Difference between immediate release and modified release
immediate release vs modified release drug formulations pharmacokinetics
Immediate Release (IR) vs Modified Release (MR) Formulations
Definitions
| Feature | Immediate Release (IR) | Modified Release (MR) |
|---|---|---|
| Definition | Releases drug rapidly after administration with no intentional delay | Alters the rate, extent, or site of drug release compared to a conventional dose |
| Goal | Rapid onset of action | Controlled, delayed, or prolonged delivery |
| Abbreviations | None (plain tablet/capsule) | ER, XR, XL, SR, CR, LA, DR, etc. |
Types of Modified Release
- Extended Release (ER / XR / XL) - drug is released slowly over many hours, maintaining steady plasma levels
- Sustained Release (SR) - drug release is prolonged but not necessarily at a constant rate
- Controlled Release (CR) - drug is released at a predictable, near-constant rate to maintain stable plasma concentrations
- Delayed Release (DR) - release is intentionally postponed (e.g., enteric-coated tablets that bypass the stomach and release in the intestine)
- Targeted Release - drug is directed to a specific anatomical location (e.g., colon-targeted formulations in IBD)
Pharmacokinetic Differences
| PK Parameter | Immediate Release | Modified Release |
|---|---|---|
| Onset of action | Rapid (minutes to ~1 hour) | Delayed or gradual |
| Tmax | Short | Extended |
| Peak plasma level (Cmax) | High, sharp spike | Lower, flatter |
| Duration of action | Short | Prolonged |
| Trough levels | May fall below therapeutic range | Maintained above therapeutic minimum |
| Dosing frequency | Multiple times per day (TID, QID) | Once or twice daily |
Clinical Implications
- Faster onset - useful for acute/breakthrough symptoms (e.g., IR morphine for breakthrough pain, IR nifedipine for hypertensive urgency)
- Easier to titrate dose quickly
- Can be crushed or split if needed
- Fewer daily doses - better patient adherence
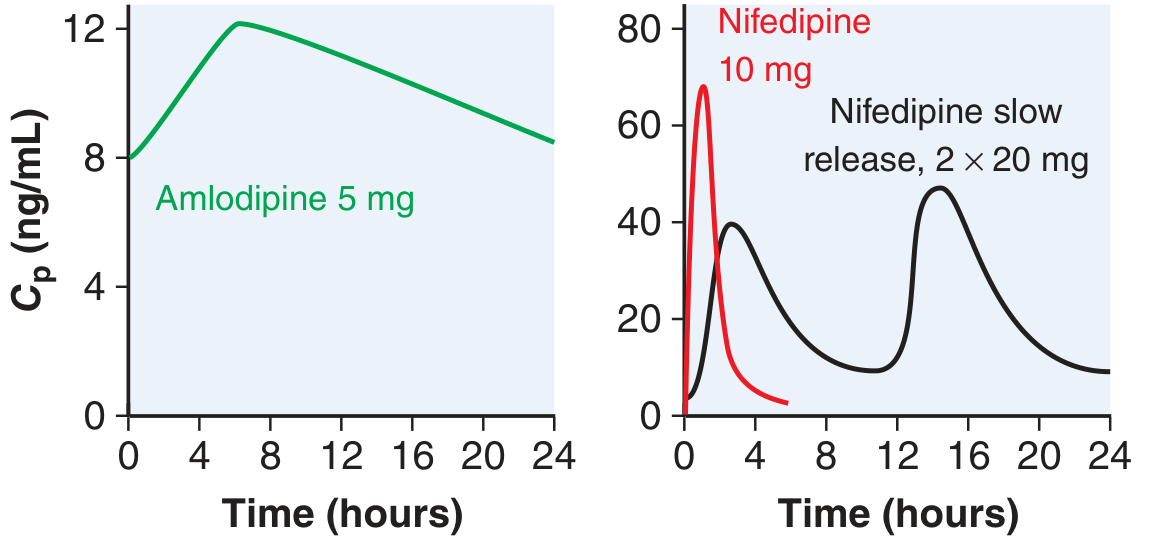
- Smoother plasma levels - reduces peak-related side effects (e.g., IR nifedipine causes reflex tachycardia and flushing due to abrupt drop in BP; SR nifedipine avoids this, as noted in Goodman & Gilman)
- Protects gastric mucosa (enteric-coated formulations)
- Better for drugs with short half-lives that would otherwise require frequent dosing (e.g., metoprolol, metformin, venlafaxine)
- Cannot be crushed, cut, or chewed - doing so destroys the release mechanism and may cause dose dumping (dangerously high, rapid release)
- Slower onset - not suitable for acute rescue therapy
- More expensive
- In overdose, absorption is delayed, prolonging toxicity - Goodman & Gilman specifically notes that modified-release preparations "will influence the time to the drug's peak concentration and result in delayed symptoms" in the context of drug overdose management
Mechanism of Modified Release
- Matrix systems - drug embedded in a slowly eroding polymer matrix
- Reservoir systems - drug core surrounded by a rate-controlling membrane
