Why Omeprazole given empty stomach in morning hours
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have excellent, authoritative textbook content. Here is the complete explanation:
Why Omeprazole Is Given on an Empty Stomach in the Morning
1. Mechanism - It Only Blocks ACTIVE Proton Pumps
Omeprazole is a prodrug and a weak base (pKa ~4). After intestinal absorption, it diffuses into the highly acidic secretory canaliculus of the gastric parietal cell, where it:
- Gets protonated and concentrated >1000-fold (Henderson-Hasselbalch trapping)
- Converts into its active sulfenamide cation form
- Forms an irreversible covalent disulfide bond with the H+/K+-ATPase (proton pump)
The critical point: Omeprazole can only bind and block pumps that are actively secreting acid at the time the drug is present in the bloodstream. Pumps sitting in quiescent tubulovesicles (not yet moved to the canalicular surface) are completely protected from inhibition.
- Katzung's Basic and Clinical Pharmacology, 16th Ed. - this mechanism of Henderson-Hasselbalch trapping and covalent binding
2. Why Empty Stomach (Fasting State)?
Food is the strongest activator of proton pumps. Taking omeprazole 30-60 minutes before a meal ensures:
| State | % of Pumps Actively Secreting |
|---|---|
| Fasting | ~10% |
| After a meal (peak stimulation) | ~70-80% |
- In a fasting state, only ~10% of pumps are active - that is too few to inhibit.
- By taking omeprazole before the first meal of the day, peak serum drug concentration (Tmax ~1-3 hours for omeprazole) coincides with the maximum meal-stimulated pump activation.
- This maximizes the number of pumps the drug can bind and irreversibly block.
Food also reduces omeprazole's bioavailability by ~50% if taken with or after food, further reducing drug levels available to act.
- Katzung's Basic and Clinical Pharmacology, 16th Ed. - "the drugs should be administered on an empty stomach... PPIs should be administered 30 to 60 minutes before breakfast, so that the peak serum concentration coincides with the maximal activity of proton-pump secretion"
3. Why Morning Specifically?
- Breakfast activates the most pumps during the day - it is the largest acid-secretory stimulus after an overnight fast.
- The parietal cell has a circadian rhythm - pump density at the canalicular surface is highest in the morning after the nocturnal fasting period.
- Omeprazole has a short serum half-life (~0.5-1 hour) but produces acid suppression lasting up to 24 hours because the pump is irreversibly destroyed. New pumps take at least 18 hours to be synthesized.
- Once-daily morning dosing therefore covers the entire 24-hour cycle.
Studies show that taking a PPI before dinner instead of before breakfast results in significantly worse nighttime and 24-hour acid control, because fewer pumps are being stimulated at dinnertime compared to the morning post-fast period.
4. The 3-4 Day Lag to Full Effect
Because not all pumps are inhibited on day 1 (those in vesicles are spared), full acid suppression builds gradually:
- Day 1: ~66% inhibition
- Day 3-4: 90-98% inhibition (steady state)
Conversely, after stopping omeprazole, full acid secretion takes 3-4 days to return (as new pumps are synthesized).
- Mulholland and Greenfield's Surgery, 7th Ed. and Katzung's Basic and Clinical Pharmacology, 16th Ed.
