****a) Define MALNUTRITION. & classify PEM b) Describe CAUSES & CLINICAL FEATURES of severe form of Malnutrition c) Explain PREVENTIVE measures to reduce PEM in India. d) Discuss in detail the prevention & social measures against malnutrition at family & community level
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I now have all the content needed to write a comprehensive answer. Let me compile the full structured response.
Malnutrition & Protein-Energy Malnutrition (PEM) - Complete Notes
a) Definition of Malnutrition & Classification of PEM
Definition of Malnutrition
Malnutrition is a pathological state resulting from a relative or absolute deficiency or excess of one or more essential nutrients. It encompasses both undernutrition (deficiency of calories, protein, vitamins, or minerals) and overnutrition (excess caloric intake leading to obesity).
In primary malnutrition, one or all dietary components are missing from the diet. In secondary (conditional) malnutrition, dietary intake is adequate but malnutrition results from nutrient malabsorption, impaired use or storage, excess losses, or increased metabolic requirements - as seen in gastrointestinal diseases, chronic wasting diseases, and acute critical illness.
- Robbins & Kumar Basic Pathology, p. 289
Classification of PEM
Protein-Energy Malnutrition (PEM) - now termed Severe Acute Malnutrition (SAM) by the WHO - is defined as a state where weight-to-height ratio is 3 standard deviations below the median growth standard, with visible wasting, or the presence of nutritional edema.
WHO/Wellcome Classification
| Grade | % of Expected Weight-for-Age | Edema |
|---|---|---|
| Normal | >80% | No |
| Underweight (mild PEM) | 80-60% | No |
| Kwashiorkor | 60-80% | Yes |
| Marasmus | <60% | No |
| Marasmic-Kwashiorkor | <60% | Yes |
IAP (Indian Academy of Pediatrics) Classification
Based on percentage of expected weight-for-age (median):
| Grade | % of Expected Weight |
|---|---|
| Normal | >80% |
| Grade I (Mild PEM) | 71-80% |
| Grade II (Moderate PEM) | 61-70% |
| Grade III (Severe PEM) | 51-60% |
| Grade IV (Very Severe PEM) | <50% |
WHO Anthropometric Classification (Z-score based)
Three nutritional indices are used:
- Underweight - weight-for-age Z-score < -2SD (composite measure)
- Stunting - height-for-age Z-score < -2SD (chronic/past malnutrition)
- Wasting - weight-for-height Z-score < -2SD (acute/current malnutrition)
Severe forms are defined at < -3SD below the median.
- Park's Textbook of Preventive and Social Medicine, p. 736
b) Causes & Clinical Features of Severe Forms of Malnutrition
The two severe ends of the PEM spectrum are Marasmus and Kwashiorkor.
MARASMUS

Cause: Severe deficiency of both calories and protein. An inadequate total caloric intake forces the body to catabolize somatic protein (skeletal muscle) and mobilize subcutaneous fat as fuel sources.
Pathophysiology: The somatic protein compartment (skeletal muscle) is severely depleted. The visceral compartment is relatively spared, so serum albumin remains near normal. Low leptin stimulates the hypothalamic-pituitary-adrenal axis, producing high cortisol that drives lipolysis.
Clinical Features of Marasmus:
- Severe generalized wasting of muscle and subcutaneous fat
- Body weight typically <60% of expected for age
- No edema - distinguishes from kwashiorkor
- Extremities emaciated; head appears disproportionately large ("old man's face" / "monkey facies")
- Skin loose, wrinkled - "baggy pants" appearance
- Serum albumin normal or only slightly reduced
- Anemia and multi-vitamin deficiency features
- Immune deficiency (especially T-cell mediated) - concurrent infections common
- Growth retardation, mental apathy, irritability
- Arm circumference < 12.5 cm indicates severe malnutrition
KWASHIORKOR
Cause: Predominantly protein deficiency with relatively adequate caloric intake. Classically occurs in children weaned early and fed predominantly a carbohydrate diet. The name comes from the Ga language in Ghana - "the illness of the displaced child."
Pathophysiology: The visceral protein compartment (liver and other organs) is severely depleted. Hypoalbuminemia results in generalized/dependent edema. Reduced synthesis of the lipoprotein carrier protein causes fat accumulation in the liver (fatty liver/steatosis).
