Chondrolysis ms ortho 20 marks answer
Reading File
Finding Sources
Finding Sources
Searching PubMed
chondrolysis hip joint pathogenesis treatment
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have comprehensive information from the textbooks. Let me compile the full 20-mark MS Ortho answer.
CHONDROLYSIS - MS Orthopaedics 20-Mark Answer
DEFINITION
Chondrolysis is the rapid, progressive dissolution (necrosis) of articular hyaline cartilage affecting both the femoral head and the acetabulum, leading to concentric narrowing of the hip joint space. It is a distinct pathological process and must be differentiated from avascular necrosis (AVN) of the femoral head.
HISTORICAL BACKGROUND
- First described by Waldenstrom (1930) as "acute juvenile arthritis of the hip"
- The term "chondrolysis" was coined by Jones (1971)
- Most classic association is with Slipped Capital Femoral Epiphysis (SCFE)
TYPES / CLASSIFICATION
1. Idiopathic (Primary) Chondrolysis
- No identifiable underlying cause
- Predominantly affects adolescent girls (10-16 years)
- Common in patients of African descent
- Can be bilateral in some cases
2. Secondary (Symptomatic) Chondrolysis
Associated with:
| Cause | Example |
|---|---|
| SCFE (most common) | Post-fixation pin penetration |
| Immobilization | Prolonged hip spica casting |
| Infection | Septic arthritis |
| Trauma | Traumatic subluxation of hip |
| Iatrogenic | Intra-articular leak of bone cement |
| Inflammatory | Psoriatic arthritis |
| Tumors | Hip tumors |
| Shoulder | Post-arthroscopy with continuous anesthetic infusion |
| Genetic | Stickler syndrome |
EPIDEMIOLOGY
- Age: Predominantly adolescents (12-17 years)
- Sex: Female >> Male (especially idiopathic form)
- Race: Higher incidence in Black/African descent individuals
- SCFE-related: Incidence has decreased from ~7% to ~1% as surgical techniques have improved
PATHOGENESIS
The exact mechanism remains debated. Several theories exist:
1. Mechanical Theory
- Persistent pin/screw penetration into the joint is the most frequently cited cause (in SCFE)
- Mechanical damage to chondrocytes and disruption of cartilage matrix
2. Immune / Inflammatory Theory
- Proposed synovitis with release of proteolytic enzymes (matrix metalloproteinases) causing cartilage degradation
- Pannus-like tissue eroding cartilage from the synovial side
- Some authors suggest an autoimmune component - an immune response triggered by slip or damaged cartilage
3. Ischemia Theory
- Vascular compromise to subchondral bone leading to cartilage necrosis
4. Nutritional Deprivation
- Prolonged immobilization restricts synovial fluid circulation, starving chondrocytes of nutrients
5. Post-Shoulder Arthroscopy (for shoulder chondrolysis)
- Associated with:
- Continuous post-operative intra-articular anaesthetic infusion (e.g., bupivacaine with epinephrine - most strongly implicated)
- Use of radiofrequency energy
- Bioabsorbable suture anchors
- Intra-articular contrast medium
- Low-grade infection
PATHOLOGY
Macroscopic
- Early: Synovial hyperemia, joint effusion
- Late: Complete cartilage loss, "bone-on-bone" appearance, fibrous ankylosis
Microscopic
- Superficial zone: Loss of chondrocytes, fibrillation of matrix
- Deep zone: Chondrocyte death (empty lacunae)
- Synovial proliferation with chronic inflammatory infiltrate (lymphocytes, plasma cells)
- Pannus formation eroding cartilage
- Subchondral bone thickening (eburnation) in advanced stages
CLINICAL FEATURES
Symptoms
- Pain in the hip (groin, thigh, or knee referred pain) - often severe
- Stiffness - particularly morning stiffness
- Limp (antalgic gait)
- Decreased range of motion - especially flexion, abduction, internal rotation
- Abnormal gait pattern
Signs
- Loss of hip motion (diagnostic criterion requires decreased ROM)
- Fixed flexion deformity may develop
- Muscle atrophy of the thigh
- In advanced cases: fibrous ankylosis
DIAGNOSIS
Diagnostic Criteria
- Joint space < 3 mm on plain radiograph (normal: 4-6 mm; some texts use 3.5-7 mm)
- Decreased range of motion of the hip joint
Both criteria must be present for diagnosis (Campbell's Operative Orthopaedics, 15th Ed, 2026).
