CSF examination in CND infections This is a 10 marks shot answer in MUHS MD pathology exam. Give model answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a complete, exam-quality answer. Here is the model answer:
CSF Examination in CNS Infections
MUHS MD Pathology - 10 Marks Model Answer
Introduction
Cerebrospinal fluid (CSF) examination via lumbar puncture is the most important laboratory investigation in diagnosing CNS infections. Normal CSF is clear, colourless, with opening pressure 70-180 mmH₂O, WBC <5 lymphocytes/μL, protein 15-45 mg/dL, and glucose 45-80 mg/dL (CSF:serum glucose ratio >0.6).
Classification of CNS Infections by CSF Pattern
CNS infections are broadly divided into:
- Acute Pyogenic (Bacterial) Meningitis
- Aseptic (Viral) Meningitis
- Chronic Meningitis - Tuberculous, Fungal, Spirochetal
1. Acute Pyogenic (Bacterial) Meningitis
Gross appearance: Turbid/purulent, opalescent, may clot on standing.
CSF Findings:
| Parameter | Finding |
|---|---|
| Opening pressure | Markedly elevated (>180 mmH₂O) in 90% |
| Appearance | Turbid, purulent |
| Cell count | >100-10,000 cells/μL; PMN (neutrophil) predominance |
| Protein | Elevated >45 mg/dL in 90% (often 100-500 mg/dL) |
| Glucose | Decreased <40 mg/dL; CSF:serum glucose ratio <0.4 in ~60% |
| Gram stain | Positive in >60% of untreated cases |
| Culture | Positive in >70% |
Common organisms: Neisseria meningitidis (young adults), S. pneumoniae (elderly), E. coli/Group B Streptococci (neonates), Listeria monocytogenes (immunocompromised/elderly).
Pathology: Neutrophils fill the subarachnoid space; gram stain shows organisms in leptomeningeal exudate. Secondary vasculitis, venous thrombosis, and leptomeningeal fibrosis may follow.
(Robbins & Kumar Basic Pathology, p. 833; Harrison's 22E, p. 1164)
2. Aseptic (Viral) Meningitis
Gross appearance: Clear, water-like ("gin-clear").
CSF Findings:
| Parameter | Finding |
|---|---|
| Opening pressure | Normal or mildly elevated (100-350 mmH₂O) |
| Appearance | Clear |
| Cell count | 25-500 cells/μL; lymphocytic pleocytosis |
| Protein | Normal or mildly elevated (<150 mg/dL) |
| Glucose | Normal (CSF:serum ratio >0.6) |
| Gram stain | Negative |
| Culture | Negative on routine culture |
Special notes:
- In the first 24-48 hours of enteroviral meningitis, PMN predominance (up to 90%) may be seen in ~50% of patients, which shifts to lymphocytes subsequently.
- West Nile Virus meningitis may show PMN predominance persisting >1 week.
- Low CSF glucose with lymphocytosis should raise suspicion for TB, fungal, or Listeria meningoencephalitis rather than viral cause.
- PCR (FilmArray ME panel) is the diagnostic procedure of choice - sensitivity 85-100% for enteroviruses and HSV.
Common organisms: Enteroviruses (80% of cases), HSV-2, mumps, LCMV, arboviruses.
(Harrison's 22E, p. 1170; Robbins & Kumar, p. 834)
3. Tuberculous (Chronic) Meningitis
Gross appearance: Clear or slightly turbid; a characteristic cobweb/pellicle clot may form on standing (due to high fibrinogen content).
CSF Findings:
| Parameter | Finding |
|---|---|
| Opening pressure | Elevated |
| Appearance | Clear/faintly turbid; pellicle/cobweb clot |
| Cell count | Lymphocytic pleocytosis (10-500 cells/μL); mixed early |
| Protein | Markedly elevated, 1-5 g/L (100-500 mg/dL) |
| Glucose | Decreased (20-40 mg/dL); mild-to-moderate reduction |
| AFB smear | Positive in only 10-40% of adults |
| Culture | Positive ~50%; gold standard; takes 4-8 weeks |
| Nucleic acid | Xpert MTB/RIF Ultra for rapid detection |
Pathology: Chronic meningitis leads to arachnoid fibrosis at the base of the brain and hydrocephalus. Tuberculomas (intraparenchymal granulomas) may coexist.