Clinical Features of Kwashiorkor:
| System | Features |
|---|---|
| General | Body weight 60-80% of expected; weight loss masked by edema |
| Edema | Generalized/pitting edema - hallmark feature; face (moon face), abdomen (ascites), limbs |
| Skin | "Flaky paint" or "crazy-pavement" dermatosis - alternating zones of hyperpigmentation, desquamation, and hypopigmentation |
| Hair | "Flag sign" - alternating bands of pale (depigmented) and darker color; fine texture; easy pluckability; loss of firm attachment |
| Liver | Enlarged fatty liver (hepatomegaly with steatosis) |
| GI | Anorexia, vomiting, diarrhea, distended abdomen |
| Neurological | Apathy, listlessness, irritability; psychomotor changes |
| Immunity | Severe immune deficiency; secondary infections common |
| Lab | Hypoalbuminemia, hypoproteinemia |
| Muscles | Relative sparing of muscle mass (may be masked by edema) |
MARASMIC-KWASHIORKOR
A mixed form with features of both - severe wasting (<60% expected weight) plus edema. Has the worst prognosis.
Common Causes of PEM (General)
- Poverty - inadequate food availability; most common root cause in India
- Ignorance - lack of knowledge about infant feeding, weaning practices, nutritional needs
- Faulty feeding practices - early weaning, delayed introduction of complementary foods, inadequate breastfeeding
- Infections - diarrhea, measles, respiratory infections (create a malnutrition-infection cycle)
- Large family size - food shared among many children
- Birth spacing - closely spaced pregnancies, displacement of older child from breast
- Low birth weight - starts life already malnourished
- Maternal malnutrition - inadequate nutrition during pregnancy
- Food taboos and cultural beliefs - restriction of certain foods for children
- Secondary causes - chronic diarrhea, protein-losing enteropathies, nephrotic syndrome, burns, malabsorption
- Robbins & Kumar Basic Pathology, p. 289-291; Park's Textbook of Preventive and Social Medicine, p. 736-737
c) Preventive Measures to Reduce PEM in India
Based on the 8th FAO/WHO Expert Committee on Nutrition and adapted for the Indian context, prevention operates at four levels:
(a) Health Promotion
- Measures for pregnant and lactating women - nutritional education, iron-folate supplementation, distribution of protein-caloric supplements through the ICDS (Integrated Child Development Services) and National Health Mission
- Promotion of breastfeeding - exclusive breastfeeding for first 6 months; colostrum should not be discarded; breast milk is the ideal food for infants
- Development of low-cost weaning foods - indigenous weaning foods using cereals + pulses (e.g., amylase-rich foods); timely introduction at 6 months; frequent feeding
- Measures to improve family diet - promotion of balanced diet using locally available foods; kitchen gardens
- Nutrition education - correct feeding practices through health workers, ANMs (Auxiliary Nurse Midwives), anganwadi workers; POSHAN Abhiyaan (National Nutrition Mission)
- Home economics - better food preservation, cooking practices that retain nutrients
- Family planning and birth spacing - limiting family size, spacing births at least 2-3 years apart reduces competition for food and maternal resources
- Improving family environment - safe water, sanitation, reducing infection burden
(b) Specific Protection
- Diet must contain protein- and energy-rich foods - milk, eggs, pulses, fresh fruits and vegetables; protein-calorie supplements
- Immunization - prevents infections (measles, diarrheal diseases) that precipitate and aggravate PEM; under Universal Immunization Programme (UIP)
- Food fortification - fortification of commonly consumed foods; e.g., iodized salt, vitamin A in dalda (vanaspati), iron-fortified wheat flour (double-fortified salt)
(c) Early Diagnosis and Treatment
- Periodic growth surveillance - maintenance of Road-to-Health (growth) charts at anganwadi centres; monthly weight monitoring through ICDS
- Early diagnosis of growth faltering - detection before severe malnutrition develops
- Arm circumference measurement - <12.5 cm indicates severe malnutrition; easy to measure in field
