

1000103279.jpg
1000103281.jpg
Ans for university exams
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I now have enough from the library plus my anatomical knowledge to give complete, exam-quality answers to all 7 questions. Here are the full answers:
University Exam Answers
Question 5 (5×2 marks)
5a. Why does cavernous sinus thrombosis cause paralysis of extrinsic muscles of the eye?
Reason:
The cavernous sinus is a venous sinus located on either side of the body of the sphenoid bone. Running through or within its lateral wall are the following cranial nerves that supply the extrinsic (extraocular) muscles of the eye:
| Nerve | Course | Muscle supplied |
|---|---|---|
| CN III (Oculomotor) | Lateral wall of cavernous sinus | Superior rectus, inferior rectus, medial rectus, inferior oblique, levator palpebrae |
| CN IV (Trochlear) | Lateral wall of cavernous sinus | Superior oblique |
| CN VI (Abducens) | Directly within the sinus (most vulnerable) | Lateral rectus |
When thrombosis (clot formation) occurs in the cavernous sinus, it causes compression and ischemia of these nerves as they pass through or alongside the sinus. This results in ophthalmoplegia - paralysis of the extrinsic eye muscles, producing diplopia (double vision), ptosis, and inability to move the eye in various directions.
- CN VI palsy occurs first (it lies freely within the sinus and is most vulnerable)
- CN III and IV are also affected as thrombosis extends
- Total unilateral ophthalmoplegia results in complete paralysis of all extrinsic eye muscles
(Bradley and Daroff's Neurology; Scott-Brown's Otorhinolaryngology Vol 1)
5b. Why does chronic middle ear infection (chronic otitis media) cause paralysis of facial muscles?
Reason:
The facial nerve (CN VII) has a very close anatomical relationship with the middle ear:
- After entering the internal acoustic meatus, the facial nerve passes through the facial canal (Fallopian canal) in the petrous part of the temporal bone.
- It runs along the medial wall of the middle ear (tympanic cavity), where it forms the genu (bend) and passes just above the oval window.
- It then turns downward and exits through the stylomastoid foramen.
In chronic otitis media (CSOM), especially with cholesteatoma:
- The chronic infection and associated erosion of bone destroys the thin bony covering (dehiscence) of the facial canal.
- Cholesteatoma (keratinized epithelium) directly erodes the bony canal wall.
- Inflammatory mediators, pus, and granulation tissue compress and invade the exposed nerve.
- This leads to lower motor neuron (LMN) facial palsy - paralysis of all ipsilateral facial muscles (both upper and lower face), including inability to close the eye, drooping of the corner of the mouth, loss of nasolabial fold, etc.
(Cummings Otolaryngology; Textbook of Family Medicine 9e)
Question 3 - Short Answer Questions (Applied) (5×2 marks)
Q3a. Why is parotid swelling very painful?
Reason:
The parotid gland is enclosed within a tough, dense, fibrous capsule derived from the investing layer of deep cervical fascia. This capsule is inelastic and non-distensible.
- When the gland swells (due to infection - parotitis, mumps, abscess, calculus, etc.), it cannot expand outward because the capsule cannot stretch.
- The swelling therefore builds up pressure within the confined space, compressing the parotid tissue, blood vessels, and nerve endings intensely.
- The auriculotemporal nerve and other sensory fibers within and around the gland are compressed, generating severe pain.
- The pain is aggravated by chewing because mastication (jaw movements) further squeezes and mechanically stimulates the already-tense gland.
This is why parotid swelling (e.g., in mumps) is characteristically much more painful than swelling of other salivary glands whose capsules are less rigid.
(Color Atlas of Human Anatomy Vol 2)
Q3b. Infection of which paranasal air sinus is most difficult to treat, and why?
Answer: The maxillary sinus (antrum of Highmore)
Reasons why it is most difficult to treat:
-
Position of the ostium (drainage opening): The natural ostium of the maxillary sinus opens into the middle meatus of the nasal cavity at its upper medial wall - near the roof of the sinus, not the floor. Since gravity cannot assist drainage (pus collects at the floor but drains from the roof), secretions accumulate.
-
Dependent drainage problem: The floor of the maxillary sinus is lower than its ostium, so mucopurulent secretions pool at the bottom and cannot drain naturally by gravity.
-
Small, narrow ostium: The natural ostium is small (~3mm) and easily becomes blocked by mucosal edema during infection, further impairing drainage.
-
Access difficulty: Surgical access requires either a Caldwell-Luc operation (via canine fossa) or functional endoscopic sinus surgery (FESS), both more involved than for other sinuses.