(Harrison's 22E, p. 1170; Robbins & Kumar, p. 833)
4. Fungal Meningitis
Gross appearance: Clear or slightly turbid.
CSF Findings:
| Parameter | Finding |
|---|---|
| Cell count | Mononuclear/lymphocytic pleocytosis |
| Protein | Elevated |
| Glucose | Decreased |
| India ink | Encapsulated budding yeast cells (Cryptococcus) |
| Cryptococcal antigen | Highly sensitive and specific - diagnostic |
| Eosinophils | May be present in Coccidioides immitis meningitis |
Key test: Cryptococcal polysaccharide antigen test in CSF (highly sensitive and specific) - a positive result establishes the diagnosis.
(Harrison's 22E, p. 1170; Medical Microbiology 9e)
5. Syphilitic (Spirochetal) Meningitis
CSF Findings:
- Lymphocytic or mononuclear pleocytosis
- Elevated protein
- CSF VDRL: highly specific (when positive), but low sensitivity (~30-70%)
- Diagnosis confirmed by reactive serum FTA-ABS or MHA-TP combined with CSF pleocytosis
Comparative Summary Table
| Parameter | Bacterial | Viral | TB | Fungal |
|---|---|---|---|---|
| Appearance | Turbid/Purulent | Clear | Clear ± pellicle | Clear |
| Pressure | ↑↑↑ | Normal/↑ | ↑ | ↑ |
| WBC type | PMNs | Lymphocytes | Lymphocytes | Lymphocytes |
| WBC count | 100-10,000 | 25-500 | 10-500 | 10-500 |
| Protein | ↑↑ (100-500 mg/dL) | Normal/mild ↑ | ↑↑ (100-500 mg/dL) | ↑ |
| Glucose | ↓↓ (CSF:serum <0.4) | Normal | ↓ (mild-mod) | ↓ |
| Gram stain | Positive >60% | Negative | Negative | Negative |
| Special test | Culture/PCR/Gram | PCR (BioFire) | AFB smear/culture/Xpert | India ink/Ag test |