- Early diagnosis and treatment of infections and diarrhea - ORS, zinc supplementation, antibiotic use
- Rehydration programmes - Oral Rehydration Therapy (ORT) for diarrheal dehydration
- Supplementary feeding during epidemics/emergencies
- Deworming - mass deworming programmes; helminth infestation worsens nutritional status
(d) Rehabilitation
- Nutritional Rehabilitation Services (NRS) - NRC (Nutritional Rehabilitation Centres) established in district hospitals; 14-day facility-based care using F-75/F-100 therapeutic feeds (WHO protocol)
- Hospital treatment - management of SAM with complications
- Follow-up care - regular follow-up after discharge; Community-Based Management of Acute Malnutrition (CMAM) using Ready-to-Use Therapeutic Food (RUTF)
India-Specific Programmes
| Programme | Description |
|---|---|
| ICDS (Integrated Child Development Services) | Supplementary nutrition, immunization, health check-up, referral services for 0-6 year children and pregnant/lactating women through anganwadi centres |
| POSHAN Abhiyaan (2018) | National Nutrition Mission targeting stunting, underweight, low birth weight, anemia reduction |
| Mid-Day Meal Scheme | Hot cooked meal to school children - addresses hunger and improves school attendance |
| National Food Security Act (2013) | Subsidized grains (5 kg/person/month) through PDS to 67% of population |
| PM POSHAN | Extended mid-day meal programme to pre-primary classes |
| NRC (Nutritional Rehabilitation Centres) | Facility-based management of SAM children |
- Park's Textbook of Preventive and Social Medicine, p. 737
d) Prevention & Social Measures Against Malnutrition at Family & Community Level
AT THE FAMILY LEVEL
1. Dietary Practices
- Ensure adequate intake of protein-rich foods (legumes, pulses, milk, eggs, meat/fish) at every meal
- Practice appropriate complementary feeding from 6 months; do not delay introduction of semisolid foods
- Feed children more frequently - small meals 5-6 times/day rather than 2-3 large meals
- Avoid giving only starchy staple foods; ensure dietary diversity (cereals + pulses + vegetables + fruits)
- Do not restrict food during illness (a common harmful practice); feed more during convalescence
2. Infant and Young Child Feeding (IYCF)
- Initiate breastfeeding within 1 hour of birth; give colostrum
- Practice exclusive breastfeeding for 6 months
- Continue breastfeeding up to 2 years with complementary foods
- Use locally available weaning foods - khichdi (rice + dal), ragi, sathu maavu
3. Maternal Nutrition
- Adequate nutrition during pregnancy and lactation - extra 300-500 kcal/day
- Regular antenatal care attendance, iron-folate supplementation
- Treat anemia before and during pregnancy
4. Family Planning
- Space births at least 3 years apart
- Limit family size to ensure each child receives adequate nutrition and care
5. Personal Hygiene and Sanitation
- Safe drinking water and proper sanitation reduce diarrheal diseases
- Hand washing before feeding children
- Proper food storage to prevent contamination
6. Income Generation
- Kitchen gardens (vegetable and fruit cultivation) to improve food security
- Poultry, dairy, backyard farming at household level
AT THE COMMUNITY LEVEL
1. Nutrition Education and Behaviour Change Communication (BCC)
- Community-based nutrition counselling by ANMs, ASHA workers, and anganwadi workers
- Dispelling food taboos and myths (e.g., eggs/fish not for children)
- Teaching mothers about growth monitoring and recognition of malnutrition signs
- Audio-visual campaigns, street plays (nukkad natak), radio messages
2. Growth Monitoring and Promotion
- Monthly weighing at anganwadi centres; plotting on growth charts
- Community-level identification of faltering children
- Grading of malnutrition (colour-coded growth charts - green/yellow/red zones)
- Village Health Nutrition Days (VHND)
3. Supplementary Feeding Programmes
- Anganwadi supplementary nutrition (ICDS) - take-home rations or hot cooked meals
- Mid-Day Meal Scheme in schools
- Therapeutic feeding at NRCs for SAM children
4. Immunization
- Full immunization under UIP protects against measles, diarrhea, whooping cough - all of which precipitate PEM
- Polio, DPT, BCG, Hepatitis B, Rotavirus vaccine
5. Control of Infections
