immunoglobulins in chronic inflammation/cirrhosis)
- Albumin:Globulin (A:G) ratio reversal (<1) suggests chronic liver disease
3h. Lactate Dehydrogenase (LDH)
- Non-specific; present in liver, heart, muscle, RBCs
- Markedly elevated LDH with modest transaminase rise may suggest ischemic hepatitis ("shock liver") or hepatic malignancy
4. Pattern Recognition - The Clinical Core
This is how LFTs are used at the bedside. Two main patterns exist:
Hepatocellular Pattern
- ALT and AST >> ALP
- Liver parenchyma (hepatocytes) are injured
- Causes: viral hepatitis (A, B, C, E), alcoholic hepatitis, NAFLD/NASH, autoimmune hepatitis, drug-induced liver injury (e.g., acetaminophen), ischemic hepatitis, Wilson disease
Cholestatic Pattern
- ALP (+ GGT) >> ALT/AST
- Bile flow is obstructed (intra- or extrahepatic)
- Causes: choledocholithiasis, cholangiocarcinoma, PSC, PBC, drug-induced cholestasis (e.g., estrogens, chlorpromazine), pancreatic head tumor
Diagnostic Algorithms
From the Tietz Textbook of Laboratory Medicine:
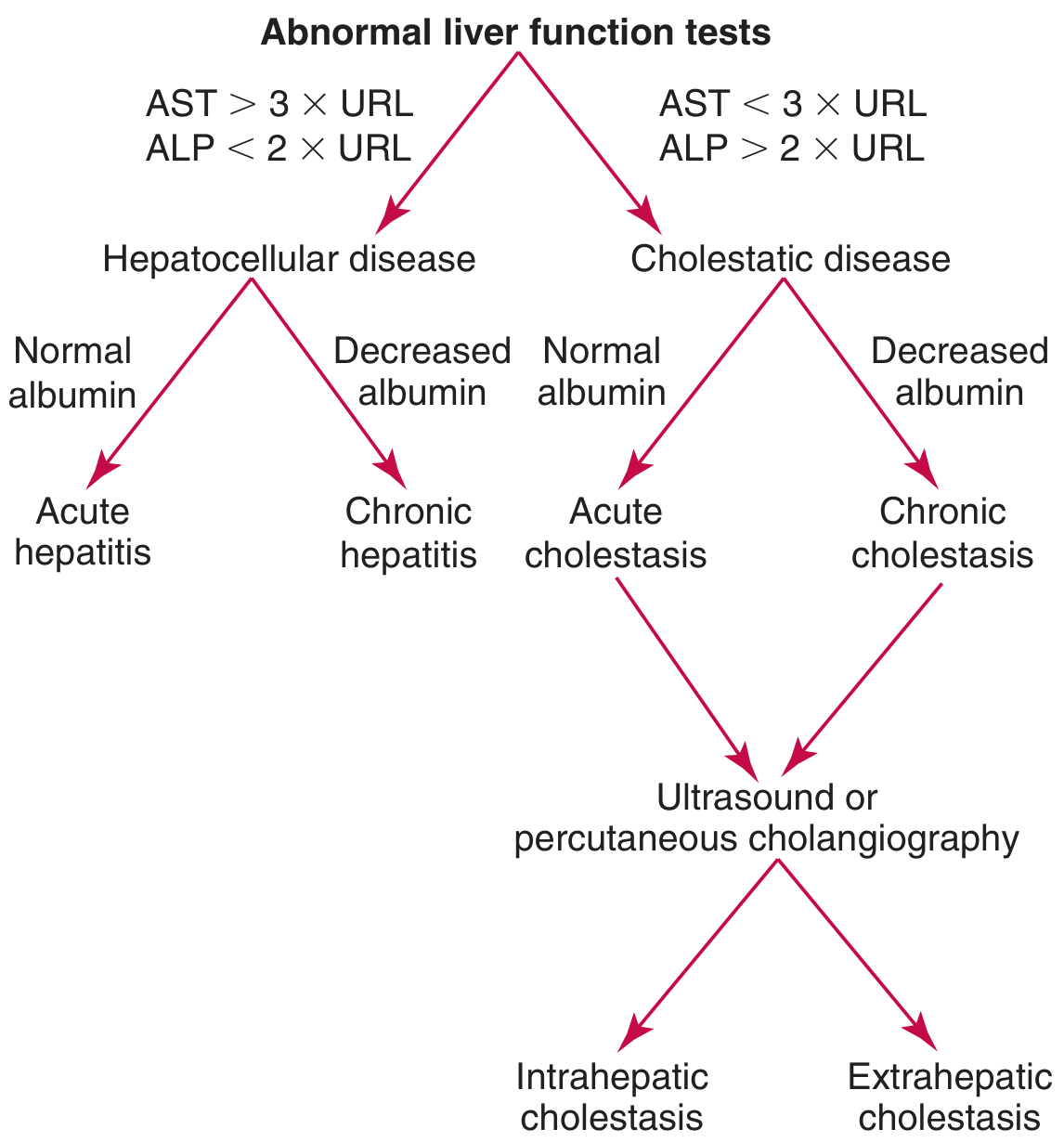
Figure: When AST > 3x URL with ALP < 2x URL = Hepatocellular disease. When ALP > 2x URL with AST < 3x URL = Cholestatic disease. Albumin then stratifies acute vs chronic.