- Osmotic pump (OROS) - osmosis drives drug release through a laser-drilled hole at a constant rate
- Enteric coating - pH-sensitive coating that resists gastric acid and dissolves only in the alkaline intestine (e.g., enteric-coated aspirin, omeprazole delayed-release)
- Multi-particulate systems - capsules containing many small beads, each coated with a different release profile
Common Clinical Examples
| Drug | IR Form | MR Form | Reason for MR |
|---|---|---|---|
| Nifedipine | Capsule (short-acting) | Adalat LA / GITS | Avoid reflex tachycardia |
| Metformin | 500/850 mg tablet | 500/750/1000 mg XR | Reduce GI side effects |
| Metoprolol | Metoprolol tartrate | Metoprolol succinate (XL) | Once-daily dosing, better BP control |
| Morphine | Oral solution, Sevredol | MS Contin, Zomorph | Background pain control |
| Venlafaxine | Effexor (TID dosing) | Effexor XR (once daily) | Better tolerability |
| Omeprazole | Immediate-release | Delayed-release (enteric) | Protect capsule from gastric acid |
| Bupropion | 3x daily | SR / XL | Reduce seizure risk at high Cmax |
Key Safety Points
- Never crush MR tablets (except specific exceptions like some MUPS capsules that can be sprinkled)
- Dose dumping - if a MR tablet is cut, chewed, or crushed, the full dose releases at once - potentially fatal (e.g., oxycodone ER, diltiazem SR)
- In overdose, toxicity from MR preparations is delayed and prolonged - patients may appear well initially and deteriorate hours later (calcium channel blockers and bupropion MR are classic examples, per Goodman & Gilman)
Immediate release modified release difference
Immediate Release (IR) vs Modified Release (MR)
Core Difference
| Feature | Immediate Release | Modified Release |
|---|---|---|
| Release | Rapid, within minutes | Controlled - delayed, extended, or targeted |
| Onset | Fast | Slower/gradual |
| Cmax | High sharp peak | Lower, flatter |
| Duration | Short | Prolonged |
| Dosing | Multiple times/day | Once or twice daily |
| Can be crushed? | Yes | No - destroys release mechanism |
Types of MR
- Extended Release (ER/XR) - slow release over hours
- Sustained Release (SR) - prolonged release
- Controlled Release (CR) - near-constant rate
- Delayed Release (DR) - postponed release (e.g., enteric coating)
- Targeted Release - specific anatomical site
When to Use Which
- IR - acute/rescue therapy, fast titration needed
- MR - chronic conditions, adherence improvement, reducing peak side effects
Key Safety Rule
Is extended release and prolonged release same or extended and sustained release same
extended release vs prolonged release vs sustained release pharmacopeia definition difference
https://www.pharmaguideline.com/2018/01/difference-between-s…
Are Extended Release and Prolonged Release the Same?
| Term | Used By | Meaning |
|---|---|---|
| Extended Release (ER/XR/XL) | USP (US Pharmacopeia), FDA | Drug release extended over a longer time than IR |
| Prolonged Release (PR) | European Pharmacopoeia (Ph. Eur.), WHO | Same concept - drug release prolonged beyond IR |
Are Extended Release and Sustained Release the Same?