Summary
| Reason | Explanation |
|---|---|
| Empty stomach | Food reduces bioavailability by ~50% |
| 30-60 min before breakfast | Peak drug level timed to maximal pump activation by food |
| Morning hours | Breakfast causes maximum pump recruitment after overnight fast |
| Irreversible binding | Only active, canaliculus-surface pumps can be inhibited |
| Once daily sufficient | Pump destruction lasts 18+ hours until new pumps are synthesized |
Special drug delivery systems including transdermal drug delivery system
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
special drug delivery systems types liposome nanoparticle osmotic controlled release implant overview pharmacology
Loading Image
Loading Image
Special Drug Delivery Systems (SDDS)
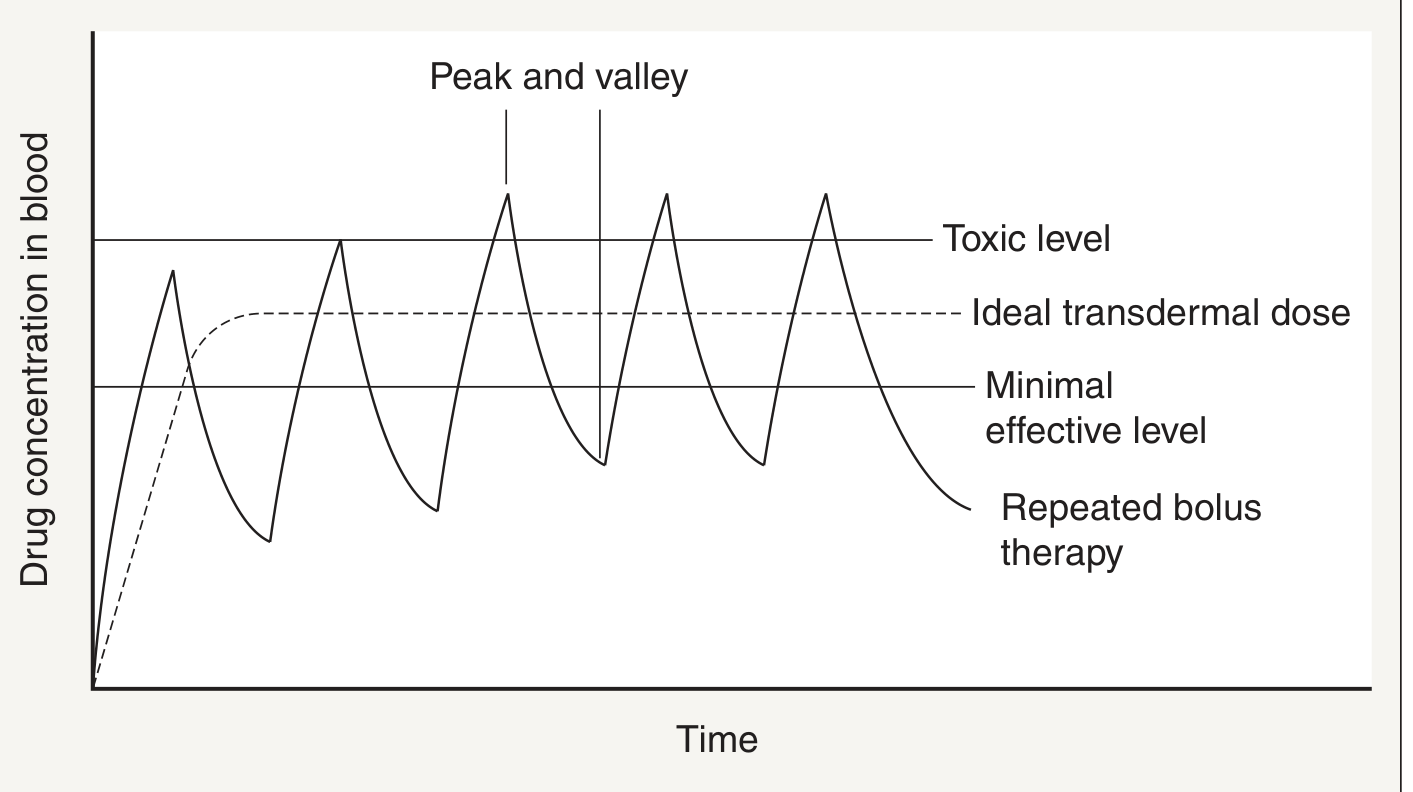
Special (novel/advanced) drug delivery systems are formulations designed to deliver drugs at a controlled rate, to a specific site, and for a desired duration - overcoming limitations of conventional dosage forms (tablets, injections) which cause erratic "peak and valley" drug levels.