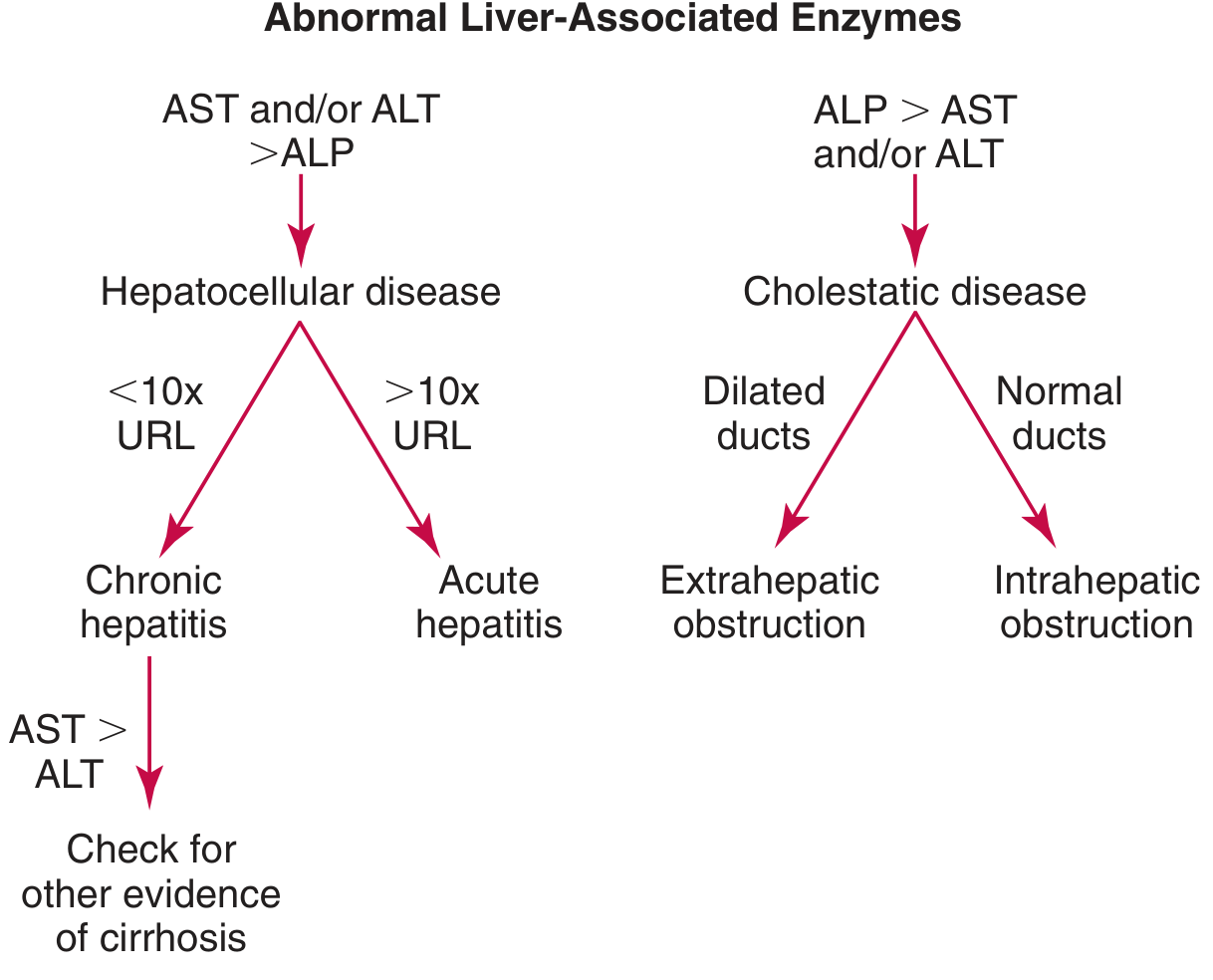
Figure: Hepatocellular pattern: >10x URL = acute hepatitis; <10x URL = chronic hepatitis. If AST > ALT = check for cirrhosis. Cholestatic pattern: dilated ducts = extrahepatic obstruction; normal ducts = intrahepatic cholestasis.
