1. Discuss anatomical and biomechanical basis for management of wrist and hand movement dysfunction. 30 M (Winter 2022) 2. Rationale of P.T. treatment in extensor tendon injury 10 M(Winter 2022) Give me MPT level topper answer for MUHS exam with references and recent advances
extensor tendon injury rehabilitation hand
wrist biomechanics carpal kinematics
hand therapy physiotherapy tendon repair early active motion protocol
relative motion splint extensor tendon zones outcomes
wrist hand biomechanics carpal kinematics physiotherapy management dysfunction MPT level
MPT-Level Answer: MUHS Winter 2022
QUESTION 1
Anatomical and Biomechanical Basis for Management of Wrist and Hand Movement Dysfunction (30 Marks)
INTRODUCTION
PART A: ANATOMICAL BASIS
1. Osseous Architecture
- Formed by the sigmoid notch of the radius and the head of the ulna
- Stabilized primarily by the triangular fibrocartilage complex (TFCC) - a structure of critical biomechanical importance
- Permits forearm pronation-supination (approximately 90° each direction)
- TFCC injury results in DRUJ instability, pain on loading, and restricted forearm rotation - a common source of wrist dysfunction
- Articulation between the distal radius (which bears ~80% of axial load) and the proximal carpal row (scaphoid, lunate, triquetrum)
- The radial inclination (~22°) and volar tilt (~11°) are key parameters; any alteration (as in malunited distal radius fractures) disrupts load distribution and precipitates dysfunction
- Primary movements: flexion-extension, radial-ulnar deviation
- Articulation between the proximal and distal carpal rows
- Contributes approximately 50% of wrist flexion-extension
- The "dart-throwing" motion (radial extension to ulnar flexion) occurs predominantly at the midcarpal joint and is the most functional arc of wrist motion - foundational to rehabilitation target setting
2. The Carpal Architecture: Rows and Columns
- Scaphoid, lunate, triquetrum, pisiform
- Has no direct muscular attachments - it is a "slave" segment, controlled by ligaments
- This explains why ligament injuries (scapholunate instability) profoundly alter carpal kinematics
- Trapezium, trapezoid, capitate, hamate
- Firmly bound by the transverse carpal arch and well-muscled; far more stable than the proximal row
3. Ligamentous System
- Volar: Radioscaphocapitate, long radiolunate, short radiolunate (strongest, most important for stability)
- Dorsal: Dorsal radiocarpal, dorsal intercarpal ligaments
- Scapholunate interosseous ligament (SLIL) - most clinically significant
- Lunotriquetral interosseous ligament
4. Musculotendinous Anatomy
| Muscle | Primary Action | Clinical Note |
|---|---|---|
| ECRL, ECRB | Wrist extension + radial deviation | Tendinopathy at lateral epicondyle |
| ECU | Wrist extension + ulnar deviation | Subluxation in pronation |
| FCR | Wrist flexion + radial deviation | Tendinopathy at base of thenar |
| FCU | Wrist flexion + ulnar deviation | Pisiform stress fractures |
- APL, EPB (De Quervain's - 1st compartment)
- ECRL, ECRB
- EPL (Listers' tubercle pulley)
- EDC, EIP
- EDM
- ECU
- Extrinsic: Long flexors (FDS, FDP) and extensors (EDC) originate in the forearm
- Intrinsic: Lumbricals, interossei, thenar, hypothenar muscles originate within the hand
- Balance: The intrinsics flex the MCPs and extend the IPs; extrinsic extensors extend the MCPs. Loss of intrinsic function = "intrinsic minus" hand (claw deformity); loss of extrinsic extension = "intrinsic plus" hand. This balance is the backbone of splinting philosophy.
5. The Extensor Hood Mechanism
- Central slip: Inserts on dorsal base of the middle phalanx - extends the PIPJ
- Lateral bands: Pass on either side of the PIPJ and unite to form the terminal extensor tendon, inserting on the dorsal base of the distal phalanx - extends the DIPJ
- Oblique retinacular ligament (ORL): Tightens during PIPJ extension, passively extending the DIPJ - couples PIPJ and DIPJ extension
- Sagittal bands: Centralize the extensor tendon over the MCPJ; injury causes tendon subluxation
PART B: BIOMECHANICAL BASIS
1. Force Transmission and Load Sharing
- 80% of axial load is transmitted through the radiocarpal joint; 20% through the ulnocarpal joint (TFCC)
- Ulnar variance (relative length of ulna to radius) determines load sharing. Positive ulnar variance increases TFCC stress - relevant in TFCC tears, ulnar impaction syndrome
- The scaphoid spans both carpal rows, acting as a kinematic link and load-bearing strut; 60% of compressive load passes through the scaphoid
2. Carpal Kinematics: Columnar vs. Row Theories
- Wrist flexion-extension occurs at both radiocarpal (RC) and midcarpal (MC) joints, with each contributing approximately 50%
- Radial deviation: primarily midcarpal; Ulnar deviation: primarily radiocarpal
- The proximal row behaves as an intercalated segment - it has no muscle attachment and is driven by ligament tension and bony geometry
- The functional diagonal arc from radial extension to ulnar flexion
- During DTM, the proximal carpal row barely moves relative to the radius - near-isometric behavior
- Has direct application: post-wrist injury rehabilitation should preserve and restore DTM early, as it is the most used wrist arc in activities of daily living. Splints that allow DTM (DTM orthoses) are now used post-distal radius fracture to maintain function.
3. Tendon Excursion and Moment Arms
- FDP requires approximately 3 cm of excursion for full digital flexion
- EDC requires approximately 5 mm of excursion per MCPJ flexion degree
- Mechanical advantage is determined by the moment arm of each tendon at each joint
- The wrist position profoundly affects tendon efficiency: wrist extension tightens the long flexors (enhancing grip), while wrist flexion tightens the long extensors (enhancing digital extension). This is the biomechanical rationale for positioning the wrist in extension (20-30°) in the "position of function" splint
4. Tenodesis Effect
- Wrist extension → passive finger flexion (via FDP/FDS tightening)
- Wrist flexion → passive finger extension (via EDC tightening)
- Used therapeutically in tenodesis splints for C6 SCI patients to provide functional grip without active hand muscles
- Also employed in early mobilization post-tendon repair to produce controlled tendon excursion without active muscle contraction
5. Three-Point Bending and Joint Forces
- The MCP joint functions as a condyloid joint; collateral ligaments are taut in flexion (cam effect) and lax in extension
- This is why MCP joints must be splinted in 70-90° of flexion to prevent collateral ligament contracture
- The PIP joint is a hinge joint; its volar plate and collateral ligaments are at risk of contracture after immobilization, making early PIP mobilization a priority
PART C: CLASSIFICATION OF WRIST AND HAND MOVEMENT DYSFUNCTION
| Dysfunction Type | Anatomical Basis | Biomechanical Consequence |
|---|---|---|
| Carpal instability (DISI/VISI) | Ligament disruption (SLL/LTL) | Altered carpal kinematics, pain, crepitus |
| Wrist stiffness post-fracture | Capsular contracture, malunion | Restricted flexion-extension arc |
| Extensor tendon injury | Disruption of extensor hood | Zone-specific deformities |
| Intrinsic tightness | Spasticity/fibrosis of interossei | PIP extension lag with MCP flexion |
| Extrinsic tightness | FDP/FDS scarring | Loss of composite digital extension |
| Nerve lesions | Median/ulnar/radial palsy | Intrinsic-extrinsic imbalance patterns |
PART D: PHYSIOTHERAPY MANAGEMENT - ANATOMICAL AND BIOMECHANICAL RATIONALE
1. Splinting
- Wrist: 20-30° extension (optimizes tenodesis, prevents flexion contracture)
- MCPJs: 70-90° flexion (tenses collateral ligaments, prevents hyperextension contracture)
- IPJs: 0-10° flexion (prevents FDP/FDS contracture)
- Thumb: palmar abduction (prevents first web space contracture)
- Static (for acute injury, immediate post-operative): immobilizes to protect repair
- Dynamic (spring-assisted): applies low-load prolonged stress on contracted structures - used in Dupuytren's post-fasciotomy, post-burn contracture
- Serial static: progressive end-range positioning - used for established joint contractures
- Relative motion splint: positions the injured digit's MCPJ in slight extension relative to adjacent digits - reduces extensor tendon tension - modern standard for zones V-VI extensor repairs (Evidence: RCT, Buhler et al., JHSR 2023)
2. Exercise Therapy
- Biomechanical goal: Prevent adhesion formation, maintain tendon excursion, preserve joint mobility
- Tendon gliding exercises (hook fist → full fist → tabletop → straight fist): maximize differential tendon gliding between FDP and FDS
- Place-and-hold technique: passive positioning followed by active muscle contraction produces controlled tendon load without full excursion stress
- Dart-throwing motion exercises: exploit the functional diagonal arc
- Intrinsic plus/minus exercises: individually target intrinsic vs. extrinsic contributions
- Putty/Thera-band: progressive resistance targeting wrist stabilizers
- Grip and pinch dynamometry-guided progressive resistance
- Wrist proprioceptive training (unstable surfaces, oscillatory tools like FlexBar)
- Work hardening / task-specific training
3. Manual Therapy
- Joint mobilization (Maitland/Kaltenborn): Carpal joint glides in the plane of the facet. Radiocarpal dorsal-volar glides restore wrist flexion-extension. Midcarpal anterior-posterior glides restore dart-throwing arc.