- Mass deworming (National Deworming Day - 10 February; Albendazole 400 mg)
- ORT corners at sub-centres for management of diarrhea
- Zinc supplementation during diarrhea (20 mg/day for 14 days in children >6 months)
6. Food Security at Community Level
- Public Distribution System (PDS) - subsidized food grains
- National Food Security Act 2013 ensures entitlement to food
- Community grain banks (especially in tribal areas)
- Self-Help Groups (SHGs) for women - income and awareness
7. Social and Economic Measures
- Poverty alleviation programmes - MGNREGS, PM-KISAN
- Education of women - educated mothers make better nutritional choices
- Empowerment of women - women who control household income spend more on food and health
- Reduction of gender discrimination - girl child given equal food as boys
8. Water, Sanitation and Hygiene (WASH)
- Swachh Bharat Mission - construction of toilets, open defecation free villages
- Safe drinking water supply (Jal Jeevan Mission)
- Reduces diarrheal disease burden, breaking the malnutrition-infection cycle
9. Intersectoral Coordination
- Convergence of Health, ICDS (Women and Child Development), Education, Agriculture, and Rural Development departments
- POSHAN Abhiyaan (National Nutrition Mission, 2018) coordinates all nutrition interventions with district-level targets
10. Training of Frontline Workers
- Training of ASHAs, ANMs, anganwadi workers in growth monitoring, nutrition counselling, SAM identification, ORS preparation, and referral
- Capacity building in community management of acute malnutrition (CMAM)
Summary Table: Prevention at Different Levels
| Level | Key Measures |
|---|---|
| Individual/Family | Breastfeeding, complementary feeding, dietary diversity, maternal nutrition, hygiene |
| Community | Growth monitoring, supplementary feeding, immunization, nutrition education, deworming |
| Health System | NRCs, VHND, CMAM, RUTF, referral pathways |
| Policy/National | ICDS, POSHAN Abhiyaan, Mid-Day Meal, PDS, NFSA, Jal Jeevan Mission |
- Park's Textbook of Preventive and Social Medicine, p. 736-737
- Robbins & Kumar Basic Pathology, p. 288-291
I ****a) Define MALNUTRITION. & classify PEM b) Describe CAUSES & CLINICAL FEATURES of severe form of Malnutrition c) Explain PREVENTIVE measures to reduce PEM in India. d) Discuss in detail the prevention & social measures against malnutrition at family & community level I need that answer for an spm exam from sp m standard textbook
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
I have all the Park's SPM content needed. Now I'll write the comprehensive, exam-standard answer entirely from Park's perspective.
Malnutrition & PEM - SPM Exam Answer (Park's Textbook)
a) Definition of Malnutrition & Classification of PEM
Definition of Malnutrition
"Malnutrition is a pathological state resulting from a relative or absolute deficiency or excess of one or more essential nutrients." - (Park's SPM)
Malnutrition comprises four forms:
- Undernutrition - condition resulting from insufficient food eaten over an extended period; in extreme cases called starvation
- Overnutrition - pathological state from consumption of excessive quantity of food over extended period (e.g., obesity, diabetes, cardiovascular disease in western societies)
- Imbalance - pathological state from disproportion among essential nutrients, with or without absolute deficiency of any nutrient
- Specific deficiency - pathological state from a relative or absolute lack of an individual nutrient (e.g., scurvy, rickets)
On a global scale, the five principal nutritional deficiency diseases accorded highest priority are: wasting, stunting, xerophthalmia, nutritional anaemias, and endemic goitre. These represent the "tip of the iceberg" - a much larger population is affected by "hidden" malnutrition.
- Park's Textbook of Preventive & Social Medicine, p. 748
Classification of PEM
Protein-Energy Malnutrition (PEM) has been identified as a major health and nutrition problem in India, particularly in children in the first years of life. It is characterised by low birth weight if the mother is malnourished, poor growth in children, and high mortality in children between 12-24 months.