| Feature | Extended Release (ER) | Sustained Release (SR) |
|---|---|---|
| Rate of release | Gradual, may not be perfectly uniform | Controlled, more uniform/constant rate |
| Plasma curve | Gradual prolonged decline - flatter than IR | Flat plateau - maintains steady concentration |
| Primary goal | Prolong the duration of action | Maintain drug levels within the therapeutic window |
| Fluctuation | Some peak-trough fluctuation still possible | Minimal fluctuation |
| Mechanism | Slow dissolution or matrix erosion | Controlled diffusion, osmotic pump, or erosion |
- SR targets a flat, steady-state concentration (like a constant infusion mimicked in oral form)
- ER simply extends the time drug is above therapeutic levels, but levels may still rise and fall
The Full Hierarchy - How They All Fit Together
Modified Release (MR)
├── Extended Release = Prolonged Release (same thing, different regions)
│ ├── Sustained Release (SR) - subset with particularly flat plasma curve
│ └── Controlled Release (CR) - most precise, near zero-order kinetics
├── Delayed Release (DR) - postponed onset, e.g. enteric coating
└── Targeted Release - specific GI site
Quick Summary
| Pair | Same or Different? |
|---|---|
| Extended Release vs Prolonged Release | Same - just USP vs Ph. Eur. terminology |
| Extended Release vs Sustained Release | Mostly same in practice; SR implies a flatter, more constant plasma profile in strict theory |
| Sustained Release vs Controlled Release | CR is more precise (zero-order kinetics); SR may have some variation |
Difference between sustained and controlled release
sustained release vs controlled release difference zero order kinetics pharmacology
https://www.colorcon.com/education-insights/controlled-vs-su…
Sustained Release (SR) vs Controlled Release (CR)
The Core Distinction
| Feature | Sustained Release (SR) | Controlled Release (CR) |
|---|---|---|
| Definition | Releases drug slowly over a prolonged period | Releases drug at a precise, predictable, programmed rate |
| Release kinetics | Primarily first-order - rate decreases over time as drug is depleted | Primarily zero-order - constant amount released per unit time regardless of remaining drug |
| Plasma curve shape | Gradually declining after peak - still flatter than IR | Flat plateau - near-constant concentration |
| Peak-trough fluctuation | Reduced compared to IR, but still some variation | Minimal - tightest control within therapeutic window |
| Predictability | Less mathematically precise | Highly precise and programmable |
| Sophistication | Simpler technology | More complex engineering required |
Understanding the Kinetics - The Critical Difference
- Rate of release is proportional to the amount of drug remaining
- As the tablet depletes, release rate slows down
- Plasma levels rise then gradually fall
- Think: "The more drug left, the faster it comes out"
- Rate of release is constant regardless of drug remaining
- A fixed amount (e.g., 10 mg/hour) is released every hour
- Plasma levels stay essentially flat for the entire dosing interval
- Think: "IV infusion in an oral tablet"
Plasma
Conc.
| IR
| /\
| / \ SR CR
| / \ /\__________ ___________
| / \ / \ / \
|____/________\_/ \_____________\__
Time
Mechanism Differences
| Mechanism | Used In |
|---|---|
| Matrix erosion / slow dissolution | SR (simpler) |
| Hydrophilic polymer matrix (HPMC) | SR |
| Rate-controlling membrane (reservoir) | CR |
| Osmotic pump (OROS) | CR - near perfect zero-order delivery |
| Ion-exchange resin | CR |
| Semi-permeable membrane with laser-drilled orifice | CR (e.g., Procardia XL, Glucotrol XL) |
Clinical Examples
| Drug | Type | Why |
|---|---|---|
| Metoprolol succinate (Toprol XL) | CR/ER | Osmotic-type, near zero-order delivery |
| Nifedipine GITS/OROS (Adalat LA) | CR | OROS technology - true zero-order |
| Diltiazem CD/SR | SR | Matrix-based, first-order |
| Morphine sulfate (MS Contin) | SR | Matrix tablet, first-order |
| Oxybutynin OROS (Ditropan XL) | CR | OROS - reduces anticholinergic side effects vs SR |
| Metformin XR | SR | Matrix erosion |
Key Comparison Table
| Parameter | SR | CR |
|---|---|---|
| Kinetics | First-order | Zero-order |
| Rate of release | Decreases over time | Constant |
| Plasma level | Gradual decline | Flat plateau |
| Therapeutic window control | Moderate | Tight |
| Technology | Simpler (matrix) | Complex (OROS, membranes) |
| Cost | Lower | Higher |
| Best for drugs with | Moderate half-life | Narrow therapeutic index |
Practical Bottom Line
- SR = "slow down the release" - good enough for most chronic drugs
- CR = "control the release precisely" - needed when you absolutely must keep plasma levels within a narrow therapeutic window (e.g., drugs where toxicity appears just above the therapeutic range)
- In practice, manufacturers use SR and CR interchangeably on labels - but when they are truly different, CR is the superior, more engineered system
- Both are subcategories under the broader umbrella of extended/modified release
Can you tell the difference in release kinetics between extended and sustained release
Release Kinetics: Extended Release (ER) vs Sustained Release (SR)
The Kinetic Profiles
| Parameter | Extended Release (ER) | Sustained Release (SR) |
|---|---|---|
| Primary kinetics | Mixed / first-order dominant | First-order (more defined) |
| Release rate | Slows progressively over time | Slow but more uniform rate than ER |
| Plasma Cmax | Lower than IR, but may still have a modest peak | Flatter - aimed at maintaining therapeutic window |
| Plasma curve shape | Gradual rise then gradual fall - elongated IR curve | Rise to a plateau, then slower decline |
| Goal | Extend the dosing interval | Maintain steady therapeutic concentration |
| Peak-trough fluctuation | Reduced vs IR but not minimized | Further reduced - closer to steady state |
Visualizing the Difference
Plasma
Conc.