- Soft tissue mobilization: Scar management post-repair (silicone gel, compression, transverse friction)
- Nerve gliding: Neural mobilization for associated median/ulnar nerve tethering
4. Electrophysical Agents
| Modality | Biomechanical Rationale | Application |
|---|---|---|
| TENS / IFC | Gate control / pain relief | Post-repair, to enable exercise |
| Ultrasound | Thermal: increases tissue extensibility; Non-thermal: collagen realignment | Scar/contracture management |
| LLLT | Photobiomodulation - reduces fibrosis, promotes tendon healing | Post-tendon repair |
| Wax bath (paraffin) | Increases local tissue temperature and extensibility | Pre-exercise for stiff joints |
| FES/NMES | Recruits paralyzed muscles (nerve palsy, SCI) | Functional electrical stimulation splint |
5. Biomechanics of Carpal Tunnel and Peripheral Nerve Entrapment Management
- Neutral wrist night splinting (reduces overnight pressure elevation)
- Nerve and tendon gliding exercises
- Activity modification to minimize provocative positions
RECENT ADVANCES (Critical for MPT Exam)
-
4D CT / Dynamic CT: Now allows real-time visualization of carpal kinematics during motion. This has redefined understanding of scapholunate instability staging (Wessel & Wolfe, J Hand Surg 2023, PMID: 37452815).
-
Dart-Throwing Motion Orthoses: New wrist orthoses that restrict radial/ulnar deviation while permitting the DTM arc have shown superior function preservation post-distal radius fracture compared to conventional immobilization.
-
Relative Motion Splinting (RMS): Evidence confirms RMS is non-inferior to dynamic extension splinting for zones V-VI extensor tendon repairs and is easier for patients to use (Buhler et al. 2023, PMID: 37045642). The 2026 RCT (Cela-Lopez et al., PMID: 41761624) further supports RMS for zones IV-VI.
-
Finite Element Analysis (FEA) of the Wrist: Computational biomechanical models have improved understanding of scaphoid fracture fixation and carpal tunnel syndrome mechanics, guiding conservative management strategies.
-
Wrist Kinematics in Rehabilitation: Studies confirm that exercises targeting DTM should be a standard part of all wrist rehabilitation programs due to their low proximal row motion and functional relevance.
REFERENCES
- Eschweiler J, et al. Anatomy, Biomechanics, and Loads of the Wrist Joint. Life (Basel). 2022;12(2):188. [PMID: 35207475]
- Wessel LE & Wolfe SW. Scapholunate Instability: Anatomy, Kinematics, and Clinical Assessment. J Hand Surg Am. 2023 Nov. [PMID: 37452815]
- Miller's Review of Orthopaedics, 9th Edition (2024). Wrist and Hand Section.
- Sabiston Textbook of Surgery, 21st Edition. Extensor Tendon Injuries, Chapter 119.
- Roberts & Hedges' Clinical Procedures in Emergency Medicine. Extensor Tendon Injuries. Chapter 48.
- Tintinalli's Emergency Medicine, 9th Edition. Extensor Tendon Lacerations.
- Buhler M, et al. Relative motion orthoses for zones V-VI extensor tendon repairs: RCT. J Hand Ther. 2023. [PMID: 37045642]
