Spinal fusion Orthopaedics 10 marks along with recent advances
"spinal fusion"[MeSH Terms] AND "recent advances"
"spinal fusion" AND "minimally invasive" OR "robotics" OR "biologics"
"lumbar spinal fusion"[MeSH Terms] AND "robotic" OR "navigation" OR "augmented reality"
"spinal fusion" AND "bone morphogenetic protein" OR "3D printing" OR "expandable cage"
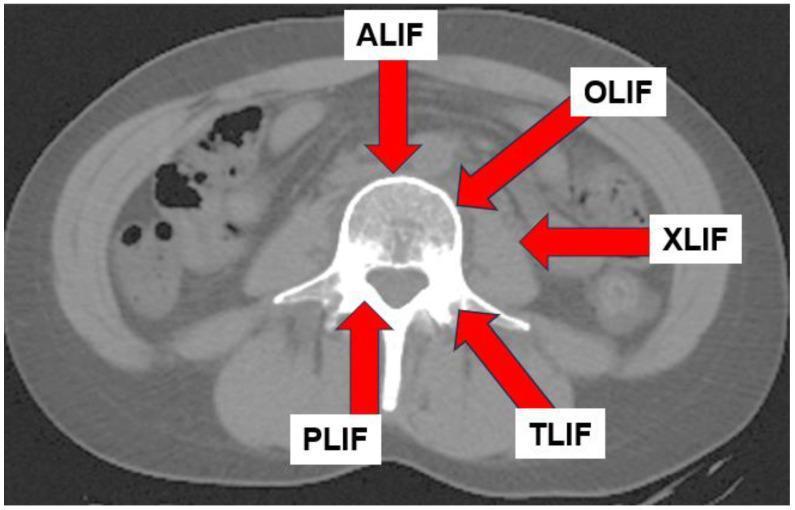
spinal fusion techniques PLIF TLIF ALIF diagram
Spinal Fusion — Orthopaedics (10 Marks)
Definition
Indications
| Category | Examples |
|---|---|
| Degenerative | Degenerative spondylolisthesis, degenerative disc disease causing intractable pain, lumbar instability |
| Traumatic | Unstable vertebral fractures with/without neurological deficit, fracture nonunion |
| Deformity | Scoliosis, kyphosis (structural correction and stabilisation) |
| Infective | Spinal tuberculosis (Pott's disease), pyogenic spondylodiscitis |
| Neoplastic | Primary/metastatic tumour with spinal instability after corpectomy |
| Iatrogenic | Post-laminectomy instability, failed back surgery syndrome with instability |
| Inflammatory | Rheumatoid arthritis with atlantoaxial subluxation >4 mm; subaxial subluxation |
Principles of Spinal Fusion
- Osteoconduction — scaffold for bone ingrowth
- Osteoinduction — growth factors stimulating new bone formation (e.g., BMPs)
- Osteogenesis — living cells capable of forming bone
Approaches and Techniques
1. Posterior Approaches
- Bone graft laid over transverse processes and facet joints
- Combined with decompressive laminectomy for neural decompression
- Standard treatment for degenerative spondylolisthesis
- Bilateral discectomy via posterior midline approach
- Interbody cage/graft placed in disc space + pedicle screw fixation
- Allows direct decompression but requires significant retraction of nerve roots
- Associated with paraspinal muscle atrophy on long-term MRI
- Unilateral posterolateral approach through the intervertebral foramen
- Less nerve root retraction than PLIF
- Can be performed as minimally invasive (MIS-TLIF) with preservation of paraspinal muscles
- Preferred technique in most centres; recent advances in technique and technology reviewed in Neurosurg Clin N Am 2025 (PMID 39542545)
2. Anterior Approaches
- Retroperitoneal approach to L4–L5 and L5–S1
- Excellent disc space distraction and large graft/cage contact area
- Avoids posterior musculature; risk of vascular and sympathetic chain injury
- Often combined with posterior instrumentation (360° fusion)
3. Lateral/Oblique Approaches
- Direct lateral transpsoas or prepsoas approach
- Avoids anterior vessels and posterior muscles
- Cannot access L5–S1 due to iliac crest
- Oblique anterolateral approach, avoids psoas and its lumbar plexus
4. Cervical Approaches
- Standard approach for cervical radiculopathy/myelopathy
- Anterior plate + interbody graft/cage
- Lateral mass screws or cervical pedicle screws with rod fixation
- Used in multilevel myelopathy, rheumatoid instability, trauma
Bone Grafts and Substitutes
| Type | Advantages | Disadvantages |
|---|---|---|
| Autograft (iliac crest) | Gold standard — osteogenic, osteoinductive, osteoconductive | Donor site morbidity, limited supply |
| Allograft (femoral ring, fibular strut) | No donor site morbidity | No osteogenicity, disease transmission risk |