-
Dental root proximity: The roots of upper molar and premolar teeth are closely related to the floor - dental infections easily spread to this sinus (dental sinusitis), and vice versa.
Q3c. Bleeding into which layer of the scalp causes "black eye," and why?
Answer: The 3rd layer - the Subaponeurotic (loose areolar) layer
The scalp has 5 layers (mnemonic: SCALP):
- S - Skin
- C - Connective tissue (dense)
- A - Aponeurosis (epicranial/galea aponeurotica)
- L - Loose areolar tissue
- P - Pericranium
Why bleeding in the loose areolar layer causes black eye:
- The loose areolar layer (Layer 4) is also called the "dangerous layer of the scalp" - it contains emissary veins and loose connective tissue with no fibrous septa to limit spread.
- Blood and fluid in this layer can spread freely in all directions without any barrier.
- Anteriorly, this layer is continuous with the loose connective tissue of the eyelids and orbital region (because the galea aponeurotica is attached anteriorly to the frontalis muscle which has no bony attachment anteriorly, allowing the plane to extend forward over the forehead and orbital margins).
- Blood tracking forward through this plane gravitates into the periorbital region, producing the classic bilateral black eye (periorbital ecchymosis/raccoon eyes).
This is why a scalp haematoma in this layer presents with delayed bruising around the eyes, even without direct orbital trauma.
Q3d. Which area of the face is known as the "danger area of the face," and why?
Answer: The central part of the face - the "Dangerous Triangle" or "Danger Triangle"
This is the triangular area with:
- Apex: at the root of the nose (between the two eyebrows)
- Base: at the upper lip (along the line connecting the two corners of the mouth)
It encompasses the nose, upper lip, and the nasolabial region.
Why it is dangerous:
The facial veins in this region are valveless and have communications with the cavernous sinus via:
- Angular vein → Ophthalmic vein (superior and inferior) → Cavernous sinus
- Deep facial vein → Pterygoid plexus → Cavernous sinus
Because the facial veins lack valves, blood (and infection) can flow in either direction - from the face backward into the intracranial cavernous sinus.
Consequences:
- Squeezing a boil/furuncle or superficial infection in this area can drive infected thrombi into the cavernous sinus via retrograde flow.
- This causes cavernous sinus thrombosis - a life-threatening condition with features of:
- High fever, septicemia
- Proptosis, chemosis, ophthalmoplegia
- Meningism, and risk of death
This is why any infection (boil, carbuncle, abscess) in the danger triangle should never be squeezed and must be treated with systemic antibiotics.
Q3e. A patient with carcinoma of the tongue presents with pain in the ear. Explain its anatomical basis.
Anatomical Basis: Referred pain via the lingual nerve and auriculotemporal nerve
This is a classic example of referred pain through shared nerve pathways.
Nerve supply of the tongue:
- The anterior 2/3 of the tongue receives general somatic sensation from the lingual nerve (branch of CN V3 - mandibular division of trigeminal).
- The posterior 1/3 of the tongue receives sensation from CN IX (glossopharyngeal).
Nerve supply of the ear:
- The external acoustic meatus and auricle receive sensory supply from the auriculotemporal nerve (also a branch of CN V3).
- CN IX also supplies the inner aspect of the tympanic membrane (Jacobson's nerve).
Mechanism of referred pain:
- In carcinoma of the anterior 2/3 of the tongue, the tumor invades and irritates the lingual nerve (CN V3).
- Since the lingual nerve and the auriculotemporal nerve are both branches of the same parent nerve (CN V3 - mandibular), their central pain fibers converge on the same neurons in the trigeminal nucleus (nucleus of the spinal tract of V).
- The brain incorrectly interprets the pain signal as coming from the ear (auriculotemporal distribution) when it actually originates from the tongue.
- This is classic referred otalgia (referred ear pain).
For posterior 1/3 carcinoma, pain is referred to the ear via CN IX (Jacobson's nerve supplying tympanic membrane).
(S Das - A Manual on Clinical Surgery 13th Ed)
Clinical importance: Referred otalgia in a patient with no obvious ear pathology should always prompt examination of the tongue, floor of mouth, tonsil, and larynx to rule out malignancy.