- Shaw AV, et al. Relative motion orthoses for early active motion: Systematic Review. J Hand Ther. 2023. [PMID: 37037728]
QUESTION 2
Rationale of Physiotherapy Treatment in Extensor Tendon Injury (10 Marks)
INTRODUCTION
ANATOMICAL BACKGROUND: ZONES OF EXTENSOR TENDON INJURY
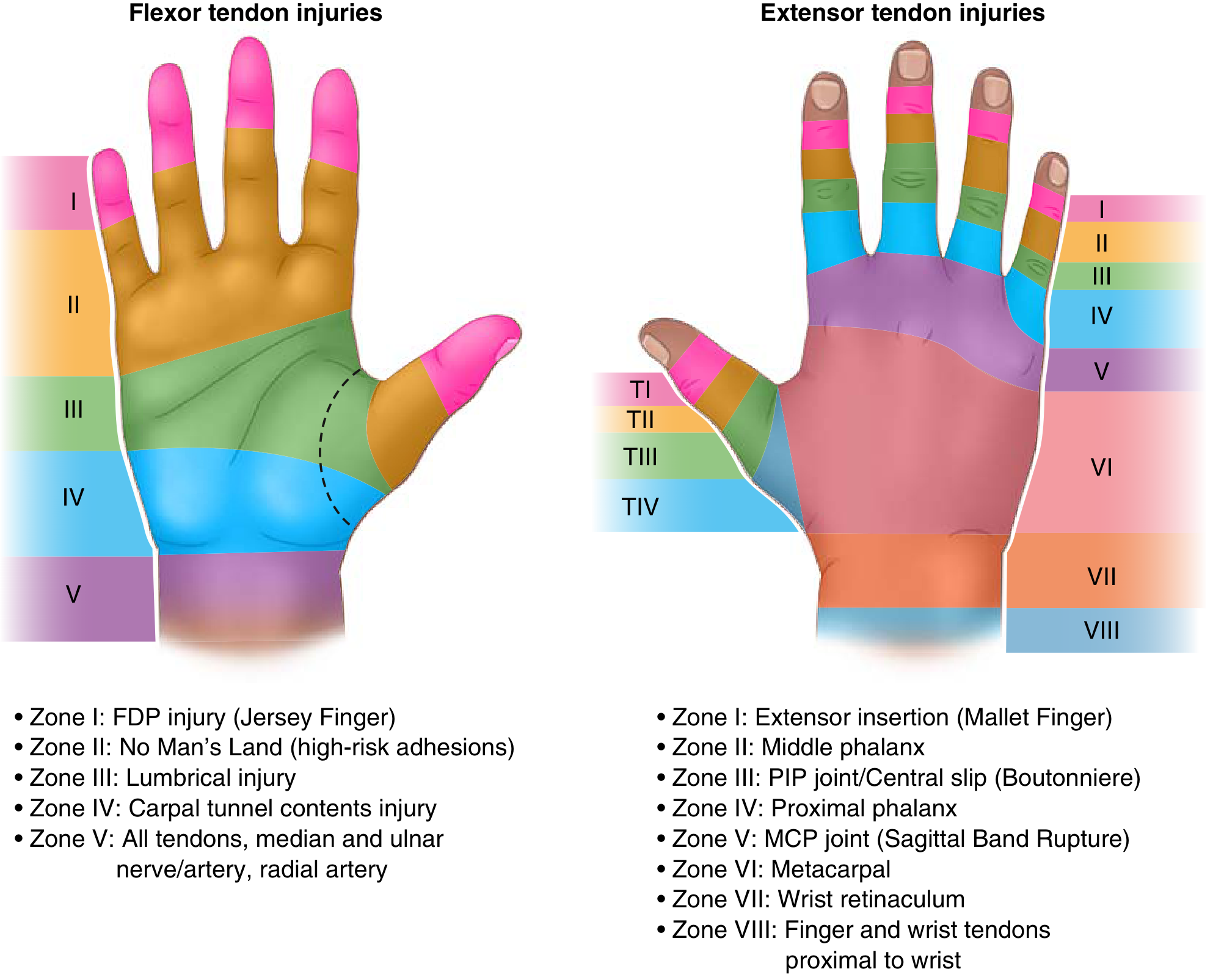
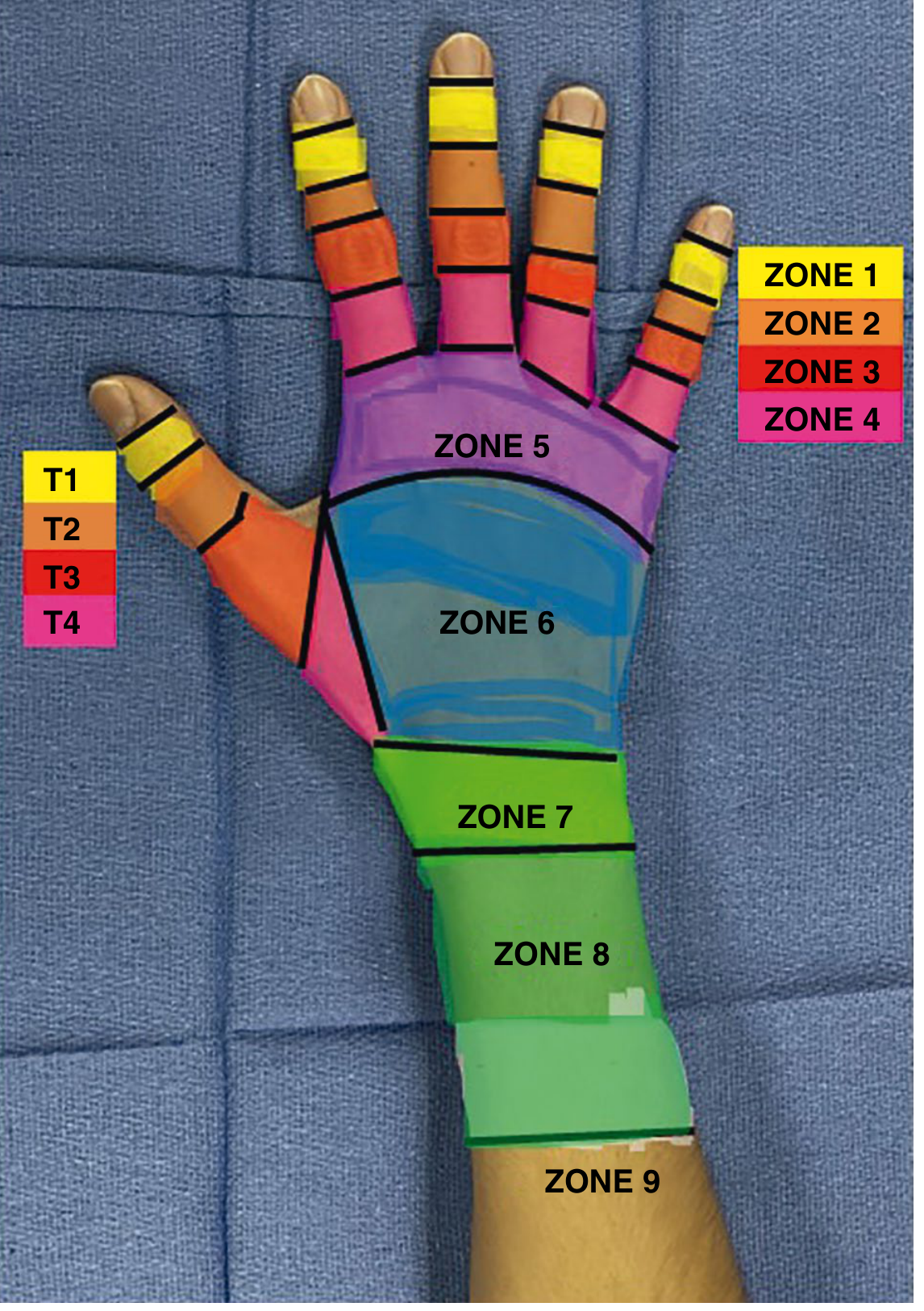
| Zone | Location | Injury Pattern |
|---|---|---|
| I | DIP joint / distal phalanx | Mallet finger |
| II | Middle phalanx | Dorsal laceration |
| III | PIP joint (central slip) | Boutonniere deformity |
| IV | Proximal phalanx | Adhesion-prone |
| V | MCP joint (sagittal band) | Tendon subluxation |
| VI | Metacarpal | Most common injury zone |
| VII | Extensor retinaculum | Adhesions within retinaculum |
| VIII/IX | Distal/proximal forearm | Musculotendinous junction |
RATIONALE FOR PHYSIOTHERAPY
I. Prevention of Deformity (Primary Rationale)
- Terminal tendon disruption causes DIPJ to drop into flexion
- Prolonged unrecognized mallet deformity allows lateral bands to migrate dorsally over the PIPJ, creating swan-neck deformity (DIPJ flexion + PIPJ hyperextension)
- PT Rationale: Static DIPJ extension splinting (Stack splint) for 6-8 weeks prevents chronic mallet and swan-neck. The PIPJ must be actively exercised to prevent FDS contracture. Night splinting for 4-6 additional weeks.
- Central slip disruption + volar subluxation of lateral bands below PIPJ axis
- Results in PIPJ flexion + DIPJ hyperextension
- PT Rationale: Static PIPJ extension splinting for 6 weeks with active DIPJ flexion maintained. Active DIPJ flexion encourages dorsal migration of lateral bands, gradually restoring the extensor mechanism balance (biomechanical rationale: ORL becomes slack when DIPJ is flexed with PIPJ extended).
II. Prevention of Adhesion Formation
- Even limited tendon excursion (1-2 mm) during controlled early motion provides the mechanical stimulus for organised collagen remodeling along lines of stress (Wolff's Law applied to tendon)
- Prevents adhesion maturation and cross-linking
- Maintains the intrinsic-extrinsic balance by preventing fibrous tethering between layers
III. Phase-Based Rehabilitation Protocol (Evidence-Based)
- Zones I-II: Static DIPJ extension splinting; maintain PIPJ active flexion
- Zones III-IV: Static PIPJ extension splinting (Stack or Capener); short-arc-motion protocol (SAM) may be started at 1-2 days: active PIPJ motion from 0-30° progressing to 0-50° by week 4. Dynamic splinting now available as alternative.
- Zones V-VII: Dynamic extension splinting (wrist at 45° extension, MCPs in neutral with volar block allowing 30-40° MCP flexion, dynamic traction mechanism passively extends digits). OR Relative Motion Splinting (positions repaired digit's MCP in 15-20° more extension than adjacent digits, offloading the repaired zone V/VI tendon during active motion). EAM begins at 1-3 days post-repair.
- Zone VII (wrist retinaculum): Splint wrist in mild extension; early protected active motion because synovial adhesions form rapidly within the retinaculum.