| Demineralised Bone Matrix (DBM) | Preserves BMP, osteoinductive | Variable potency between preparations |
| Calcium phosphate ceramics (HA, TCP) | Osteoconductive scaffold | No osteogenicity |
| rhBMP-2 (recombinant BMP) | Powerful osteoinduction | Cost; risk of ectopic ossification, osteolysis, seroma |
| Synthetic PEEK/titanium cages | Immediate load-bearing, MRI compatible | Stress shielding (PEEK); artifact on CT (titanium) |
Instrumentation
- Pedicle screws and rods: Most commonly used posterior construct; enhanced pullout strength with larger diameter screws
- Cement-augmented pedicle screws: For osteoporotic spine — PMMA or calcium phosphate injected through cannulated/fenestrated screws
- Anterior cervical plates: Used in ACDF
- Interspinous devices: Adjunct to motion preservation
Complications
Early
- Haemorrhage, CSF leak, infection (superficial or deep)
- Neurological injury, dural tear
Late
- Pseudarthrosis (non-union): 1–15% depending on level and construct; highest at thoracolumbar junction and L5–S1; risk factors — smoking, diabetes, obesity, multilevel fusion, poor bone quality. Suspect on imaging if >4 mm translation or >10° angular motion on dynamic X-rays
- Adjacent Segment Disease (ASD): Accelerated degeneration above/below fused levels due to altered biomechanics; treated with extension of fusion
- Hardware failure: Screw loosening (peri-implant lucency on CT), rod fracture, cage migration
- Junctional fractures: Especially in osteoporotic spine
- Failed Back Surgery Syndrome (FBSS): Persistent or recurrent pain after technically successful surgery
Imaging Assessment of Fusion
- Plain radiographs: Flexion-extension views — <4 mm translation and <10° angulation indicates probable fusion
- CT: Most sensitive for bony trabeculae bridging; identifies pseudarthrosis, hardware loosening
- MRI: Assesses adjacent segment pathology, infection, neural compression from migrated hardware
Recent Advances
1. Robotic-Assisted Spinal Surgery
- Systems: Mazor X Stealth, ROSA Spine, ExcelsiusGPS
- Real-time intraoperative navigation for pedicle screw placement
- Improved accuracy (>95% Gertzbein grade A/B vs ~90% freehand), reduced radiation exposure, lower revision rates
- Systematic review of robotic systems 2025 (World Neurosurg, PMID 39864806): improved accuracy, comparable adverse events vs conventional
2. Augmented Reality (AR) Navigation
- AR headsets (e.g., HoloLens-based systems) overlay real-time 3D screw trajectories onto the surgical field
- Systematic review 2024 (Eur Spine J, PMID 38177834): AR-assisted pedicle screw placement achieves comparable or superior accuracy to CT navigation
- Eliminates need for physical tracking arrays; surgeon sees trajectory without looking away from the field
3. Image-Guided Spine Surgery (IGSS)
- Intraoperative CT (O-arm) or flat-panel fluoroscopy with navigation
- Allows real-time 3D confirmation of screw position before final tightening
- Reviewed in Neurosurg Clin N Am 2024 (PMID 38423733)
4. Minimally Invasive Surgery (MIS)
- MIS-TLIF: Tubular retractors, percutaneous pedicle screws → less blood loss, shorter hospital stay, faster rehabilitation, preserved paraspinal musculature
- Endoscopic lumbar interbody fusion (ELIF/endoscopic TLIF): Fully endoscopic approach; emerging evidence