Summary Table for Quick Revision:
| Question | Key Answer |
|---|---|
| 5a | CN III, IV, VI pass through/alongside cavernous sinus → thrombosis compresses them → ophthalmoplegia |
| 5b | Facial nerve runs in facial canal on medial wall of middle ear → CSOM erodes bony canal → LMN facial palsy |
| Q3a | Tough inelastic parotid capsule cannot expand → raised pressure → pain on chewing |
| Q3b | Maxillary sinus - ostium near roof, floor below ostium, no gravity drainage |
| Q3c | Loose areolar layer (Layer 4) - blood spreads forward to eyelids → black eye |
| Q3d | Danger triangle of face - valveless facial veins communicate with cavernous sinus |
| Q3e | Lingual nerve (V3) irritated by tumor → referred to auriculotemporal nerve (also V3) → pain felt in ear |
Blood brain barrier Short note
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete short note on the Blood-Brain Barrier, exam-ready with diagram:
Blood-Brain Barrier (BBB)
Definition
The blood-brain barrier is a highly selective structural and functional barrier between the blood circulating in cerebral capillaries and the brain tissue (extracellular fluid of the CNS). It maintains the optimal microenvironment for normal neuronal function by tightly regulating what enters and exits the brain.
Historical Note
Over 100 years ago, it was observed that vital dyes injected into the bloodstream stained nearly all organs except the brain - this was the first description of the BBB. Modern microscopy and molecular biology have since revealed its precise structure.
Structural Components
The BBB consists of three layers working together:
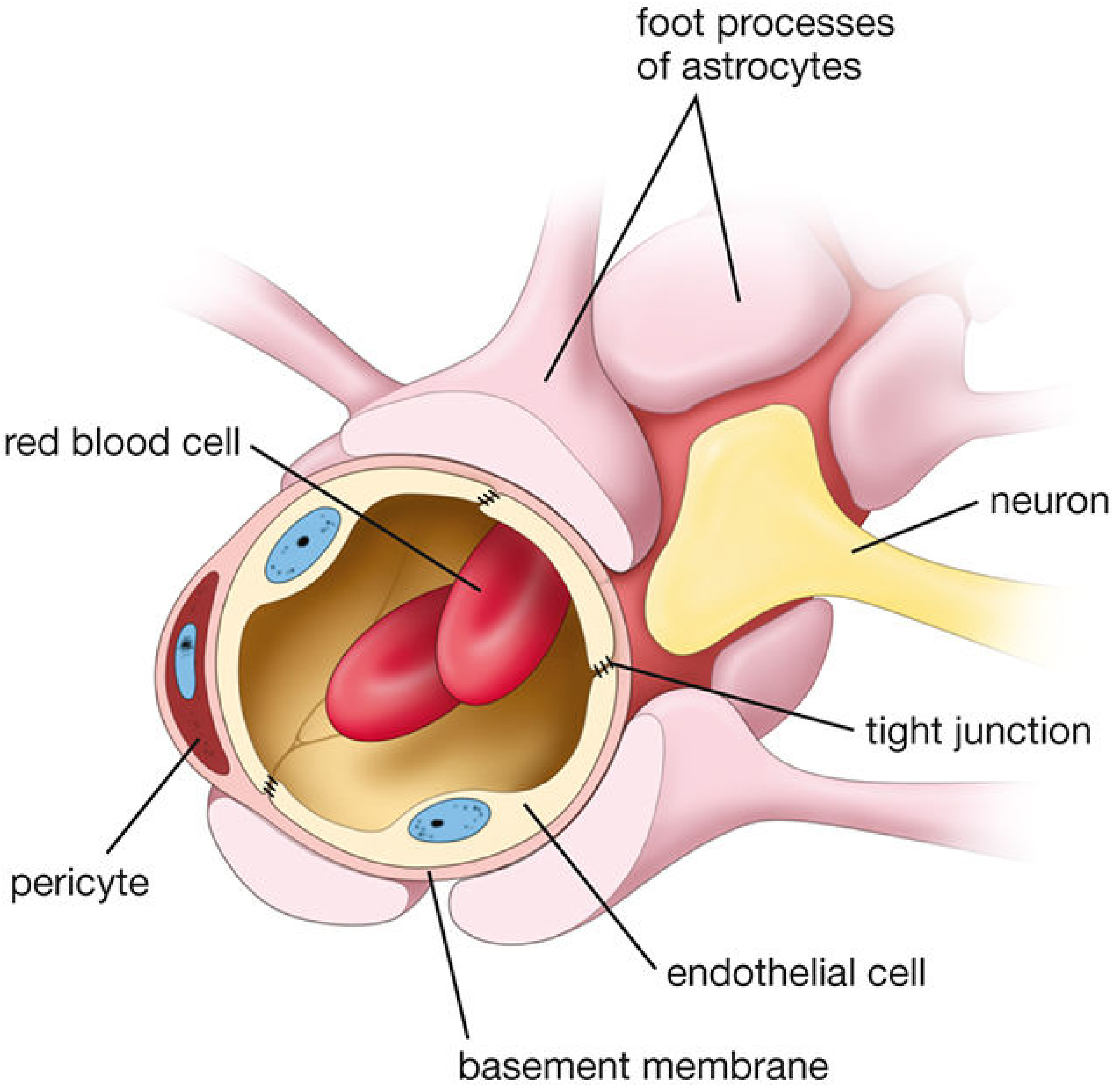
| Component | Role |
|---|---|
| Endothelial cells (with tight junctions) | Principal barrier - fused junctions, no pores, minimal pinocytosis |
| Basement membrane | Structural support; with pericytes embedded in it |
| Astrocyte perivascular end-feet (foot processes) | Regulate tight junction integrity via soluble factors; wrap around capillary |
Key structural features:
- Tight junctions (zonula occludens) between adjacent endothelial cells - these are complex, resembling epithelial junctions more than typical endothelial junctions. They eliminate intercellular gaps and prevent paracellular diffusion.