Why Special DDS Are Needed
Conventional repeated bolus dosing causes oscillating drug concentrations that repeatedly cross the toxic ceiling and fall below the minimum effective level. Special DDS maintain a flat, ideal therapeutic concentration:
Classification of Special DDS
1. Controlled Release Oral Systems
These modify the rate and site of drug release from oral formulations.
| Type | Mechanism | Examples |
|---|---|---|
| Enteric-coated | Dissolves only at intestinal pH (>6) | Omeprazole, diclofenac |
| Matrix tablets | Drug embedded in polymer; release by diffusion | Metformin XR |
| Reservoir systems | Drug core surrounded by rate-controlling membrane | Nifedipine GITS |
| Osmotic pump (OROS) | Osmotic pressure drives drug out through laser-drilled orifice at constant rate | Methylphenidate (Concerta), Nifedipine (Procardia XL), Glipizide |
| Ion exchange resins | Drug bound to resin; released by ion exchange in GI tract | Dextromethorphan (Delsym) |
Osmotic Pump (OROS) is particularly elegant: a semipermeable membrane surrounds an osmotic core. Water enters by osmosis, expands the core, and pushes drug out at a zero-order (constant) rate independent of GI motility or pH.
2. Transdermal Drug Delivery Systems (TDDS)
The most detailed and clinically important of the special DDS.
What is TDDS?
Drug delivery across the skin into systemic circulation. The skin acts both as the route and the reservoir.
Advantages
-
Bypasses hepatic first-pass metabolism
-
Avoids GI degradation and side effects
-
Continuous, steady-state drug release - no peaks or valleys
-
Improved patient compliance (weekly/biweekly patches)
-
Easily terminated - just remove the patch
-
Reduced total dose needed (increased efficiency)
-
Avoids painful injections
-
Dermatology 2-Volume Set 5e
Ideal Drug Characteristics for TDDS
| Property | Requirement |
|---|---|
| Molecular weight | < 400 Da |
| Lipophilicity | Moderate (octanol-water partition coefficient up to 10,000) |
| Daily dose | < 10 mg/day |