1. Wellcome Classification (Most widely used in SPM exams)
Based on body weight as % of expected weight-for-age and presence/absence of oedema:
| Condition | % Expected Weight | Oedema |
|---|---|---|
| Normal | >80% | Absent |
| Undernutrition | 80-60% | Absent |
| Kwashiorkor | 60-80% | Present |
| Marasmus | <60% | Absent |
| Marasmic-Kwashiorkor | <60% | Present |
2. IAP (Indian Academy of Pediatrics) Grading
Based on % of expected weight-for-age:
| Grade | % of Expected Weight |
|---|---|
| Normal | >80% |
| Grade I (Mild) | 71-80% |
| Grade II (Moderate) | 61-70% |
| Grade III (Severe) | 51-60% |
| Grade IV (Very Severe/SAM) | <50% |
3. WHO Z-score Classification (Anthropometric)
Three key indices - each expressed as Z-scores (SD units below the median of WHO Child Growth Standards):
| Index | Condition | Cut-off |
|---|---|---|
| Weight-for-Age | Underweight | < -2 SD (moderate); < -3 SD (severe) |
| Height-for-Age | Stunting (chronic/past malnutrition) | < -2 SD |
| Weight-for-Height | Wasting (acute/current malnutrition) | < -2 SD |
Severe Acute Malnutrition (SAM) is defined by WHO as:
- Weight-for-height Z-score below -3 SD, OR
- Mid-upper arm circumference (MUAC) < 115 mm, OR
- Presence of nutritional oedema
Children who are severely wasted are 9 times more likely to die than well-nourished children.
- Park's Textbook of Preventive & Social Medicine, p. 736-737
b) Causes & Clinical Features of Severe Malnutrition (Kwashiorkor & Marasmus)
KWASHIORKOR
Kwashiorkor is a severe form of undernutrition which develops in individuals on diets with a low protein/energy ratio. It commonly occurs when a child is displaced from the breast by a new baby and fed a predominantly carbohydrate diet.
Causes:
- Inadequate protein intake with relatively adequate calorie intake (low protein/energy ratio diet)
- Low concentration of essential amino acids in the diet
- Early abrupt weaning - displaced child fed on starchy gruels, diluted cereal porridges
- Infections - diarrhoea, measles, whooping cough precipitate/aggravate kwashiorkor
- Poverty and food insecurity
- Food taboos - restricting protein-rich foods (eggs, meat, fish) for children
- Ignorance of proper feeding practices
Clinical Features of Kwashiorkor:
| System | Feature |
|---|---|
| Oedema | Hallmark feature - pitting oedema, starts in feet/legs, progresses to face ("moon face"), abdomen (ascites) |
| Growth | Weight 60-80% of expected; actual weight loss masked by fluid retention |
| Skin | "Flaky paint" / "crazy pavement" dermatosis - alternating hyperpigmentation, desquamation, hypopigmentation |
| Hair | "Flag sign" - alternating bands of depigmented/normal colour; fine texture; easy pluckability; straightening |
| Liver | Hepatomegaly - fatty liver (steatosis) due to reduced lipoprotein synthesis |
| Mental/Behavioural | Apathy, listlessness, loss of appetite, irritability; "misery facies" |
| GI | Diarrhoea, vomiting, anorexia, distended abdomen |
| Muscle | Relative sparing of muscle (masked by oedema) |
| Lab | Hypoalbuminaemia - serum albumin reduced (key finding) |
| Immunity | Immune deficiency; susceptibility to secondary infections |
MARASMUS
Marasmus is caused by inadequate intake of both protein and energy - a form of severe cachexia with weight loss due to wasting in infancy and childhood.