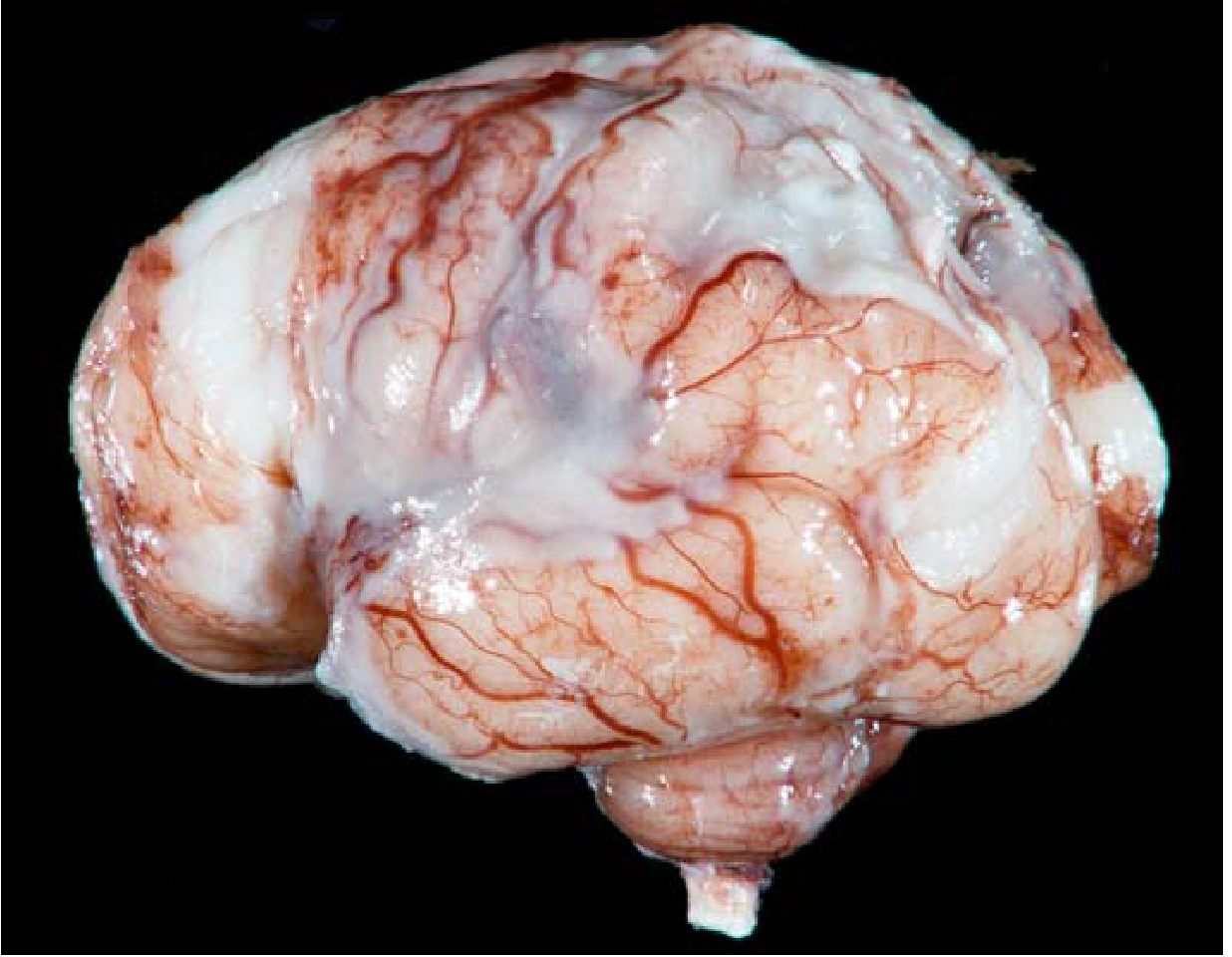
Gross Appearance - Pyogenic Meningitis
The image below (Robbins & Kumar, Fig. 21.16) shows a thick suppurative exudate covering the brain stem and leptomeninges in acute pyogenic meningitis:
Additional Investigations on CSF
- Opening pressure measurement before fluid collection
- Cell count and differential - centrifuge and examine
- Biochemistry - glucose (with simultaneous blood glucose), protein, lactate
- Microbiology - Gram stain, AFB smear, India ink (for Cryptococcus), ZN stain
- Culture - aerobic, anaerobic, fungal, mycobacterial
- Serology/Antigen tests - Cryptococcal antigen, VDRL, Lyme serology
- Molecular - PCR (FilmArray ME panel for 14 pathogens; Xpert MTB/RIF Ultra)
- Cytology - to exclude malignant/neoplastic meningitis
Key Exam Points to Remember:
- Bacterial meningitis = PMN pleocytosis + low glucose + high protein + turbid CSF
- Viral meningitis = lymphocytic pleocytosis + normal glucose + clear CSF
- TB meningitis = lymphocytic + markedly elevated protein + mild-moderate glucose drop + pellicle + low AFB smear sensitivity (10-40%)
- Fungal meningitis = lymphocytic + low glucose + India ink / Cryptococcal antigen positive
- CSF:serum glucose ratio <0.4 is highly suggestive of bacterial but also seen in TB/fungal/carcinomatous meningitis
Sources: Robbins & Kumar Basic Pathology 10e; Harrison's Principles of Internal Medicine 22E; Medical Microbiology 9e
This is a shared conversation. Sign in to Orris to start your own chat.