| Skin permeability | Adequate intrinsic permeability |
Drugs Available as Transdermal Patches
Buprenorphine, capsaicin, clonidine, estradiol, ethinyl estradiol, fentanyl, glyceryl trinitrate (nitroglycerin), nicotine, scopolamine, rivastigmine, rotigotine, selegiline, testosterone, lidocaine, methylphenidate, oxybutynin, sumatriptan
Pathways of Drug Entry into Skin
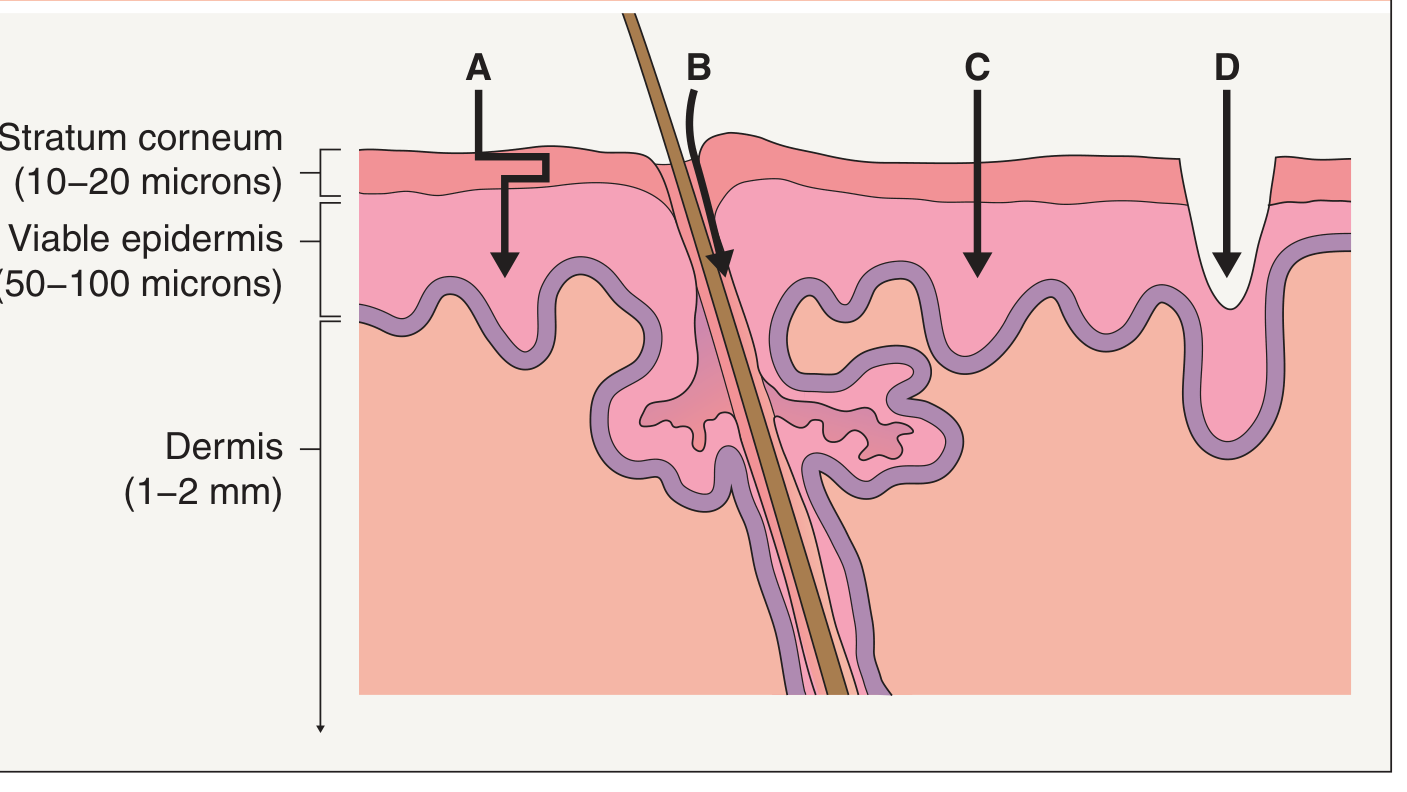
- A - Transcellular / Intercellular (tortuous lipid) pathway: Main route during passive and chemically enhanced delivery. Drug traverses through the lipid bilayers of the stratum corneum extracellular matrix.
- B - Follicular route (shunt pathway): Via hair follicles and sweat ducts. Enhanced by iontophoresis and particulate formulations.
- C - Electroporation: High-voltage pulses create pores through stratum corneum for macromolecule delivery.
- D - Mechanical disruption routes: Microneedles, ablation, abrasion, fractional photothermolysis - create micron-scale channels bypassing the stratum corneum entirely.
Strategies to Enhance Transdermal Delivery
The stratum corneum (SC) is the major barrier. Enhancement strategies are divided into chemical and physical:
Chemical Enhancers
| Agent | Mechanism |
|---|---|
| Water (occlusion) | Hydrates SC; swells corneocytes, distends intercellular spaces, creates "pores" - most common |
| Solvents (ethanol, DMSO) | Extract SC lipids, disrupt lamellar bilayers |
| Surfactants (SLS, propylene glycol) | Extract lipids, expand lacunar domains |
| Azone, fatty acids, urea | Alter SC lipid phase behavior |
| Ionic liquids | Drug paired with counterion in liquid form - avoids need for solvent |
| Peptides (polyarginine) | Penetrate/disrupt SC lipids |
| Liposomes/nanoparticles | Increase drug solubility and skin partitioning; some allow slow release |
Note: Liposomes typically do NOT penetrate intact SC as whole vesicles - they enhance delivery by increasing effective drug concentration at the skin surface and facilitating partitioning.