- Minimal pinocytosis - very few vesicles in endothelial cells; transcytosis is severely restricted.
- Continuous-type capillaries (no fenestrations) throughout the CNS.
- Pericytes embedded in the basement membrane help regulate the barrier.
(Histology: A Text and Atlas - Eroschenko; Goldman-Cecil Medicine)
Functions
- Protect the brain from blood-borne toxins, pathogens, and fluctuating levels of electrolytes, hormones, and metabolites.
- Maintain homeostasis of the CNS microenvironment (optimal ionic composition for action potentials).
- Meet metabolic demands of the brain by regulating transport of nutrients.
Permeability - What Crosses and What Doesn't
Freely crosses:
- O₂ and CO₂ (lipid-soluble gases) - by simple diffusion
- Lipid-soluble substances - anaesthetic agents, alcohol, steroids (freely enter)
- Water - moves freely by bulk flow
Crosses with help (carrier-mediated):
- Glucose - via facilitated transport (GLUT-1 transporter); glucose is the brain's sole energy source
- Amino acids - via specific transporters
- Certain drugs - via active transport or facilitated diffusion
Does NOT cross (or crosses poorly):
- Hydrophilic (polar) and large molecules (molecular weight >500 Da)
- Ionized substances (e.g., Na⁺ - equilibration half-life is 2-4 hours)
- Proteins and large polar molecules
- Mannitol - does not cross; used clinically to draw water out of the brain (osmotic diuresis)
- Most antibiotics and many chemotherapy drugs (a major clinical problem)
Development
The BBB develops early in embryonic life through interaction between glial astrocytes and capillary endothelial cells. Astrocytes release soluble factors that increase barrier properties and tight junction protein content - loss of astrocyte function leads to BBB breakdown.
Disruption of the BBB
The BBB can be disrupted (broken down) by:
- Severe hypertension
- Tumors (cerebral metastases, gliomas)
- Trauma (head injury)
- Stroke (ischemia - endothelial cell compromise)
- Infections (meningitis, encephalitis)
- Marked hypercapnia or hypoxia
- Sustained seizure activity
When disrupted, fluid movement becomes dependent on hydrostatic pressure rather than osmotic gradients, leading to vasogenic cerebral oedema.
Circumventricular Organs - Areas WITHOUT a BBB
Certain brain regions lack a complete BBB (called circumventricular organs):
- Area postrema (chemoreceptor trigger zone - vomiting)
- Posterior pituitary (neurohypophysis)
- Pineal gland
- Median eminence
- Subfornical organ
These regions require direct access to blood-borne signals (hormones, toxins).
Clinical Significance
| Clinical Context | Relevance |
|---|---|
| Drug delivery to brain | Most drugs cannot cross - challenge in treating brain tumors, CNS infections |
| Mannitol | Does not cross BBB; used to reduce raised ICP by osmosis |
| Lipid-soluble drugs | Anaesthetics, anticonvulsants - cross readily |
| Cerebral oedema | BBB breakdown → vasogenic oedema |
| Contrast MRI | Normal brain does not enhance; BBB breakdown shown by contrast enhancement (tumors, abscess) |
| Meningitis | Inflammation increases BBB permeability - allows some antibiotics to cross |
Summary (Quick Recall)
BBB = Endothelial tight junctions + Basement membrane + Astrocyte foot processes
- Allows: O₂, CO₂, lipid-soluble molecules, glucose (GLUT-1), water
- Blocks: large molecules (>500 Da), polar/ionized substances, proteins, mannitol
- Broken by: hypertension, trauma, tumors, infection, ischemia, hypoxia
- Absent at: circumventricular organs
(Goldman-Cecil Medicine; Morgan & Mikhail's Clinical Anesthesiology 7e; Histology: A Text and Atlas)
This is a shared conversation. Sign in to Orris to start your own chat.