- Progressive active composite flexion and extension exercises
- Place-and-hold technique (passive full composite flexion held actively)
- Tendon gliding exercises: hook fist, full fist, tabletop, straight fist
- Scar management: compression garments, silicone gel, retrograde massage
- Progressive resistance using putty, therapy balls, pinch/grip dynamometry
- Return to function: grip, pinch, functional task training
- Sensory re-education if associated nerve injury
- Work hardening if occupationally relevant
IV. Splinting Rationale - Biomechanical Summary
| Splint Type | Zone | Rationale |
|---|---|---|
| Stack/extension splint | I-II | Prevents terminal tendon gapping; allows healing at correct length |
| PIP extension splint | III-IV | Prevents boutonniere; keeps central slip approximated |
| Dynamic extension splint | V-VII | Allows controlled tendon gliding; prevents MCP extension lag |
| Relative motion splint | V-VI | Reduces tendon excursion demands at repaired site; allows full hand use |
| Forearm-based wrist splint | VII | Reduces retinacular adhesions; protects wrist extensor repair |
V. Rationale of Electrophysical Modalities
- LLLT (Low-Level Laser Therapy): Promotes fibroblast activity and collagen synthesis aligned along tendon axis
- Ultrasound (pulsed): Non-thermal cavitation promotes cellular repair; thermal mode used at 4+ weeks to increase tissue extensibility before stretching
- TENS: Reduces post-operative pain, enabling compliance with early mobilization protocols
- Wax bath: Pre-exercise thermal modality to increase tissue extensibility and reduce stiffness
VI. Patient Education and Compliance
- Patients must understand that premature active resistance can cause tendon rupture (most common complication in zones V-VII)
- Splint compliance (especially for zone I mallet - 100% continuous wear required for 6-8 weeks)
- Failure of mallet splinting is the most common cause of swan-neck deformity - patient non-compliance is the primary cause
COMPLICATIONS PREVENTED BY APPROPRIATE PT
| Complication | Zone | Prevention Strategy |
|---|---|---|
| Swan-neck deformity | I | Continuous DIP extension splinting |
| Boutonniere deformity | III | Central slip protection + DIP active flexion |
| MCP extension lag | V | Dynamic/relative motion splinting |
| Tendon rupture | All | Compliance education; staged resistance progression |
| Retinacular adhesions | VII | Early motion within retinaculum |
| PIP contracture | III-IV | Maintain PIP passive flexion during immobilization |
RECENT ADVANCES
-
Relative Motion Splinting (RMS) is now strongly supported as first-line for zones V-VI repairs: Buhler et al. (2023, PMID: 37045642) - RCT showing RMS is non-inferior to dynamic extension splinting with better cost-effectiveness. The 2026 RCT by Cela-Lopez et al. (PMID: 41761624) confirms RMS superiority over classic immobilization for zones IV-VI.
-
New classification by Tang JB (2025, PMID: 41025781) proposes simplified zone classification (8 zones) with protocol modifications emphasizing stronger suture repairs allowing earlier mobilization with better outcomes.
-
Telerehabilitation for hand injuries: Seven et al. (2024, PMID: 38307736) demonstrated comparable functional outcomes with telerehabilitation, with implications for access and compliance monitoring.
-
Short-arc-motion protocols are now recognized as safe for zones III-IV with no increased rupture risk, offering better functional outcomes compared to static splinting alone.
REFERENCES
- Miller's Review of Orthopaedics, 9th Edition. Extensor Tendon Injury Zones. WBSF.
- Sabiston Textbook of Surgery, 21st Ed. Chapter 119: Extensor Tendon Injuries. [Zone-wise management]
- Roberts & Hedges' Clinical Procedures in Emergency Medicine. Postrepair Care and Rehabilitation. Chapter 48.
- Tintinalli's Emergency Medicine, 9th Ed. Extensor Tendon Lacerations.
- Buhler M, et al. Relative motion orthoses vs. dynamic splinting for zones V-VI: RCT. J Hand Ther. 2023. [PMID: 37045642]
- Shaw AV, et al. Relative motion orthoses systematic review. J Hand Ther. 2023. [PMID: 37037728]
- Tang JB. Extensor tendon injuries: a new classification, strong repairs, and easier therapy. Plast Reconstr Surg. 2025. [PMID: 41025781]
- Cela-Lopez M, et al. Relative Motion Extension Orthosis vs Classic Immobilization, Zones IV-VI: RCT. Hand (N Y). 2026. [PMID: 41761624]
- Campbell's Operative Orthopaedics, 15th Ed 2026. Extensor Tendon Rupture and Realignment.
EXAMINER TIPS (MPT Topper Insight)
- Q1 (30M): Structure under: Anatomy → Biomechanics → Classification of Dysfunction → PT Management principles. Use tables, clearly labeled headings, and biomechanical concepts (DISI, dart-throwing motion, tenodesis, intrinsic-extrinsic balance). Connect every anatomical point to a management implication.
- Q2 (10M): Focus on the rationale, not just the protocol. For every intervention, write "because" - give the biomechanical or biological justification. Zone-specific approach + phases + deformity prevention = complete answer.
- Always mention at least 2-3 recent advances citing year and journal for MPT-level differentiation.
- Diagrams of extensor zones and deformities (mallet, boutonniere, swan-neck) earn significant marks.
3. Enumerate various hand grips. Mention one method of evaluation for the same. 10 M(winter 2022) 4. Explain the principles of hand splinting. 10 M(Summer 2020 MPT level topper style answer for MUHS exam with references and recent advances
hand grip strength assessment dynamometry
hand splinting orthosis rehabilitation principles
handgrip strength normative values Jamar dynamometer
hand grip classification prehension types power precision lateral pinch MPT physiotherapy
hand grip prehension classification functional assessment
Napier 1956 hand grip classification Landsmeer Elliot prehension types physiotherapy evidence
https://www.physio-pedia.com/Grip_Strength
hand orthosis splinting contracture prevention rehabilitation
grip strength vital sign sarcopenia frailty health outcomes
MPT-Level Answers: MUHS Winter 2022 / Summer 2020
QUESTION 3
Enumerate Various Hand Grips. Mention One Method of Evaluation. (10 Marks)
INTRODUCTION
CLASSIFICATION OF HAND GRIPS
PART I: NAPIER'S FUNDAMENTAL CLASSIFICATION (1956)
| Feature | Power Grip | Precision Grip |
|---|---|---|
| Thumb position | Adducted, wraps around object | Abducted, opposed to fingers |
| Object position | Against palm and fingers | Held between fingertips |
| Hand position | Static (immobilizes object) | Dynamic (manipulates object) |
| Muscles dominant | Extrinsic long flexors | Intrinsic + extrinsics together |
| Force generated | High | Low (fine motor) |
| Example | Holding hammer | Writing with pen |
PART II: POWER GRIPS (Detailed Classification)
1. Cylindrical Grip (Palmar Grip / Fist Grip)
- Object grasped in palm with all four fingers flexed uniformly and thumb adducted as a buttress
- MCPJs: 45-55° flexion; PIPJs: 70-90° flexion; DIPJs: 50° flexion
- Muscles: FDP, FDS, intrinsics, adductor pollicis
- Clinical relevance: First structure to be lost in median/ulnar nerve palsy; evaluated in grip strength testing
- Examples: Holding a mug, hammer, door handle
2. Spherical Grip (Ball Grip)
- Object grasped as a sphere; fingers spread and curved with thumb in opposition
- Requires full opposition of thumb (CMC joint) and adduction of all fingers
- Requires intrinsic muscle activity to maintain digital abduction with flexion
- Examples: Holding a tennis ball, orange
3. Hook Grip
- MCPJs remain extended (or hyperextended); PIPJs and DIPJs strongly flexed; thumb not involved