Physical Enhancers
| Method | How it Works | Examples |
|---|---|---|
| Iontophoresis | Low current from external electrode drives charged drug molecules across SC by electrophoresis | Fentanyl, lidocaine, pilocarpine, glucose monitoring (reverse iontophoresis) |
| Electroporation | Short, high-voltage pulses (~100V, microsecond-millisecond) create lipid pores in SC | Chemotherapy into skin tumors |
| Ultrasound (cavitational) | Low-frequency (<1 MHz) creates bubble cavitation - microscopic SC defects | Pre-treatment before lidocaine patches |
| Ultrasound (thermal) | Heats deep tissue, increases permeability | Anti-inflammatory delivery during physiotherapy |
| Microneedles | 0.2-1 mm needles (solid, hollow, or dissolving) punch micropores in SC | Naltrexone, zolmitriptan, insulin, influenza vaccines |
| Thermal ablation | Microsecond heat pulses create micropores; minimal deep-tissue damage | Macromolecule delivery |
| Tape stripping / Abrasion | Mechanical removal of SC layers | Research; pre-treatment |
| Fractional photothermolysis | Laser-created micron holes | 5-FU, ALA, lidocaine delivery |
| STAR particles | Millimeter particles with protruding microneedles; rubbed on skin over large areas | Broad-area macromolecule delivery |
- Dermatology 2-Volume Set 5e
3. Liposomes
Phospholipid bilayer vesicles that can encapsulate both water-soluble (in aqueous core) and fat-soluble (in membrane) drugs.
- Passive targeting: Accumulate in tumors via Enhanced Permeability and Retention (EPR) effect
- Active targeting: Surface-conjugated antibodies or ligands direct to specific cell receptors
- PEGylation: Coating with polyethylene glycol prolongs circulation half-life ("stealth liposomes")
- Examples: Doxil (doxorubicin-liposome for cancer), Marqibo (vincristine-liposome for ALL), DepoDur (morphine epidural)
4. Nanoparticles
Particles 1-1000 nm used as drug carriers.
| Type | Material | Use |
|---|---|---|
| Polymeric nanoparticles | PLGA, PLA | Sustained release, cancer |
| Solid lipid nanoparticles | Lipid matrix | Topical, oral, parenteral |
| Dendrimers | Branched polymers | Gene delivery, cancer |
| Mesoporous silica | Silica framework | pH-triggered release |
5. Implantable Drug Delivery Systems
Devices surgically inserted for long-term, continuous drug release.
- Non-degradable: Silastic rods - levonorgestrel (Norplant, Jadelle)
- Biodegradable: PLGA matrices that erode over time - no removal needed
- Osmotic implants: Viadur (leuprolide acetate pump for prostate cancer)
- Release mechanisms: diffusion, osmotic pressure, biodegradation
Ideal properties: Biocompatible, sterile, stable, retrievable, rate-controlled release
6. Mucoadhesive / Mucosal Drug Delivery
- Buccal/sublingual: Bypasses first-pass (e.g., buprenorphine, fentanyl lozenges)
- Nasal: Rapid systemic absorption (e.g., desmopressin, sumatriptan nasal spray)
- Rectal: Useful when oral route unavailable
- Vaginal rings: Continuous hormonal delivery (e.g., NuvaRing)
7. Targeted / Antibody-Drug Conjugates (ADC)
Monoclonal antibody linked to a cytotoxic drug. The antibody delivers the drug specifically to cancer cells expressing target antigens, minimizing systemic toxicity. Examples: Trastuzumab emtansine (Kadcyla) for HER2+ breast cancer.
Summary Table
| System | Route | Mechanism | Key Examples |
|---|---|---|---|
| Osmotic pump (OROS) | Oral | Zero-order osmotic release | Concerta, Procardia XL |
| Transdermal patch | Skin | Passive/enhanced diffusion | Fentanyl, NTG, nicotine |
| Liposomes | IV/topical | Vesicle encapsulation | Doxil, Marqibo |
| Nanoparticles | IV/oral | Polymer/lipid matrix | PLGA drug conjugates |
| Implants | Subcutaneous | Diffusion/osmosis | Norplant, Viadur |
| Mucoadhesive | Mucosal | Adhesion + diffusion | Buccal buprenorphine |
| ADC | IV | Antibody targeting | Kadcyla |
This is a shared conversation. Sign in to Orris to start your own chat.