In Alf stages of liver failure
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Here is a comprehensive overview of the stages of Acute Liver Failure (ALF):
Stages / Classification of Acute Liver Failure (ALF)
Definition
ALF is a clinical syndrome of sudden liver injury with:
-
Elevated transaminases
-
Coagulopathy (INR > 1.5)
-
Hepatic encephalopathy (mandatory for diagnosis)
-
No pre-existing liver disease
-
Illness duration < 26 weeks
-
Sabiston Textbook of Surgery, p.1069
Stage 1: Classification by Time Course (O'Grady Classification)
This is the primary staging system, based on the interval from onset of jaundice to encephalopathy:
| Stage | Time Interval | Features |
|---|---|---|
| Hyperacute | 0-7 days | Severe coagulopathy, high risk of cerebral edema - but better prognosis with spontaneous recovery |
| Acute | 8-28 days | Intermediate features |
| Subacute | 29 days to 12 weeks (some say up to 24 weeks) | Less coagulopathy, less cerebral edema - but worse prognosis without transplant, more portal hypertension |
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p.1836
- Sabiston Textbook of Surgery, p.1069
- Bailey and Love's Short Practice of Surgery, 28th Edition
Key clinical insight: The shorter the onset, the more likely cerebral edema develops - but paradoxically, patients also have better chances of spontaneous recovery. Subacute patients rarely develop cerebral edema but rarely recover without liver transplant.
Stage 2: Hepatic Encephalopathy Grading (West Haven Criteria)
Encephalopathy grading is critical for management decisions in ALF, including transplant listing:
| Grade | Clinical Features |
|---|---|
| Grade 1 | Euphoria or anxiety; decreased attention; impaired simple calculations; subtle personality change |
| Grade 2 | Decreased arousal; apathy; minimal disorientation when spoken to; subtle personality changes; asterixis (liver flap) |
| Grade 3 | Increasing difficulty to arouse; confusion; disorientation; drowsiness |
| Grade 4 | Coma - unresponsive to verbal stimuli |
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p.629 (West Haven Criteria)
Clinical significance of grading in ALF:
- Grade 3-4: Cerebral edema develops in ~80% of patients at Grade 4
- Grade 2 progression: Often used as a trigger to list for liver transplant
- Grade 3-4 + coagulopathy + acidosis: Meets King's College Criteria for urgent transplant listing
Key Complications by Stage
| Stage | Main Danger |
|---|---|
| Hyperacute / Grade 3-4 HE | Cerebral edema, raised ICP, cerebral herniation (>50% of ALF mortality) |
| Any grade | Coagulopathy, renal failure, sepsis, hemodynamic instability, hypoglycemia |
| Subacute | Portal hypertension > cerebral edema |
Older Terminology
| Old Term | Meaning |
|---|---|
| Fulminant hepatic failure | Encephalopathy within 8 weeks of jaundice (broadly used) |
| Subfulminant hepatic failure | Liver disease up to 26 weeks before encephalopathy |
| Hyperacute | Within 1 week (most severe, best chance of recovery) |
- Current Surgical Therapy, 14th Edition
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Summary: Why Staging Matters
- Transplant urgency - Grade 2+ encephalopathy guides listing; Grade 3-4 with King's College Criteria = urgent (Status 1A)
- ICP monitoring - Initiated at Grade 3-4 due to cerebral edema risk
- Prognosis - Hyperacute has the best spontaneous recovery despite being the most dramatic; subacute has the worst without transplant
- Management approach - Grade 3-4 patients need head-of-bed elevation, sedation, hypertonic saline (target Na 150-155 mEq/L), and avoidance of nephrotoxic drugs
Paracetamol poisoning stages
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a complete breakdown of paracetamol (acetaminophen) poisoning stages:
Paracetamol (Acetaminophen) Poisoning - Stages
Mechanism First
Normal metabolism: ~90% conjugated to glucuronide + sulfate (safe). ~5-15% oxidized via CYP2E1 to the toxic metabolite NAPQI (N-acetyl-p-benzoquinoneimine), which is neutralized by glutathione.
