A 22 yr old male presented with Chest pain at right parasternal area radiation to back which is throbbing in naturem. His BP was 150/80 mm hg in both arms . History of Vomiting present.What's the diagnosis and initial management?
Reading File
Checking Date & Time
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to give a comprehensive answer. Let me synthesize the clinical picture.
Diagnosis: Acute Aortic Dissection (most likely Type A / DeBakey Type I or II)
Clinical Reasoning
| Feature | Significance |
|---|---|
| 22-year-old male | Young age → think connective tissue disorder (Marfan syndrome, Ehlers-Danlos) |
| Throbbing chest pain at right parasternal area | Anterior chest pain is classic for ascending aorta involvement (Stanford Type A) |
| Radiation to the back | Hallmark of aortic dissection — pain follows the path of dissection |
| BP 150/80 mmHg in BOTH arms | Equal BPs do not exclude dissection; a difference >20 mmHg is more specific but absent in many confirmed cases |
| Vomiting | Vagal response to severe aortic pain; also seen with dissection extending to mesenteric vessels |
| Hypertension | The most common predisposing and presenting factor (hypertension in ~49% of IRAD patients) |
"Classically, dissection presents with abrupt and severe pain in the chest that radiates to an area between the scapulae... 60% of patients had anterior chest pain (more common in Stanford type A)" — Tintinalli's Emergency Medicine
Aortic dissection has a bimodal age distribution: the first peak involves younger patients with connective tissue disorders (Marfan syndrome, Ehlers-Danlos); the second peak is in those >50 years with hypertension. — Tintinalli's Emergency Medicine
"Younger individuals [are more likely to have] Marfan syndrome and other genetic diseases." — Braunwald's Heart Disease
Classification
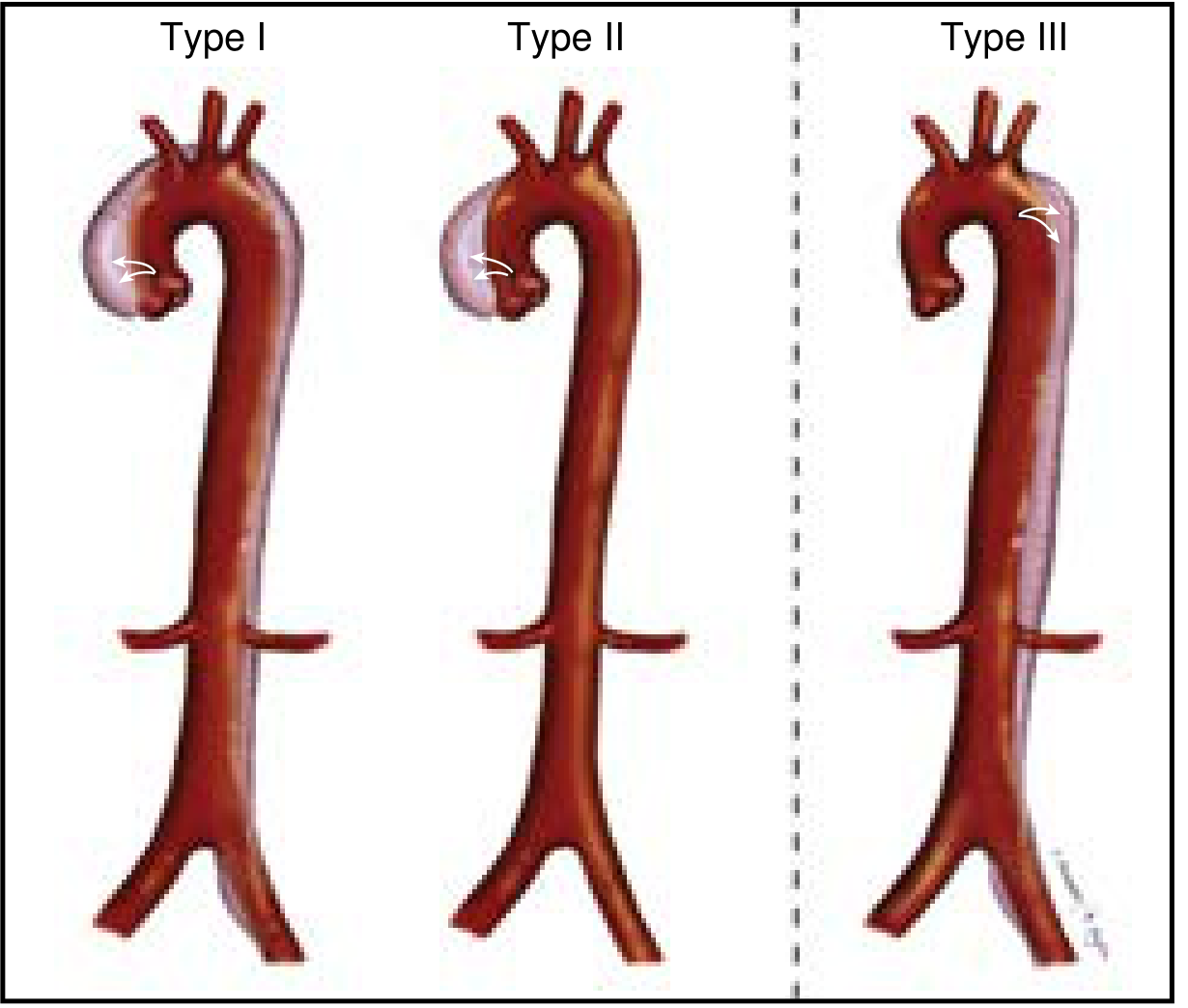
| Stanford | DeBakey | Anatomy | Management |
|---|---|---|---|
| Type A | Type I & II | Involves ascending aorta | Emergency surgery |
| Type B | Type III | Descending aorta only (distal to L subclavian) | Medical management ± TEVAR |
Given right parasternal pain + radiation to back, this is most consistent with Stanford Type A (ascending aorta ± arch/descending) — surgical emergency.
Aortic Dissection Detection (ADD) Risk Score
This patient scores ≥1 point (right parasternal/anterior chest pain + back radiation), which mandates immediate imaging workup.
Initial Management
1. Immediate Stabilization
- IV access × 2, continuous cardiac monitoring, pulse oximetry
- Baseline ECG (to exclude MI/ACS, also detects tamponade effects)