- Flattens the transverse arch of the hand
- Used when heavy loads are suspended from fingers
- Pure extrinsic grip - does NOT require intrinsic muscles
- Clinical importance: The only grip available in intrinsic minus hand (combined median + ulnar palsy, T1 lesion, Dupuytren's contracture); preserved in leprosy patients with intrinsic paralysis
- Examples: Carrying a briefcase, hanging from a bar
4. Lateral (Key) Prehension - Power Variant
- Thumb adducted against the radial side of the index finger
- Used for power tasks where the object is stabilized on both sides
- Example: Holding a key to turn a lock (initial forceful phase)
PART III: PRECISION GRIPS (Detailed Classification)
1. Pad-to-Pad Pinch (Palmar Pinch / Pulp Pinch)
- Pulp of thumb opposes pulp of index finger ± middle finger
- Three-jaw chuck / tripod pinch: thumb pulp opposes pulps of index + middle fingers simultaneously - strongest precision grip
- Requires: APB, OP (thenar muscles), 1st dorsal interosseous, FPL, FDP
- Examples: Holding a pen, picking up a coin, pinching salt
2. Tip-to-Tip Pinch (Tip Pinch)
- Thumb tip precisely opposes fingertip with both DIPJs in flexion
- Requires FDP activation (to maintain DIPJ flexion) and FPL
- Used for handling small, fragile objects with maximum precision
- Examples: Threading a needle, turning a watch crown
3. Lateral Pinch (Key Pinch / Pad-to-Side Grip)
- Thumb pulp presses against lateral (radial) aspect of the middle phalanx of the index finger
- Requires adductor pollicis (ulnar nerve) - hence absent in ulnar nerve palsy (Froment's sign)
- Strongest type of pinch grip (generates ~40% more force than tip pinch)
- Examples: Holding a key to unlock, turning a page
4. Lumbrical Grip (Interdigital Grip)
- Object held between adjacent fingers (without thumb)
- MCPJs flexed, IPJs extended (intrinsic plus position)
- Exclusively intrinsic muscle activity (lumbricals + interossei)
- Examples: Holding cigarette between index and middle fingers, holding chopsticks
5. Tripod Pinch (Three-Jaw Chuck)
- Subtype of pad-to-pad: thumb opposes index and middle finger pulps simultaneously
- Provides greater stability than two-point pinch
- Most commonly used grip in fine motor writing and tool manipulation
PART IV: INTERMEDIATE / TRANSITIONAL GRIPS
- Variant of power grip across a rectangular surface (e.g., a book)
- Approximately 65% of power grip strength
- Strongly influenced by grip span
- Between adjacent finger surfaces (without thumb)
- Used in cigarette holding, syringe holding between surgical fingers
PART V: DEVELOPMENTAL PROGRESSION of Grip
| Age | Grip Type Emerging |
|---|---|
| 3-4 months | Palmar grasp (whole hand) |
| 6-8 months | Radial palmar grasp (thumb-assisted) |
| 8-12 months | Radial digital grasp |
| 9-12 months | Inferior pincer (lateral pinch) |
| 12 months | Superior (tip) pincer grasp |
| 3-5 years | Tripod pinch matures |
PART VI: MUSCLES UNDERLYING GRIP FUNCTION
| Component | Muscle(s) | Nerve Supply |
|---|---|---|
| Finger flexion (power) | FDS, FDP | Median + Ulnar |
| Thumb opposition | APB, OP | Median (C8, T1) |
| Thumb adduction | Adductor pollicis | Ulnar (C8, T1) |
| Intrinsic flexion | Lumbricals, interossei | Median + Ulnar |
| Hook grip maintenance | FDP, FDS (no intrinsics) | Median + Ulnar |
| Lateral pinch | Adductor pollicis | Ulnar |
EVALUATION OF HAND GRIPS: JAMAR DYNAMOMETRY
Rationale for Assessment
Instrument Description
- Adjustable anatomical rigid handle - 5 grip positions (1" to 3" span, adjustable in 0.5" increments)
- Closed hydraulic system - measures force in kilograms or pounds
- Analogue display with dual-pointer (one pointer holds peak value; second pointer follows live force)
Standardized Test Protocol (American Society of Hand Therapists - ASHT Recommended Position)
- Seated with shoulder adducted to side, elbow flexed to 90°
- Forearm in neutral (thumb up) position
- Wrist in 0-15° extension, neutral deviation
- Dynamometer handle adjusted to the 2nd or 3rd position (optimal span ~2 inches for most adults)
- No support of the forearm (free hanging)
- Position: as described above; consistent between sessions
- Instruct patient: "Squeeze as hard as you can"
- 3 trials for each hand, with 30-60 second rest between trials
- Record both dominant and non-dominant hands
- Calculate: Mean of 3 trials is the reported grip strength
- Alternate hands between trials (DH, NDH, DH, NDH, DH, NDH) is the recommended sequence
| Gender | Dominant Hand | Non-dominant Hand |
|---|---|---|
| Adult male | 40-55 kg | 35-50 kg |
| Adult female | 25-35 kg | 20-30 kg |
- Dominant hand is typically 10-12% stronger than non-dominant
- In left-handed individuals, strength is generally equal in both hands
- Grip strength <26 kg (male) / <18 kg (female) = diagnostic for sarcopenia (EWGSOP2 criteria)
- Serial measurements track rehabilitation progress objectively
- The Bell curve / rapid exchange grip test differentiates true grip weakness from malingering (in genuine weakness, highest grip at position 2-3; in feigned weakness, near-equal force at all positions)
Pinch Strength Evaluation (Pinch Dynamometer / Pinchmeter)
| Test | Technique | Normal Value |
|---|---|---|
| Lateral pinch (key pinch) | Pinchmeter between radial side of index and thumb pulp | 5-8 kg |
| Palmar (three-jaw chuck) | Pinchmeter between thumb pulp and index + middle pulp | 4-7 kg |
| Tip pinch | Pinchmeter between thumb tip and index fingertip | 3-5 kg |
RECENT ADVANCES
-
Grip Strength as a Vital Sign: A 2024 systematic review established grip strength as a reliable biomarker for all-cause mortality, cardiovascular events, hospital length of stay, and sarcopenia screening - validating its routine use in hand rehabilitation outcome tracking (PMC: pmc.ncbi.nlm.nih.gov/articles/PMC10777545).
-
International Normative Data (2025): Tomkinson et al. published the largest normative database to date - 2.4 million adults from 69 countries - enabling precise age-, sex-, and population-adjusted grip strength targets for clinical rehabilitation (PMID: 39647778).
-
GRASP Taxonomy (Feix et al., 2016): A computer-vision-informed taxonomy classified 33 distinct grasp types into Power, Precision, and Intermediate categories with sub-typing by thumb opposition and finger-palm contact. Used in robotic prosthetics and AI-driven rehabilitation.
-
Wearable Grip Sensors: Smart gloves with embedded pressure sensors now allow continuous grip force mapping during ADL tasks, enabling real-time task-specific rehabilitation feedback.
-
Automated Hand Prehension Assessment from Egocentric Video after spinal cord injury (Zhao & Zariffa, IEEE Trans Neural Syst Rehabil Eng, 2024, PMID: 39102325) - AI-based prehension grading without manual assessment.
REFERENCES
- Napier JR. The prehensile movements of the human hand. J Bone Joint Surg Br. 1956;38(4):902-913.
- Elliott JM & Connolly KJ. A classification of manipulative hand movements. Developmental Medicine & Child Neurology. 1984;26(3):283-296.
- Tomkinson GR, et al. International norms for adult handgrip strength. J Sport Health Sci. 2025. [PMID: 39647778]
- Feix T, et al. The GRASP Taxonomy of Human Grasp Types. IEEE Trans Human-Machine Systems. 2016;46(1):66-77.
- Zhao N & Zariffa J. Automated Hand Prehension Assessment from Egocentric Video after SCI. IEEE Trans Neural Syst Rehabil Eng. 2024. [PMID: 39102325]
- Roberts & Hedges' Clinical Procedures in Emergency Medicine. Hand Splinting Chapter (Position of Function).
- Physio-pedia: Grip Strength (evidence-based review, 2024 update).