|
| IR: sharp spike
| /\
| / \
| / \ ER: elongated curve SR: flatter plateau
|/ \ / \ /‾‾‾‾‾‾‾‾‾\
| \_/ \__ / \___
|___________________________________________ Time →
- ER flattens and stretches the IR curve - still rises and falls, just more slowly
- SR achieves a more plateau-like profile - the flat portion is the defining feature
Why ER Does Not Have a Fixed Kinetic Order
- First-order matrix erosion
- Zero-order osmotic pump
- Biphasic release (initial IR burst + slow ER phase)
SR Has a More Defined Kinetic Intent
- First-order kinetics in most matrix-based SR formulations
- Release rate that is proportional to drug remaining in the dosage form
- The goal is not just "longer duration" but "maintained therapeutic levels"
- Rate equation: dC/dt = -k·C (rate decreases as concentration in tablet falls)
The Honest Summary
| Question | Answer |
|---|---|
| Do ER and SR have distinctly different kinetics? | In theory yes, in practice often no |
| What kinetics does ER follow? | Any - it is a label term, not a kinetic definition |
| What kinetics does SR follow? | First-order (primarily), occasionally approaching zero-order |
| Which is more precisely defined? | SR has more pharmacokinetic intent; CR is the most precisely defined |
| Are they used interchangeably? | Yes, constantly - metoprolol succinate is called XL, SR, ER, and CR by different manufacturers/countries |
Where the Real Kinetic Distinction Lives
First-order release (SR) → rate decreases as drug depletes
Zero-order release (CR) → rate stays constant regardless of drug remaining
Can you give the conc time graph of extended sustained controlled and immediate release
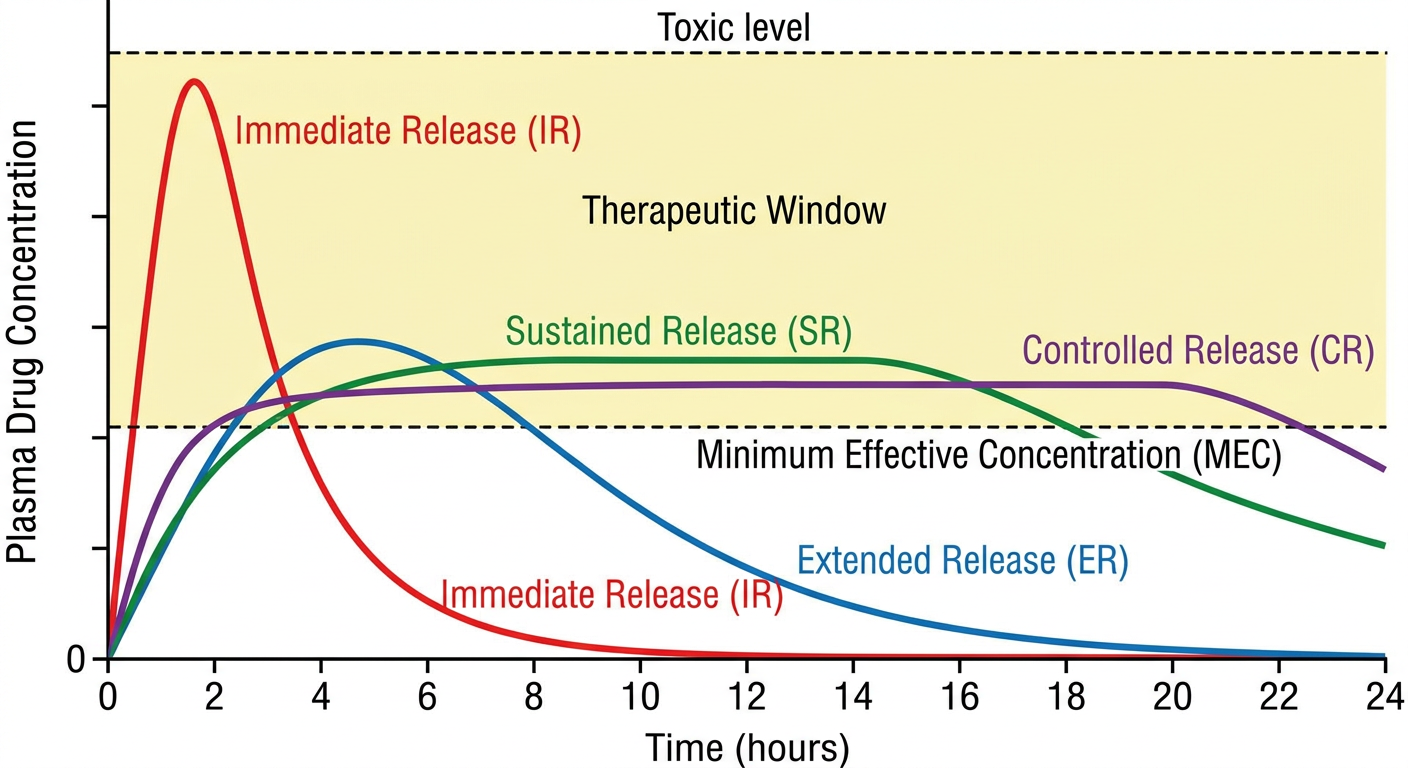
A clean pharmacokinetics concentration-time graph showing 4 drug release profiles on the same axes. X-axis labeled "Time (hours)" from 0 to 24. Y-axis labeled "Plasma Drug Concentration". Two horizontal dashed lines: one labeled "Toxic level" near the top and one labeled "Minimum Effective Concentration (MEC)" in the middle. Four curves: 1) "Immediate Release (IR)" - a