Investigations
Plain Radiograph (AP + Lateral Hip)
- Concentric joint space narrowing (hallmark) - affects entire joint space uniformly
- Periarticular osteoporosis
- Joint space < 3 mm (diagnostic)
- Later: Osteophyte formation
- Protrusio acetabuli may develop
- Premature fusion of greater trochanteric epiphysis
- Maximal narrowing typically develops within the first year
MRI
- Early detection before radiographic changes
- Shows cartilage thinning, synovitis, joint effusion
- Subchondral bone marrow changes
Technetium-99m Bone Scan
- Marked periarticular uptake (hot scan)
- Premature fusion of the greater trochanteric epiphysis
- Findings may precede changes on MRI and plain radiographs - useful for early diagnosis
Ultrasound
- Joint effusion
Synovial Fluid Analysis
- Inflammatory pattern (elevated WBC)
- Helps exclude septic arthritis
DIFFERENTIAL DIAGNOSIS
| Condition | Differentiating Features |
|---|---|
| AVN (femoral head) | Sclerosis + subchondral collapse on one side; preserved joint space early |
| Septic arthritis | Acute onset, fever, elevated ESR/CRP, purulent fluid |
| Transient synovitis | Self-limiting, normal/minimal joint space change |
| Tuberculous arthritis | Chronic, systemic symptoms, erosive pattern, night sweats |
| Juvenile idiopathic arthritis (JIA) | Systemic features, multiple joints, RF/ANA |
| Legg-Calve-Perthes disease | Femoral head fragmentation, younger children |
TREATMENT
Conservative Management
The following have NOT been shown to modify the course of chondrolysis:
- Bed rest
- Traction
- Salicylates / NSAIDs
- Corticosteroids (systemic)
- Physical therapy alone
Active Management
1. Intra-articular Corticosteroid Injection
- Some success reported (Campbell's Operative Orthopaedics)
- Reduces intra-articular inflammation
2. Operative Manipulation + Physical Therapy
- Manipulation under anaesthesia to restore range of motion
- Followed by vigorous physiotherapy program
- Campbell's reports "some success" with this combination
3. Remove Causative Factor
- Remove any penetrating pins/screws immediately (in SCFE-related cases)
- Cease intra-articular anaesthetic infusions (shoulder)
4. Physiotherapy
- Passive and active ROM exercises
- Hydrotherapy
- Gait training
5. Surgical Options (for advanced disease)
| Procedure | Indication |
|---|---|
| Arthodesis (Hip fusion) | Young patient, unilateral, severe joint destruction |
| Total Hip Arthroplasty (THA) | Skeletally mature, bilateral, failed conservative Rx |