Causes:
- Total calorie and protein deficiency - starvation
- Early or abrupt cessation of breastfeeding without adequate replacement
- Repeated infections - diarrhoea, respiratory infections in infancy
- Poverty - inability to purchase adequate food
- Large family size - competition for food
- Maternal malnutrition - low birth weight, inadequate breast milk
- Ignorance of proper infant feeding
Clinical Features of Marasmus:
| System | Feature |
|---|---|
| Weight | <60% of expected weight for age |
| Wasting | Severe generalised wasting of muscle and subcutaneous fat |
| Oedema | Absent - distinguishes from kwashiorkor |
| Appearance | Emaciated extremities; head appears disproportionately large ("old man in a baby's body"); "monkey facies" |
| Skin | Loose, wrinkled; "baggy pants" appearance; no dermatosis |
| Hair | May be thin, sparse - but no flag sign or depigmentation |
| Abdomen | Scaphoid (sunken) abdomen |
| Subcutaneous fat | Minimal or absent - measured skinfold thickness reduced |
| Serum albumin | Normal or near-normal (visceral protein relatively spared) |
| Immunity | Immune deficiency (T cell-mediated) - concurrent infections common |
| Behaviour | Misery, crying, but alert - unlike the apathy of kwashiorkor |
| MUAC | < 12.5 cm (severe malnutrition) |
Malnutrition-Infection Cycle
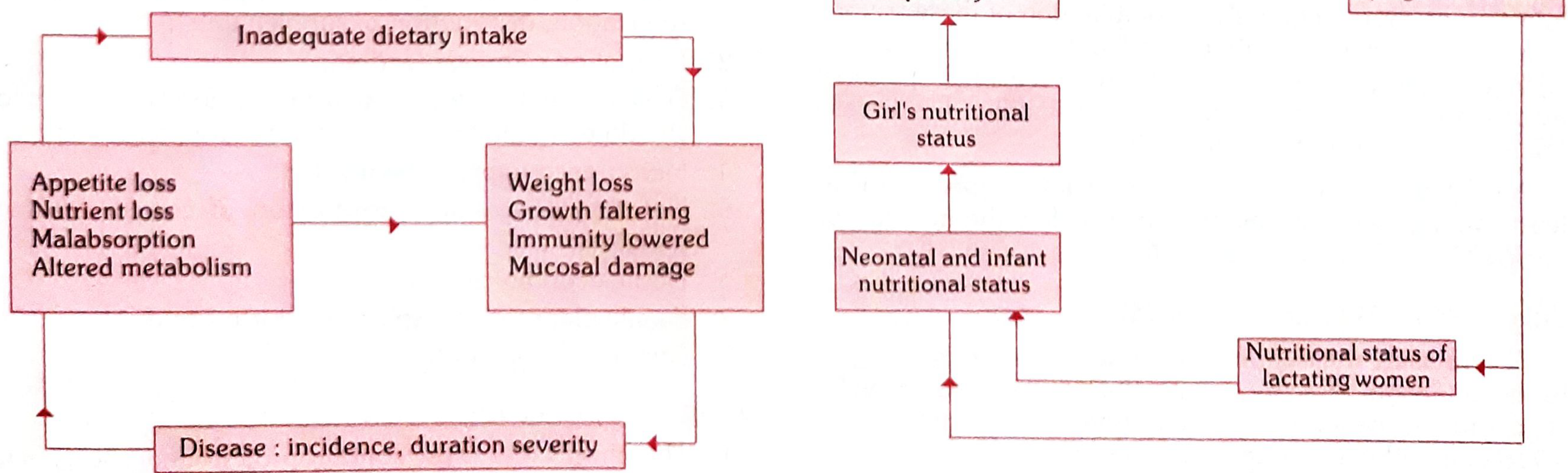
Infection contributes to malnutrition AND malnutrition causes otherwise minor childhood ailments to become killers - forming a vicious cycle. Children in developing areas may suffer some infection for almost half of their first three years of life.
c) Preventive Measures to Reduce PEM in India
"There is no simple solution to the problem of PEM. Many types of actions are necessary." - Park's SPM (adapted from 8th FAO/WHO Expert Committee on Nutrition)
(a) Health Promotion
- Measures directed to pregnant and lactating women - nutrition education, distribution of protein-calorie supplements; iron-folic acid supplementation; treatment of anaemia
- Promotion of breastfeeding - initiate within 1 hour of birth; give colostrum; exclusive breastfeeding for first 6 months; continue up to 2 years with complementary feeds
- Development of low-cost weaning foods - timely introduction at 6 months; child should be made to eat more food at frequent intervals; use locally available foods (khichdi, ragi, sattu)
- Measures to improve family diet - promote dietary diversity with locally available foods; kitchen gardens; encourage consumption of pulses, green leafy vegetables, fruits
- Nutrition education - promotion of correct feeding practices through health workers, ASHA, ANM, anganwadi workers; counter misleading commercial advertising for baby foods
- Home economics - better food preservation; cooking practices that retain nutrients; hygienic food preparation
- Family planning and spacing of births - limiting family size; spacing births at least 2-3 years apart reduces competition for food and maternal nutritional resources
- Family environment - improve the overall family environment including safe water, sanitation, housing
(b) Specific Protection