QUESTION 4
Explain the Principles of Hand Splinting (10 Marks)
INTRODUCTION
CLASSIFICATION OF HAND SPLINTS
By Mechanism:
| Type | Description | Example |
|---|---|---|
| Static | No moving parts; immobilizes completely | Volar forearm splint post-fracture |
| Static progressive | Fixed at end-range; adjusted as motion improves | Serial casting for burn contracture |
| Dynamic | Spring-loaded components; apply force while permitting motion | Dynamic extension splint post-extensor repair |
| Relative motion | Positions injured digit relative to adjacent digits | Zones V-VI extensor tendon repair |
By Functional Purpose:
- Immobilization splints: Protect healing structures
- Mobilization splints: Correct contracture (low-load prolonged stretch)
- Restriction splints: Limit a range to protect (e.g., block flexion after tendon repair)
- Torque transmission splints: Transmit joint torque (e.g., flexion gloves)
- Functional splints: Replace lost motor function (tenodesis splint for C6 SCI)
PRINCIPLES OF HAND SPLINTING
PRINCIPLE 1: BIOMECHANICAL EFFICIENCY (Mechanical Principles)
- Pressure = Force / Area
- To minimize skin breakdown, the splint must distribute applied forces over the maximum possible surface area
- Splints should be wide, well-padded, and conform to bony contours
- Narrow splints create high-pressure points causing ischemia and necrosis
- Longer lever arms generate greater corrective torques with less force
- A forearm-based splint provides a longer lever arm than a hand-based splint - used for more powerful corrections
- The moment arm of the splint strap relative to the joint determines the effectiveness of correction
- Dynamic force should be applied perpendicular to the bone segment (90° angle of pull) for maximum rotational torque and minimum compressive or distractive joint force
- An angle of pull deviating from 90° creates undesirable joint compression or distraction in addition to rotation
- As motion improves, the point of attachment must be repositioned to maintain 90° pull
PRINCIPLE 2: TISSUE PHYSIOLOGY AND LOW-LOAD PROLONGED STRETCH (LLPS)
- High-load brief stretch (manual therapy, vigorous exercise): produces elastic deformation only - tissue returns to original length when force is removed
- Low-load prolonged stretch (splinting maintained for hours): produces plastic/creep deformation - permanent elongation of shortened structures
- Force: Low (sub-pain threshold, typically 100-300 g for most digital joints)
- Duration: Minimum 6-8 hours of wear per day for contracture correction; ideally 8-12 hours (worn at night and during rest)
- Frequency: Daily progressive adjustment as range improves
PRINCIPLE 3: JOINT PROTECTION AND ANTI-DEFORMITY POSITIONING
- Wrist: 20-30° extension (prevents flexion contracture; optimizes tenodesis and extrinsic tendon tension)
- MCPJs: 70-90° flexion (tenses collateral ligaments at their maximal length - prevents collateral shortening)
- IPJs: 0° extension (full extension - prevents FDS/FDP contracture)
- Thumb: Palmar abduction (prevents first web space adduction contracture)
- Short-term (7-14 days): "Position of function" (wrist 10-20° extension, MCPs 50-60° flexion, IPs slight flexion) - acceptable
- Long-term (>2 weeks): "Intrinsic plus/safe position" (MCPs 90° flexion, IPs in full extension) - mandatory to prevent intrinsic tightness and capsular contracture
PRINCIPLE 4: PROTECTION OF HEALING STRUCTURES
- Too little stress: Adhesion formation, tendon atrophy, joint stiffness
- Too much stress: Tendon rupture, malunion, ligament re-injury
PRINCIPLE 5: CORRECT FORCE APPLICATION AND SPLINT DESIGN
- Radial and ulnar styloids
- Lateral epicondyle
- Dorsum of MCP joints
- Base of thumb
- Do not compress the superficial branch of radial nerve (dorsoradial forearm)
- Do not compress the ulnar nerve at the Guyon's canal (ulnar wrist)
- Do not compress the median nerve at the wrist (carpal tunnel)
- Forearm trough should extend to the proximal 2/3 of the forearm (not beyond the elbow)
- Too short = insufficient lever arm; too long = restricts elbow motion unnecessarily
- Low-temperature thermoplastics (e.g., Orfit, Aquaplast): Most common for hand rehabilitation; self-moldable at 60-70°C, lightweight, perforated for ventilation
- Plaster of Paris: For emergency and acute fracture situations (heavier, less customizable)
- Fiberglass casting tape: For pediatric and high-compliance situations
- Neoprene / soft splints: For mild support, sensory awareness, mild joint hypermobility
PRINCIPLE 6: PATIENT EDUCATION AND COMPLIANCE
- Wearing schedule: The physiotherapist must prescribe a specific wearing schedule (not just "wear when needed")
- Skin checks: Patient instructed to check for skin redness, numbness, tingling every 2 hours
- Donning/doffing: Patient and caregiver must demonstrate correct application
- Hygiene: Splint cleaned daily; skin inspected for maceration between fingers
- Compliance is the #1 determinant of outcome - a technically perfect splint worn for 2 hours/day is less effective than a simpler splint worn 10 hours/day
PRINCIPLE 7: SPLINTING MUST COMPLEMENT EXERCISE - NOT REPLACE IT
- Splints are worn between exercise sessions, not instead of therapy
- The goal of immobilization splints is to provide a resting environment for healing; active exercises are performed at prescribed intervals with the splint removed
- Mobilization splints are worn during rest periods; active exercise is essential during waking hours
- Early active motion protocols (post-tendon repair, post-fracture) are the current evidence-based standard - they produce better outcomes than prolonged immobilization
PRINCIPLE 8: PROGRESSIVE MODIFICATION (SPLINT WEANING)
- As healing progresses, splints must be progressively modified to allow increasing range of motion
- Splint weaning schedule: typically begun at 6-8 weeks post-injury
- Failure to wean splints leads to dependency, muscle atrophy, and perpetuation of joint stiffness
- The splint is a temporary therapeutic device - not a long-term orthosis
SUMMARY TABLE: PRINCIPLES OF HAND SPLINTING
| Principle | Key Point |
|---|---|
| Three-point pressure | Mechanical corrective force without excess skin pressure |
| LLPS (Low-Load Prolonged Stretch) | Plastic deformation of contracted tissues |
| Anti-deformity positioning | MCPs 70-90° flexion; IPs 0°; wrist 20-30° extension |
| Tissue protection | Safe window of stress; prevent adhesion without rupture |
| Bony prominence padding | Avoid pressure ulcers and nerve compression |
| Patient education | Wearing schedule, skin checks, compliance |
| Complement exercise | Splints do not replace active therapy |
| Progressive weaning | Gradual reduction as healing progresses |
RECENT ADVANCES
-
Relative Motion Orthoses (RMO): Now standard of care for zones V-VI extensor tendon repairs. The injured digit's MCPJ is positioned 15-20° more extended than adjacent digits, reducing tendon excursion demands at the repair site while allowing full hand use. RCT evidence (Buhler et al. 2023, PMID: 37045642; Cela-Lopez et al. 2026, PMID: 41761624) confirms non-inferiority or superiority over dynamic extension splinting.
-
3D-Printed Custom Orthoses: Additive manufacturing now allows patient-specific, anatomically precise orthoses generated from 3D scans. Studies show equivalent or superior compliance compared to traditional thermoplastic splints, with better fit and less skin breakdown.
-
Smart / Sensor-Embedded Splints: Wearable splints with embedded pressure and motion sensors provide real-time feedback on wearing time, joint angles achieved, and force applied - addressing compliance monitoring and dose-response relationships.
-
Neoprene and Soft Splints for Hypermobility: Systematic review evidence supports the use of neoprene thumb CMC joint stabilization splints for osteoarthritis and hypermobility - equivalent pain relief with better compliance than rigid splints.
-
Telerehabilitation and Remote Splint Monitoring: Following the COVID-19 pandemic, hand therapy via telehealth with remote splint fabrication guidance has proven feasible with comparable outcomes (Seven et al., J Hand Ther 2024, PMID: 38307736).
REFERENCES
- Napier JR. The prehensile movements of the human hand. J Bone Joint Surg Br. 1956;38(4):902-913.
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, 7th Ed. Hand Splinting - Position of Function. Chapter 50.
- Miller's Review of Orthopaedics, 9th Edition. Wrist-Hand Orthosis Section.