- Chest X-ray (widened mediastinum >8 cm is a classic but non-specific sign)
2. Pain Control
- IV opioid analgesia (morphine/fentanyl) — reduces sympathetic drive and catecholamine surge
3. Blood Pressure & Heart Rate Control (critical — the cornerstone of medical therapy)
Target: Systolic BP < 120 mmHg + Heart rate < 60 bpm within 30 minutes
Step 1 — Rate control FIRST (before vasodilators):
"Beta-blocker therapy should be initiated before vasodilation because the latter can lead to reflex tachycardia and worsening of dP/dt (rate of pressure rise)." — Rosen's Emergency Medicine
- Esmolol (preferred — short-acting, titratable): Bolus 500 mcg/kg IV → maintenance 0.05–0.2 mcg/kg/min
- Labetalol (alternative — α + β blockade): 20 mg IV q10 min boluses; note longer half-life (4–6 hours), less titratable
Step 2 — Add vasodilator once HR < 60 bpm:
- Sodium nitroprusside, nicardipine, or clevidipine (titrate to SBP ~100–120 mmHg)
4. Definitive Imaging
- CT Angiography (CTA) of the entire aorta — gold standard (sensitivity/specificity 90–100%), confirms diagnosis, classifies type, maps extent
- TEE — if hemodynamically unstable or renal contraindication to contrast; rapidly assesses tamponade, aortic valve, and wall motion
- MRI/conventional aortography have limited role in the acute setting
5. Definitive Treatment
- Stanford Type A → Emergency surgical repair (open surgery)
- Stanford Type B (uncomplicated) → Medical management (BP/HR control)
- Stanford Type B (complicated) → TEVAR (thoracic endovascular aortic repair)
6. Work up for Underlying Cause in This Young Patient
- Examine for Marfan stigmata: tall stature, arm span > height, arachnodactyly, lens dislocation, scoliosis, pectus excavatum, high-arched palate
- Genetics consult + FBN1/TGFBR2 mutation testing
- Echocardiogram for aortic root dimensions
- Screen family members
Key Points to Remember
- Do NOT give thrombolytics — if ACS is on the differential, exclude dissection first; thrombolytics in dissection are rapidly fatal
- Equal BP in both arms does NOT rule out dissection — only 15% have pulse/BP differentials
- Vomiting is a vagal response, not a distinguishing feature
- Cocaine use history must be asked in young patients — it is implicated in 0.5–37% of dissection cases
Sources: Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Braunwald's Heart Disease; Current Surgical Therapy 14e
History of shortness of breath present in above case
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
This is exactly what I needed. I now have a complete, well-sourced answer.