| Shoulder arthroscopy | Shoulder chondrolysis - improves pain and ROM but increases reoperation rate (~25%) |
| Intertrochanteric osteotomy | Some role in preventing progression in SCFE-related cases |
PROGNOSIS
- Generally poor, especially idiopathic form
- Many patients eventually require hip replacement (Rheumatology, 2-Volume Set, Elsevier 2022)
- Spontaneous partial cartilage recovery has been reported (unusual)
- Fibrous ankylosis of the hip is a common end-stage outcome
- After chondrolysis develops in SCFE patients, ~45% will ultimately require arthroplasty
- Joint space and motion may slightly improve during the first few years, but then progression occurs with osteophyte formation and protrusio acetabuli
COMPLICATIONS
- Fibrous ankylosis
- Secondary osteoarthritis
- Protrusio acetabuli
- Limb length discrepancy
- Premature physeal fusion
- Avascular necrosis (may coexist, especially in SCFE)
CHONDROLYSIS AT SHOULDER (Special Mention)
- Occurs post-shoulder arthroscopy, typically with continuous post-operative intra-articular anesthetic infusion
- Complete dissolution of articular cartilage of humeral head and glenoid
- Manifests as worsening pain and gradual reduction in ROM
- Arthroscopic treatment improves pain and ROM but carries ~25% reoperation rate
- (Miller's Review of Orthopaedics, 9th Ed)
IMPORTANT POINTS FOR EXAM
| Key Fact | Value |
|---|---|
| Diagnostic joint space width | < 3 mm |
| Normal hip joint space | 4-6 mm |
| Most common cause | Pin penetration in SCFE |
| Most common victim (idiopathic) | Adolescent girls |
| Peak narrowing timing | Within first year |
| Bone scan finding | Marked periarticular uptake + premature GT fusion |
| Modality to detect early | Technetium bone scan (precedes MRI changes) |
| Prognosis | Poor - often requires THA |
RADIOLOGICAL SERIES (Campbell's, Fig. 38.124)
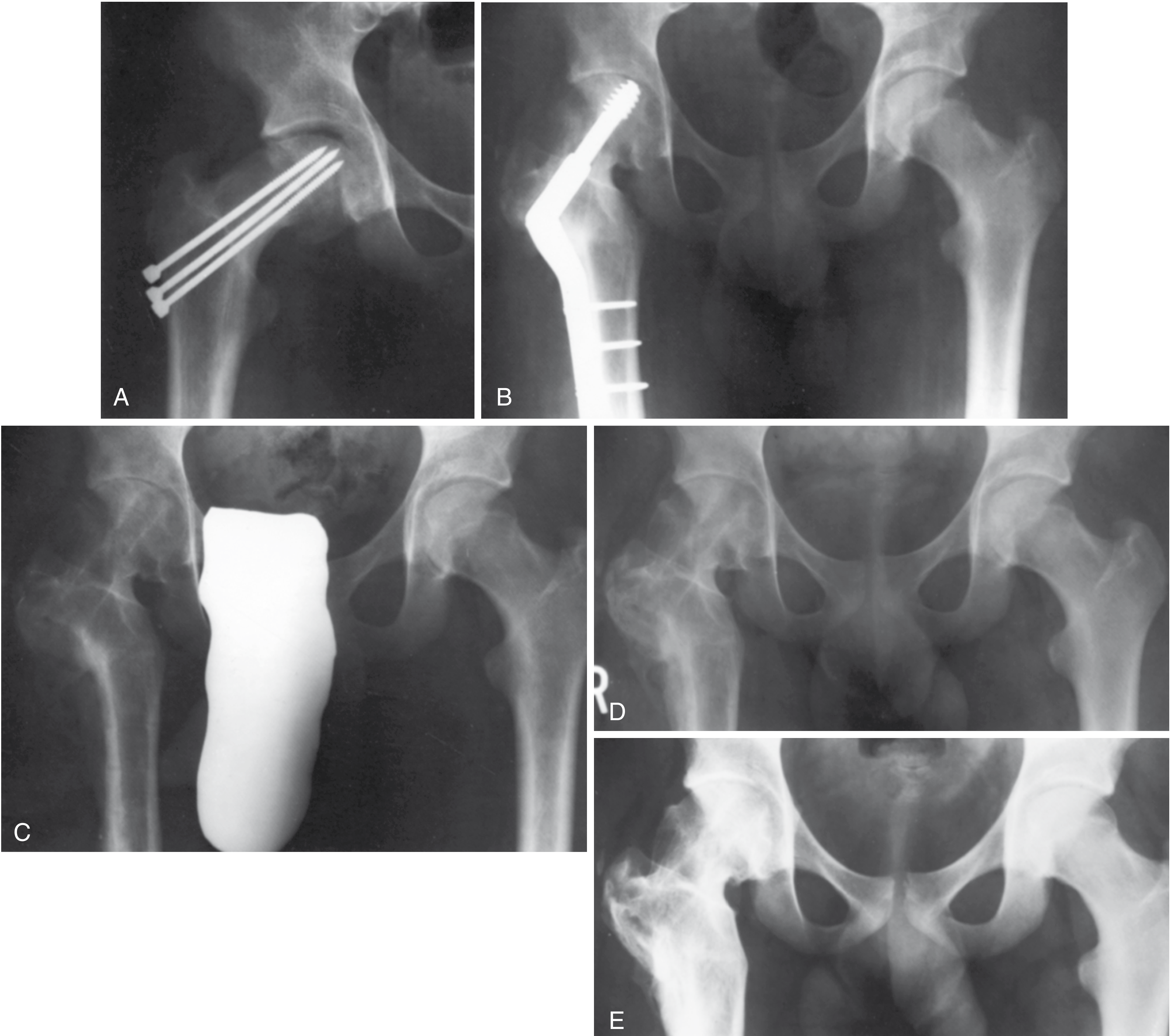
Fig. 38.124 - Chondrolysis 24 months after flexion internal rotation osteotomy for severe SCFE. Note progressive joint space loss (A), fixation with cannulated screw (B), and eventual total hip arthroplasty (C-E). - Campbell's Operative Orthopaedics, 15th Ed, 2026
Sources:
- Campbell's Operative Orthopaedics, 15th Ed 2026, Section: CHONDROLYSIS, p.1844
- Rheumatology, 2-Volume Set, Elsevier 2022, Section: IDIOPATHIC CHONDROLYSIS
- Miller's Review of Orthopaedics, 9th Ed, Chapter: Chondrolysis (shoulder)
- Rosen's Emergency Medicine - SCFE complications
This is a shared conversation. Sign in to Orris to start your own chat.