- Diet must contain protein- and energy-rich foods - milk, eggs, pulses, fresh fruits and vegetables; protein-calorie supplements through ICDS
- Immunization - full immunization under Universal Immunization Programme (UIP) prevents infections (measles, diarrhoea, pertussis) that precipitate PEM
- Food fortification - addition of nutrients to commonly consumed foods: vitamin A in vanaspati/dalda; iodised salt; iron-fortified flour (double-fortified salt)
(c) Early Diagnosis and Treatment
- Periodic nutritional surveillance - continuous monitoring of nutritional status in the community
- Growth monitoring - maintenance of growth charts (Road-to-Health cards) at anganwadi centres; monthly weighing; early diagnosis of any lag in growth
- Arm circumference measurement - MUAC: >13.5 cm = satisfactory; 12.5-13.5 cm = mild/moderate malnutrition; <12.5 cm = severe malnutrition
- Early diagnosis and treatment of infections and diarrhoea - ORS, zinc supplementation, antibiotic use when appropriate
- Rehydration programmes - Oral Rehydration Therapy (ORT) for diarrhoeal dehydration
- Supplementary feeding during epidemics/outbreaks
- Deworming of heavily infested children - National Deworming Day; Albendazole 400 mg
(d) Rehabilitation
- Nutritional rehabilitation services - Nutrition Rehabilitation Centres (NRCs) for inpatient management of SAM with complications; F-75 and F-100 WHO therapeutic feeds
- Hospital treatment - for complicated SAM (oedema, infections, hypoglycaemia, hypothermia)
- Community-Based Management of Acute Malnutrition (CMAM) - using Ready-to-Use Therapeutic Food (RUTF) for uncomplicated SAM
- Follow-up care - regular follow-up after discharge to prevent relapse
India-Specific National Programmes
| Programme | Key Interventions |
|---|---|
| ICDS (Integrated Child Development Services) | Supplementary nutrition, immunization, health check-up, health/nutrition education - targeting children 0-6 years and pregnant/lactating women through anganwadi centres |
| POSHAN Abhiyaan (2018) / National Nutrition Mission | Convergent nutrition improvement targeting stunting, underweight, anaemia, low birth weight with time-bound targets |
| Mid-Day Meal Scheme | Hot cooked meals to school children - combats hunger, improves school attendance |
| National Food Security Act (NFSA, 2013) | Subsidised food grains (5 kg/person/month) through PDS to 67% of population |
| Applied Nutrition Programme | Production of protective foods by the community for the community |
| NRC (Nutritional Rehabilitation Centres) | Facility-based 14-day management of SAM children in district hospitals |
- Park's Textbook of Preventive & Social Medicine, p. 737
d) Prevention & Social Measures Against Malnutrition at Family & Community Level
"Since malnutrition is the outcome of several factors, the problem can be solved only by taking action simultaneously at various levels - family, community, national and international levels." - Park's SPM
ACTION AT THE FAMILY LEVEL
The principal target of nutritional improvement in the community is the family. The instrument for combating malnutrition at the family level is nutrition education.