In overdose: Glucuronidation and sulfation pathways saturate. More drug is shunted to CYP2E1 → massive NAPQI production → glutathione stores fall below 30% of normal → NAPQI binds covalently to hepatocyte proteins → centrilobular hepatic necrosis.
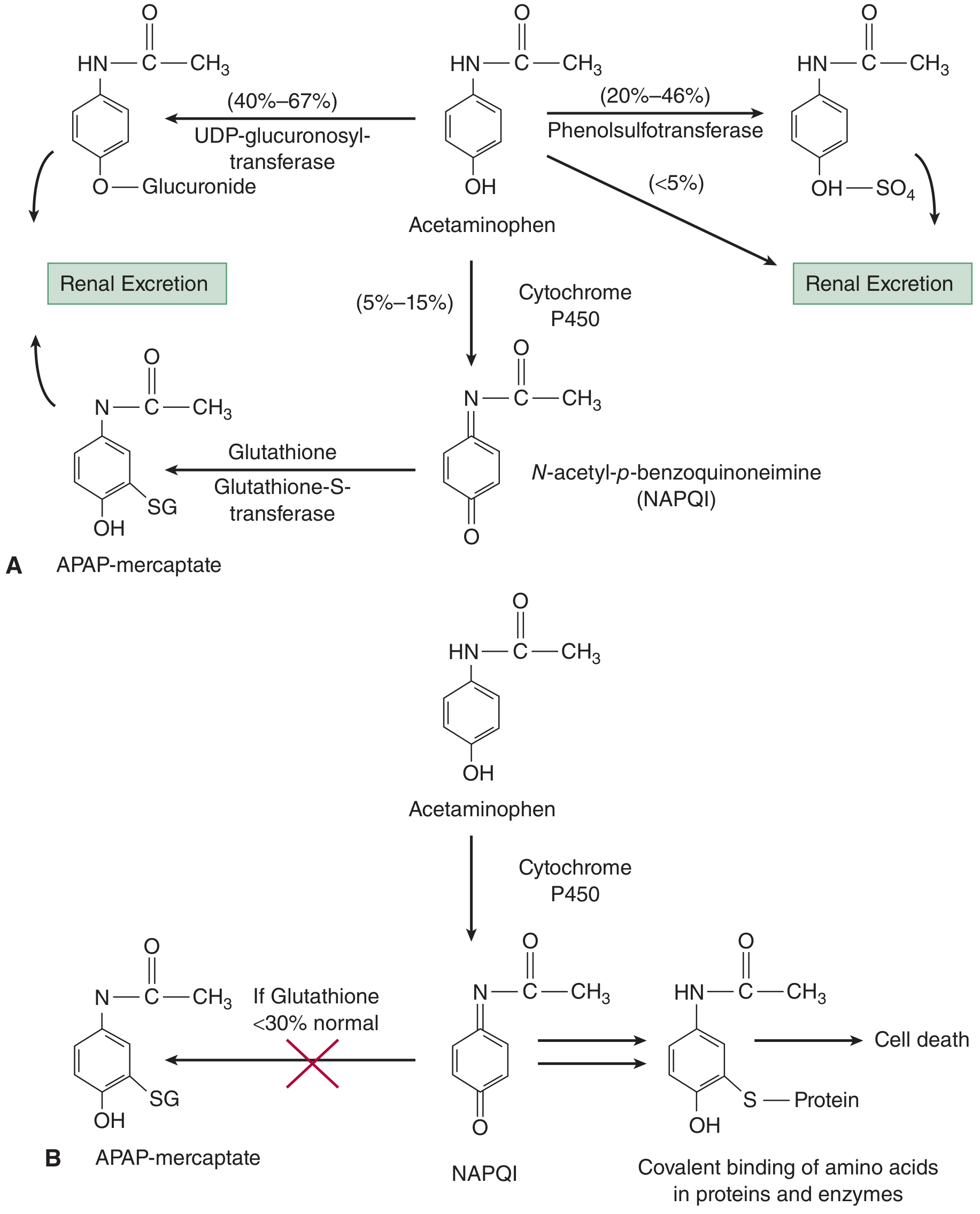
NAC (N-acetylcysteine) acts as a glutathione precursor, replenishing stores to detoxify NAPQI.