5. Summary Table of All LFTs
| Test | Normal Range | What it Reflects | Elevated In | Clinical Pearl |
|---|---|---|---|---|
| Total Bilirubin | <1.2 mg/dL | Liver excretion, hemolysis | Jaundice of any cause | >2.5 mg/dL = clinical icterus |
| Direct (Conjugated) Bilirubin | <0.3 mg/dL | Conjugation/excretion | Obstruction, hepatocellular | Appears in urine (dark urine) |
| Indirect Bilirubin | <1.0 mg/dL | Hemolysis, conjugation defects | Hemolysis, Gilbert, neonatal | NOT in urine |
| ALT | 7-56 U/L | Hepatocyte integrity (specific) | Hepatitis, NAFLD, drugs | Best marker of hepatocellular injury |
| AST | 10-40 U/L | Hepatocyte integrity (non-specific) | Hepatitis, alcohol, cardiac, muscle | AST:ALT >2 = alcoholic liver disease |
| ALP | 44-147 U/L | Bile duct epithelium, bone | Cholestasis, bone disease | Confirm with GGT to prove liver origin |
| GGT | 9-48 U/L | Bile canaliculi, microsomal induction | Cholestasis, alcohol, drugs | Confirms ALP is hepatic; rises early in cholestasis |
| Albumin | 3.5-5.0 g/dL | Chronic synthetic function | ↓ in cirrhosis, malnutrition | Half-life 15-20 days; not acute marker |
| PT/INR | PT 11-13.5s / INR <1.1 | Acute synthetic function | Acute/severe liver disease | Factor VII t½ = 6 hrs; used in MELD score |
6. Key Clinical Scenarios
Acute Viral Hepatitis: ALT > AST (both markedly elevated, often >10x URL), bilirubin elevated, ALP mildly elevated, albumin normal (acute, so synthetic function preserved unless fulminant), PT may be elevated in severe cases.
Alcoholic Hepatitis: AST:ALT ratio > 2:1 (but rarely >8x URL), GGT markedly elevated, bilirubin elevated, PT prolonged (Maddrey score uses PT to assess severity).
Obstructive Jaundice (e.g., gallstone in common bile duct): ALP and GGT markedly elevated, conjugated bilirubin predominates, dark urine + pale stools, AST/ALT mildly elevated (can be significantly elevated acutely).
Cirrhosis: ALT/AST mildly elevated (burnt-out liver), AST > ALT, low albumin, prolonged PT, elevated bilirubin in decompensation, low platelet count (from hypersplenism).
Non-Alcoholic Fatty Liver Disease (NAFLD/NASH): ALT > AST mildly elevated (usually 1-3x URL), ALP mildly elevated or normal.
Primary Biliary Cholangitis (PBC): ALP and GGT markedly elevated, anti-mitochondrial antibodies (AMA) positive.
Ischemic Hepatitis ("Shock Liver"): Massive AST and ALT rise (often >50x URL), LDH very high, improves rapidly with restoration of perfusion.
7. LFTs and the MELD Score
The MELD (Model for End-Stage Liver Disease) score uses:
- INR
- Total bilirubin
- Serum creatinine
It predicts 90-day mortality in cirrhosis and is used worldwide for liver transplant prioritization.
MELD = 3.78 × ln[bilirubin mg/dL] + 11.2 × ln[INR] + 9.57 × ln[creatinine mg/dL] + 6.43
8. A Practical Note on "LFTs are not really function tests"
As Sabiston's Textbook of Surgery notes, "standard liver function tests (LFTs) are generally NOT tests of function" - a critical distinction. Most tests (AST, ALT, ALP, GGT) measure hepatocyte injury or enzyme leakage, not liver capacity. Only albumin and PT/INR truly reflect the liver's functional reserve.
Sources:
- Harper's Illustrated Biochemistry, 32nd Ed
- Tietz Textbook of Laboratory Medicine, 7th Ed
- Schwartz's Principles of Surgery, 11th Ed
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed
- Sabiston Textbook of Surgery, p. 31-42
This is a shared conversation. Sign in to Orris to start your own chat.