- Buhler M, et al. Relative motion extension orthoses vs. dynamic extension orthoses for zones V-VI: RCT. J Hand Ther. 2023. [PMID: 37045642]
- Cela-Lopez M, et al. Relative Motion Extension Orthosis vs Classic Immobilization, Zones IV-VI: RCT. Hand (N Y). 2026. [PMID: 41761624]
- Newington L, et al. Relative motion flexion splinting for flexor tendon repairs: Systematic Review. Hand Ther. 2021. [PMID: 37904882]
- Tomkinson GR, et al. International norms for adult handgrip strength: Systematic review of 2.4 million adults. J Sport Health Sci. 2025. [PMID: 39647778]
- Seven B, et al. Telerehabilitation in patients with hand injury. J Hand Ther. 2024. [PMID: 38307736]
- Kaunnil A, et al. Hand-splinting practice: perspectives of occupational therapists. IJERPH. 2022. [PMID: 35897366]
EXAMINER TIPS (MPT Topper Insight)
- Start with Napier's classification (it shows depth)
- Enumerate systematically: Power grips (4 types) → Precision grips (5 types) → Developmental sequence
- Add muscle-nerve supply table - shows integration of anatomy
- For evaluation: use Jamar Dynamometer - describe the full ASHT protocol with 5 points (position, trials, hands, mean calculation, interpretation)
- Mention recent normative data (Tomkinson 2025) and GRASP taxonomy as advances
- Use a numbered principles format with subheadings - examiners can award marks clearly
- The biomechanical principles (3-point pressure, LLPS, angle of pull) differentiate MPT answers from BPT
- Anti-deformity positioning table is essential
- Connect every principle to a clinical consequence of violation (e.g., "failing to flex MCPs to 90° causes collateral ligament contracture")
- End with recent advances: 3D printing, RMO, sensor-embedded splints
5. Explain the principles of extensor tendon injury management. 10 M(Summer 2020) 6. Physiotherapy management for flexor tendon injury. 10 M(Winter 2018) MPT level Topper answer with references & recent advances
flexor tendon repair rehabilitation early active mobilization protocol
extensor tendon zone management splinting outcomes
flexor tendon zone II repair suture technique outcomes
extensor tendon injury rehabilitation relative motion splint
flexor tendon healing biology tendon repair principles
flexor tendon repair zone II controlled active motion outcome functional
WALANT wide awake local anesthesia flexor tendon repair rehabilitation
flexor tendon injury zones rehabilitation protocols Kleinert Duran Belfast place hold controlled active motion 2023 2024
Tang JB extensor tendon new classification strong repair
https://asht.org/sites/asht/files/images/International/Sept%…
flexor tendon rehabilitation cochrane systematic review
MPT-Level Answers: MUHS Summer 2020 / Winter 2018
QUESTION 5
Explain the Principles of Extensor Tendon Injury Management (10 Marks)
INTRODUCTION
PRINCIPLE 1: THOROUGH UNDERSTANDING OF THE ZONE-BASED ANATOMY
| Zone | Location | Key Structure | Injury Pattern |
|---|---|---|---|
| I | DIP joint / distal phalanx | Terminal tendon | Mallet finger |
| II | Middle phalanx | Lateral bands / triangular ligament | Dorsal laceration |
| III | PIP joint | Central slip | Boutonniere deformity |
| IV | Proximal phalanx | EDC over P1 | Adhesion-prone; causes extension lag |
| V | MCP joint | Sagittal bands / EDC | Tendon subluxation; fight bites |
| VI | Metacarpal | EDC, juncturae tendinum | Most common zone injured |
| VII | Extensor retinaculum | All finger + wrist extensors | Synovial adhesions, retraction |
| VIII | Distal forearm (MJT) | Musculotendinous junction | Poor suture purchase |
| IX | Proximal forearm | Muscle bellies | Suboptimal repair outcomes |
- Distal zones (I-III): only 1-2 mm of normal excursion - immobilization is imperative, not motion
- Middle zones (IV-V): prone to adhesion formation with immobilization; early motion protocols indicated
- Proximal zones (VI-VII): 5 mm excursion required; early active motion essential to prevent adhesions within the retinaculum
PRINCIPLE 2: RESTORATION OF THE EXTENSOR HOOD MECHANISM
Deformity 1: Mallet Finger (Zone I)
- Closed/tendinous mallet: Stack splint or custom thermoplastic DIPJ extension splint for 6-8 weeks continuous (100% compliance mandatory - even a single episode of DIPJ flexion restarts the healing clock)
- Bony mallet without subluxation: extension splinting until fracture union (~6-8 weeks)
- Bony mallet with >50% articular surface or volar subluxation of P3: operative fixation (CRPP or extension block pinning)
- After immobilization: night splinting for additional 4-6 weeks; progressive DIPJ active flexion exercises
Deformity 2: Boutonniere Deformity (Zone III)
- Acute closed boutonniere: Full-time PIPJ extension splinting for 6 weeks with simultaneous active DIPJ flexion maintained (biomechanical rationale: active DIPJ flexion draws the lateral bands dorsally, restoring the balance of the extensor mechanism and encouraging the oblique retinacular ligament to adopt a dorsal orientation)
- Part-time splinting for additional 4-6 weeks
- Elson's test must be used to diagnose central slip injury: PIPJ flexed 90° over edge of table - if central slip intact, DIP remains supple; if ruptured, DIP becomes rigid as extensor power is diverted to lateral bands
Deformity 3: Swan-Neck Deformity
- Supple swan-neck: Fowler central slip tenotomy or SORL (spiral oblique retinacular ligament) reconstruction
- Established rigid deformity: dynamic splinting first to restore passive motion, then operative correction
PRINCIPLE 3: REPAIR TECHNIQUE BASED ON ZONE AND TENDON THICKNESS
- Tendons too thin for core sutures
- Figure-of-eight, running, or cross-stitch sutures sufficient
- Suture caliber: 4-0 to 5-0 non-absorbable (polypropylene / nylon)
- Tendons thicker; accommodate 2-4 core strand repairs
- Core suture + epitendinous suture recommended (epitendinous repair adds ~10-20% to overall repair strength)
- Suture caliber: 3-0 to 4-0 for core sutures
- Thorough wound washout and debridement (especially fight bites - zone V)
- Adequate haemostasis before repair
- Avoid over-tightening (causes finger extension deficit, loss of composite flexion)
- Lacerations >50% of tendon width must be repaired; <50% may be managed with early active motion without formal repair
- Zone VII: counterincision in forearm often needed to retrieve retracted proximal stump
PRINCIPLE 4: ZONE-SPECIFIC PHYSIOTHERAPY REHABILITATION PROTOCOL
- Immobilization (needed in distal zones I-III where excursion is minimal and gap formation must be prevented)
- Early motion (mandatory in zones IV-VII where adhesions form rapidly and tendon excursion demands are higher)
Early Mobilization Protocols - Physiotherapy Rationale
- DIPJ static extension splinting × 6-8 weeks
- No motion of DIPJ during healing phase
- PIPJ active ROM preserved throughout
- Initiated 24-48 hours post-repair
- Week 1-2: Active PIPJ 0-30° motion range
- Week 3-4: Progressively increase to 0-50°
- Dynamic PIPJ extension splints may be used as an alternative
- Rationale: 3-4 mm of tendon excursion sufficient to prevent adhesion; SAM preserves PIP flexion without endangering the central slip repair
- Dynamic extension splint: Wrist at 45° extension, MCPs neutral with volar block permitting 30-40° MCP flexion; rubber band traction passively extends digits. Started 1-3 days post-repair.