1. Nutrition Education
- The housewife is the "manager" of food consumption in the family; in some families, the husband also determines what foods reach the table
- Both husband and wife must be educated on selection of right local foods and planning of nutritionally adequate diets within their purchasing power
- Harmful food taboos and dietary prejudices can be identified and corrected (e.g., avoiding eggs/fish for children, food restrictions in pregnancy)
- Since food expenditure amounts to 50-70% of family budgets, nutrition education programmes are a good investment
2. Infant and Young Child Feeding (IYCF)
- Promote breastfeeding - initiation within 1 hour of birth, exclusive breastfeeding for 6 months
- Timely introduction of complementary foods - from 6 months; frequent small feeds; dietary diversity
- Counter misleading commercial advertising regarding baby foods
- Attention to nutritional needs of expectant and nursing mothers in the family
3. Food Production at Home
- Kitchen garden - planning a kitchen garden to grow vegetables, fruits
- Backyard poultry - to meet shortage of protective foods (eggs, meat)
- Adequate nutrition can be obtained in most countries with a combination of locally available and acceptable foods
4. Package of MCH Services
- Other related activities at the family level include the "package" of mother and child health, family planning and immunization services
- The community health workers and multipurpose workers are key people to impart nutrition education to families in their areas
5. Family Planning
- Spacing of births - reduces maternal nutritional depletion and competition for food among children
- Limiting family size - ensures adequate per-capita food availability
ACTION AT THE COMMUNITY LEVEL
Action at the community level should commence with:
- (a) Analysis of the extent, distribution and types of nutritional deficiencies
- (b) Identification of population groups at risk
- (c) Assessment of dietary and non-dietary factors contributing to malnutrition (through diet and nutrition surveys in representative samples)
1. Supplementary Feeding Programmes
- ICDS supplementary nutrition - take-home rations or hot cooked meals at anganwadis for children 6 months to 6 years and pregnant/lactating women
- Mid-Day Meal Scheme - school meals to reduce hunger and improve attendance
- These are regarded as stop-gap/palliative measures for rehabilitation of malnourished children - permanent solution requires more fundamental approaches
2. Applied Nutrition Programme (ANP)
- Promotes production of various types of protective foods by the community for the community
- Kitchen gardens, fisheries, poultry, dairy at community level
3. ICDS - Integrated Child Development Services
- Delivers a basic minimum package: supplementary nutrition + immunization + health check-ups + health and nutrition education for mothers + non-formal education for pre-schoolers
- Target groups: children up to 6 years, pregnant and lactating women, other women 15-44 years
4. Nutritional Surveillance
- "Continuous monitoring of factors/conditions which indicate, relate to, or impinge on nutritional status of individuals or groups of people" (WHO, 1976)
- Clinical examination + body measurements at health centres; surveys in villages
- Village Health Nutrition Days (VHND) - monthly weighing, growth monitoring
5. Nutritional Rehabilitation
- Children with severe PEM and complications: hospital/NRC-based care
- Less severely affected: managed on domiciliary basis or in special Nutrition Rehabilitation Centres linked with health centres
6. Immunization
- Full immunization under UIP protects against infections that precipitate PEM
- Children need immunization against: tuberculosis, diphtheria, whooping cough, tetanus, hepatitis B, Hib, Japanese encephalitis (endemic states), measles, and polio
7. Control of Infections and Diarrhoea
- ORT corners at sub-centres; zinc supplementation during diarrhoea
- Mass deworming programmes (National Deworming Day)
- Improvement of water supply and environmental sanitation
8. Health Education
- "About 50% of nutritional problems can be solved by appropriate educational action" - Park's SPM
- Community-level nutrition counselling by ASHA, ANM, anganwadi workers
- Audio-visual campaigns; behaviour change communication (BCC)
- Teaching mothers to recognise growth faltering and signs of malnutrition
9. Improvement in Living Conditions
- Safe drinking water supply (Jal Jeevan Mission)
- Improved sanitation - Swachh Bharat Mission - open defecation free villages
- Reduction of infection burden through WASH interventions
10. Broad Socio-Economic Development
- "A broad socio-economic development of the entire community is called for" - Park's SPM
- Poverty alleviation, women's empowerment, education of women
- Women's education is one of the most powerful predictors of child nutritional status
ACTION AT THE NATIONAL LEVEL (Brief Overview)
- Rural development - raise living standards and purchasing power, especially in rural India (72% of population)
- Increasing agricultural production - modern farming, irrigation, better seeds and fertilisers; food distribution system
- Stabilisation of population - population policy linked to food and nutrition policy
- Food distribution - Public Distribution System (PDS), National Food Security Act 2013
- Nutrition policy - National Nutrition Policy; POSHAN Abhiyaan with district-level targets
Key Points for Exam
Ecology of malnutrition (Jelliffe, 1966) - five conditioning factors:
- Conditioning influences (infections)
- Cultural influences (food habits, taboos, religion, food fads, cooking practices)
- Socio-economic factors (poverty, purchasing power)
- Food production (agriculture, availability)
- Health and other services (nutritional surveillance, rehabilitation, supplementation, health education)
"Malnutrition is a man-made disease. It is a disease of human societies. It begins quite commonly in the womb and ends in the grave." - Jelliffe; Park's SPM p. 748
Source: Park's Textbook of Preventive & Social Medicine (Park's SPM), pages 736-750
This is a shared conversation. Sign in to Orris to start your own chat.