sharp tall spike that peaks around 1-2 hours then drops rapidly below MEC by hour 6, colored red. 2) "Extended Release (ER)" - a broad low curve that rises slowly, peaks moderately around hour 4-6, then gradually declines, staying above MEC until about hour 12-14, colored blue. 3) "Sustained Release (SR)" - a curve that rises to a modest plateau, stays relatively flat and within the therapeutic window from about hour 2 to hour 14, then slowly declines, colored green. 4) "Controlled Release (CR)" - the flattest curve of all, nearly a perfect horizontal line within the therapeutic window from hour 1 to hour 20, then gently declining, colored purple. All four curves start at zero. The area between the two dashed lines is shaded light yellow and labeled "Therapeutic Window". Clean white background, clear labels on each curve, professional medical textbook style diagram.
Reading the Graph
| Formulation | Peak (Cmax) | Time above MEC | Plateau? | Kinetics |
|---|---|---|---|---|
| IR (red) | Highest - may breach toxic level | Shortest (~4-6 hrs) | No - sharp spike and drop | Rapid absorption, first-order elimination |
| ER (blue) | Moderate | Medium (~12-14 hrs) | No - broad curve, still rises and falls | Mixed/first-order, prolonged absorption |
| SR (green) | Lower, flatter | Longer (~14-16 hrs) | Partial - modest plateau phase | First-order, release rate proportional to drug remaining |
| CR (purple) | Lowest Cmax, flattest | Longest (~18-20 hrs) | Yes - near-perfect flat line | Approaches zero-order - constant rate regardless of drug remaining |
Key Takeaways from the Graph
- IR - highest peak, shortest duration, most likely to breach toxic threshold and drop below MEC between doses
- ER - smooths the curve out, reduces Cmax, extends the dosing interval - but still has a visible peak and trough
- SR - further flattening with a more defined plateau, better suited for drugs needing steady levels
- CR - the gold standard, mimics a continuous IV infusion in oral form - stays within the therapeutic window the longest with minimal fluctuation