The Four Clinical Stages
| Stage | Timeframe | Clinical Features |
|---|---|---|
| Stage I | 0-24 hours | Nausea, vomiting, anorexia, malaise, pallor, diaphoresis. Often asymptomatic; LFTs usually normal |
| Stage II | 24-72 hours | Stage I symptoms improve; right upper quadrant pain and tenderness appears; rising AST/ALT and bilirubin; prolonged PT; possible early renal involvement |
| Stage III | 72-96 hours | Peak hepatotoxicity: jaundice, coagulopathy, hypoglycemia, hepatic encephalopathy, renal failure, metabolic acidosis, possible multi-organ failure - highest mortality |
| Stage IV | 4-14+ days | Clinical improvement if patient survives; gradual normalization of liver function; full recovery possible due to liver regeneration (complete in 1-3 months) |
- The Essentials of Forensic Medicine and Toxicology, 36th Edition (2026)
- Tintinalli's Emergency Medicine, Table 190-1
Key Points Per Stage
Stage I (0-24 h) - "Deceptive calm"
- The patient may look well despite a lethal ingestion
- LFTs are still normal - do NOT falsely reassure
- Action: Measure serum paracetamol level at 4 hours post-ingestion, plot on Rumack-Matthew nomogram, start NAC if indicated
Stage II (24-72 h) - "Biochemical injury"
- Hepatocyte lysis releases transaminases: AST/ALT begin to rise
- Right upper quadrant tenderness is the first clinical sign of hepatotoxicity
- Most patients with mild-moderate hepatotoxicity recover if NAC started in time
Stage III (72-96 h) - "Fulminant failure"
- AST/ALT can reach >10,000 IU/L in severe cases
- Cerebral edema risk if encephalopathy develops (Grade 3-4)
- King's College Criteria for transplant listing applies here:
- Arterial pH < 7.30 (after resuscitation), OR
- All three: PT > 100 sec + creatinine > 300 µmol/L + Grade III/IV encephalopathy
Stage IV (4-14 days) - "Recovery or death"
- The liver has remarkable regenerative capacity if the patient survives Stage III
- Complete histological and functional recovery is possible, even after severe necrosis
Risk Factors for Enhanced Toxicity
These groups develop toxicity at lower doses because of increased CYP2E1 activity or reduced glutathione:
- Chronic alcohol use (CYP2E1 is induced by alcohol)
- Malnutrition / fasting (depleted glutathione stores)
- CYP450-inducing drugs: phenytoin, carbamazepine, rifampin
Postmortem Findings (Forensic)
-
Centrilobular hepatic necrosis
-
Acute tubular necrosis (kidneys)
-
Myocardial damage
-
Cerebral edema
-
The Essentials of Forensic Medicine and Toxicology, 36th Edition (2026)
Treatment Summary
| Intervention | Detail |
|---|---|
| Activated charcoal | Within 1-2 hours of ingestion; reduces absorption |
| NAC (oral) | Loading 140 mg/kg, then 70 mg/kg q4h × 17 doses; most effective within 8-10 hours |
| NAC (IV) | 150 mg/kg over 1 hr → 50 mg/kg over 4 hr → 100 mg/kg over 16 hr (21-hr regimen) |
| Methionine | Oral glutathione precursor; alternative when NAC unavailable |
| Liver transplant | Severe acidosis, PT > 100 sec, creatinine > 300 µmol/L |
This is a shared conversation. Sign in to Orris to start your own chat.