- OLIF and XLIF: Less invasive lateral corridors avoiding posterior muscle stripping
5. Expandable Interbody Cages
- Collapsed cage inserted through narrow corridor then expanded in situ
- Allows larger footprint and better sagittal alignment correction without wide exposure
- Available in TLIF, ALIF, and lateral configurations
6. 3D-Printed Patient-Specific Implants
- Titanium cages with trabecular architecture manufactured by additive printing
- Match patient-specific anatomy; porous surface promotes osseointegration
- Reduced stress shielding compared to solid titanium
7. Biologic Enhancements
- Platelet-rich plasma (PRP) and mesenchymal stem cells (MSCs): Adjunct to bone grafting; early clinical evidence for improved fusion rates
- BMP-2 (INFUSE®): FDA-approved for ALIF at L4–L5; widespread off-label use; concerns about ectopic bone, osteolysis at high doses
- Parathyroid hormone (teriparatide): Perioperative use in osteoporotic patients shown to improve fusion rates and reduce hardware failure
8. Cement-Augmented and Novel Fixation Techniques
- SAIF (Stent-Screw-Assisted Internal Fixation): Combines vertebral body stent insertion with cement augmentation through cannulated fenestrated pedicle screws — preserves height and prevents cement leakage in severe osteoporotic fractures — Rockwood & Green's, 10th ed.
9. Sagittal Alignment Optimisation
- Modern spinal fusion incorporates spinopelvic parameter planning: pelvic incidence (PI), lumbar lordosis (LL), pelvic tilt (PT), sacral slope (SS)
- Target: LL = PI ± 9°; mismatch predicts proximal junctional kyphosis and revision surgery
- Current concepts review 2025 (J Am Acad Orthop Surg, PMID 40549931)
10. Motion-Preserving Alternatives
- Total disc arthroplasty (TDA): Comparable 2-year outcomes to ALIF for single-level L4–L5/L5–S1 disease; avoids fusion; concerns about long-term durability and revision access
- Dynamic stabilisation: Interspinous devices (Coflex, X-STOP) and dynamic rods — adjuncts to decompression without rigid fusion; role still evolving
Key Points for 10-Mark Answer
- Definition: Bony union between vertebral segments to achieve stability
- Indications: Spondylolisthesis, trauma, deformity, infection, neoplasm, iatrogenic instability
- Approaches: PLF, PLIF, TLIF, ALIF, XLIF, OLIF, ACDF, posterior cervical fusion
- Bone graft hierarchy: Autograft (gold standard) → allograft → synthetic substitutes → BMPs
- Instrumentation: Pedicle screw-rod constructs; cement augmentation for osteoporosis
- Complications: Pseudarthrosis, adjacent segment disease, hardware failure, infection, FBSS
- Assessment of fusion: Dynamic X-rays, CT (gold standard), MRI
- Recent advances: Robotics, AR navigation, MIS techniques, expandable cages, 3D-printed implants, biologics (BMP, MSC), sagittal alignment planning
Canal stenosis lumbar and cervical recent advances
"lumbar spinal stenosis"[MeSH Terms] AND treatment
"cervical stenosis"[MeSH Terms] AND "myelopathy" AND management
"lumbar stenosis" AND "decompression" AND outcomes
"cervical myelopathy" AND surgery AND outcomes
"laminoplasty" OR "laminectomy" AND "cervical stenosis" AND "outcomes"
"degenerative cervical myelopathy" AND "surgical treatment"
"lumbar stenosis" AND "interspinous" OR "minimally invasive decompression"
lumbar spinal stenosis MRI axial cross section neurogenic claudication