Impact of Shortness of Breath on the Case
Adding dyspnea (shortness of breath) to the clinical picture of a 22-year-old male with anterior chest pain radiating to the back strongly points toward Stanford Type A Aortic Dissection with a proximal complication — this is now a more urgent surgical emergency.
What Dyspnea Tells You: Proximal Complications of Type A Dissection
Schwartz's Principles of Surgery provides a highly relevant table of anatomical complications and their symptoms:
| Complication | Mechanism | Symptoms/Signs |
|---|---|---|
| Aortic Valve Insufficiency (AR) | Dissection disrupts aortic valve commissures → regurgitation | Dyspnea, diastolic murmur, pulmonary rales, shock |
| Pericardial Tamponade | Serosanguineous effusion from thin outer wall of dissected ascending aorta accumulates | Dyspnea, JVD, muffled heart sounds, pulsus paradoxus, low-voltage ECG |
| Coronary Malperfusion (usually RCA) | Dissection shears coronary ostia → acute MI | Chest pain, nausea/vomiting, shock, ECG changes |
"Ascending aortic dissection can directly injure the aortic valve, causing regurgitation... ranging from partial separation of one commissure... to complete prolapse of the valve into the left ventricle, producing severe acute heart failure. Patients with acute aortic valve regurgitation may report rapidly worsening dyspnea." — Schwartz's Principles of Surgery, 11e
"The thin and inflamed outer wall of a dissected ascending aorta often produces a serosanguineous pericardial effusion that can accumulate and cause tamponade. Suggestive signs include jugular venous distension, muffled heart tones, pulsus paradoxus, and low-voltage ECG." — Schwartz's Principles of Surgery, 11e
Most Likely Mechanism in This Case
In this 22-year-old with likely Marfan syndrome:
Aortic Dissection (Type A)
↓
Ascending Aorta involved
↓
┌───────────────────────────────┐
│ 1. Aortic Valve Disruption │→ Acute Aortic Regurgitation → Pulmonary Edema → Dyspnea
│ 2. Pericardial Effusion │→ Cardiac Tamponade → Dyspnea + Shock
│ 3. Coronary Ostial Shearing │→ Acute MI (usually RCA) → LV failure → Dyspnea
└───────────────────────────────┘
How Dyspnea Changes the Management
Additional Bedside Examination Priorities
- Auscultate for diastolic murmur (early decrescendo — acute AR from commissural disruption)
- Check JVD + pulsus paradoxus (>10 mmHg drop in SBP on inspiration → tamponade)
- Auscultate for bilateral basal crepitations (pulmonary edema from acute AR/LV failure)
Immediate Additional Investigations
| Test | Purpose |
|---|---|
| ECG | Low-voltage (tamponade), RCA territory changes (inferior STEMI from coronary malperfusion) |
| Bedside Echo/POCUS | Rapidly detect pericardial effusion, tamponade physiology, aortic regurgitation, LV function |
| CXR | Widened mediastinum, pleural effusion (left > right), cardiomegaly |
| CTA whole aorta | Definitive — confirms dissection, maps extent, detects complications |
Critical Management Adjustments
- If tamponade suspected — Do NOT pericardiocentesis (decompressing the pericardium removes the only thing preventing exsanguination into the pericardial sac; this is a surgical pericardiotomy decision)
- If acute AR with pulmonary edema — Avoid beta-blockers that increase regurgitant fraction; proceed urgently to surgery
- If inferior ST elevation on ECG — Do NOT give thrombolytics; this is coronary malperfusion from dissection, not primary ACS
Definitive Treatment
Emergency open surgical repair of the ascending aorta — this remains the treatment of choice for Stanford Type A. Surgery addresses:
- Resection of the intimal tear
- Aortic valve repair or replacement (if AR present)
- Pericardial decompression
- Coronary ostial reimplantation if needed
Summary: How Dyspnea Upgrades the Urgency
| Without Dyspnea | With Dyspnea Added |
|---|---|
| Aortic dissection suspected | Proximal complication (AR, tamponade, coronary malperfusion) strongly suspected |
| Urgent imaging | Emergent POCUS + simultaneous CTA |
| Controlled BP, prepare for surgery | Immediate surgical team activation |
| Time-sensitive | Minutes matter — do not delay |
Sources: Schwartz's Principles of Surgery 11e; Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.