- Active flexion (against the rubber band) creates 3-5 mm of controlled tendon glide
- Active motion added at 3-4 weeks; resistance added at 7 weeks
- Relative Motion Splinting (RMS): Positions repaired digit's MCPJ in 15-20° more extension than adjacent digits - reduces extensor tendon excursion demands at the repair site while permitting full functional hand use. Current evidence-based first-line option (Buhler et al. 2023, PMID: 37045642)
- Synovial lining makes this zone uniquely prone to adhesion formation
- Early active motion within the retinaculum is essential (splint wrist in mild extension; early active motion program)
- Counterincision to retrieve tendon ends; repair with 3-0 core + epitendinous suture
PRINCIPLE 5: PREVENTION AND MANAGEMENT OF COMPLICATIONS
| Complication | Zone | Prevention |
|---|---|---|
| Swan-neck | I | Continuous DIP extension splinting × 6-8 weeks; patient education on compliance |
| Boutonniere | III | PIPJ extension splinting + active DIP flexion; Elson test for diagnosis |
| Tendon rupture | V-VII | Staged resistance; patient education; avoid passive wrist flexion + active grip |
| Adhesions | IV-VII | Early motion protocols; scar management |
| Extension lag | IV-VI | Dynamic splinting; active extension exercises |
| MCP subluxation | V | Careful sagittal band repair; splint MCPs in extension (exception to intrinsic-plus rule) |
| Skin ulceration | I-II | Stack splint not in hyperextension; skin checks every 2 hours |
PRINCIPLE 6: PATIENT COMPLIANCE IS THE PARAMOUNT PRINCIPLE
- Compliance with splint wear is the single greatest determinant of outcome
- Zone I mallet finger: one single event of DIPJ flexion during the 6-week period restarts the healing clock entirely
- Patient must receive written and verbal education on: splint wearing schedule, donning/doffing, skin inspection, what activities to avoid
PRINCIPLE 7: OUTCOME MEASUREMENT
- TAM% = [(Active PIP flexion + Active DIP flexion) - (PIP + DIP extension lag)] ÷ 175 × 100
- Excellent: 85-100%; Good: 70-84%; Fair: 50-69%; Poor: <50%
- Used for zones I-IV extensor tendon injuries
RECENT ADVANCES (Critical for MPT)
-
Relative Motion Splinting (RMS) as First-Line (2023-2026):
- RCT by Buhler et al. 2023 (PMID: 37045642): RMS non-inferior to dynamic extension splinting for zones V-VI, with better cost-effectiveness and patient satisfaction
- RCT by Cela-Lopez et al. 2026 (PMID: 41761624): RMS superior to classic immobilization for zones IV-VI in return of TAM and grip strength
- Relative motion flexion splinting extended to flexor tendon repairs (Newington et al., systematic review 2021, PMID: 37904882)
-
Novel Tang JB Classification (2025, PMID: 41025781): Proposes simplified 8-zone system with emphasis on strong repairs (multi-strand core sutures even for extensor tendons) allowing true active motion rather than passively assisted motion post-repair. Challenges the historical view that extensor repairs are "simpler" than flexor repairs.
-
Novel repair approaches (Tang & Lalonde 2026, PMID: 41537406): Achieving balance in tendon repair - using intraoperative active flexion under WALANT anesthesia to verify that repair does not impede full digit flexion, guiding rehabilitation protocols.
-
Strong Extensor Tendon Repairs (Tang JB 2025, PMID: 41016635): Applying flexor tendon repair principles (4-strand core suture, epitendinous suture) to extensor tendon zones V-VIII allows true active motion within days of repair - previously not possible with weaker suture techniques.
REFERENCES
- Miller's Review of Orthopaedics, 9th Ed. Extensor Tendon Injury Zones and Management.
- Sabiston Textbook of Surgery, 21st Ed. Chapter 119: Extensor Tendon Injuries.
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, 7th Ed. Chapter 48: Post-repair Care and Rehabilitation.
- ASHT: Rehabilitation of flexor and extensor tendon injuries in the hand. Hand Ther. 2023 (ASHT International, Sept 2023).
- Buhler M, et al. Relative motion extension orthoses vs dynamic extension orthoses, zones V-VI: RCT. J Hand Ther. 2023. [PMID: 37045642]
- Cela-Lopez M, et al. Relative Motion Extension Orthosis vs Classic Immobilization, Zones IV-VI: RCT. Hand (N Y). 2026. [PMID: 41761624]
- Tang JB. Extensor tendon injuries: a new classification, strong repairs, and easier therapy. Plast Reconstr Surg. 2025. [PMID: 41025781]
- Tang JB & Lalonde D. Achieving balance in tendon repair. J Hand Surg Eur Vol. 2026. [PMID: 41537406]
- Arvind V, et al. Extensor Tendon Repair. JBJS Essent Surg Tech. 2024. [PMID: 39440273]
QUESTION 6
Physiotherapy Management for Flexor Tendon Injury (10 Marks)
INTRODUCTION
PART A: ANATOMY AND ZONES OF FLEXOR TENDON INJURY
| Zone | Location | Key Feature |
|---|---|---|
| I | Tip to FDS insertion (middle of middle phalanx) | FDP alone; "Jersey finger" (avulsion from distal phalanx) |
| II | FDS insertion to distal palmar crease | "No Man's Land" - both FDS + FDP in tight sheath; highest adhesion risk |
| III | Distal palmar crease to carpal tunnel distal edge | Lumbrical origin zone |
| IV | Within the carpal tunnel | Median nerve + 9 tendons; iatrogenic bowstringing risk |
| V | Proximal to carpal tunnel | Forearm; favorable prognosis; "spaghetti wrist" injuries |
- Both FDS and FDP run within a single tight fibro-osseous sheath
- A2 and A4 pulleys (the most biomechanically critical) are here
- The tendon-sheath interface promotes adhesion formation
- The tendon receives nutrition by diffusion (not vascularization) in this region
- Repair tension must be precise to prevent bowstringing (if pulleys damaged) or restricted flexion (if repair too tight)
PART B: BIOLOGY OF TENDON HEALING - THE PHYSIOLOGICAL BASIS
| Phase | Timing | Biology | PT Implication |
|---|---|---|---|
| Inflammatory | 0-5 days | Neutrophil/macrophage infiltration; weak repair | Protect; no active loading |
| Proliferative | Day 5 - 3 weeks | Fibroblast collagen deposition (initially Type III); adhesion formation risk highest | Controlled tendon excursion prevents adhesions; early motion begins |
| Remodelling | 3 weeks - 6+ months | Type III → Type I collagen; repair strength increases to ~60% at 6 weeks | Progressive loading; strengthen |
- Extrinsic healing: From surrounding tissues; produces adhesions (functionally problematic)
- Intrinsic healing: From the tendon itself (diffusion-based, nutrition via synovial fluid); produces organized collagen without adhesions
PART C: SURGICAL REPAIR PRINCIPLES (Context for PT Management)
- 4-strand core suture minimum (e.g., modified Kessler, Adelaide, four-strand cruciate) - required for early active motion protocols; 2-strand repair insufficient
- Epitendinous suture - adds 10-50% to repair strength; allows earlier active motion
- A2 and A4 pulley preservation - mandatory to prevent bowstringing; loss increases work of flexion
- Tendon purchase distance: 0.7-1.2 cm from tendon end; dorsally placed sutures stronger than volar
- Timing: Primary repair within 12-24 hours preferred; delayed primary repair up to 7-10 days acceptable
PART D: PHYSIOTHERAPY REHABILITATION - ZONE-SPECIFIC PHASE-BASED PROTOCOL
Phase I: Protective Phase (Days 3-5 to Week 3)
- Zones I-III: Wrist 20-30° extension; MCPs 30-40° flexion; IPs at 0°
- Zones IV-V: Wrist 0° neutral; MCPs 60-75° flexion; IPs at 0°
- Duration: Worn continuously for 6 weeks (removed only for supervised exercises)
- Pulley ring orthosis if pulley was repaired
1. Passive Mobilization - Modified Duran Protocol (Conservative - for 2-strand repairs or non-compliant patients)
- Initiated: Day 3-5 post-surgery
- Technique: Passive digital flexion followed by active extension within the splint
- Passive DIPJ flexion + active extension to splint (10 reps × hourly)
- Passive PIPJ flexion + active extension to splint
- Passive composite flexion + active extension to splint
- Rationale: 3-5 mm of passive tendon excursion sufficient to prevent adhesion maturation without loading the repair
- Limitation: Insufficient glide to prevent all adhesions; less functional than active protocols
2. Place-and-Hold (Modified Kleinert) - Semi-Active Protocol (for compliant patients with robust repair)
- Initiated: Day 4-5 post-surgery
- Technique:
- Passively place digit in full composite flexion (all joints)
- Ask patient to actively hold this position (FDP contracts isometrically to maintain position)
- Actively extend digits to neutral within splint
- No active against-resistance flexion
- Rationale: Isometric tendon contraction in the shortened position produces 3-5 mm of tendon excursion with minimal tensile loading of the repair. Produces better glide than pure passive protocols.
- Requirement: Minimum 4-strand core suture repair
3. Controlled Active Motion (CAM) - True Active Protocol (for highly compliant patients with strong repairs)
- Initiated: Day 3-5 post-surgery (requires intraoperative verification that active flexion is full without impingement - increasingly done with WALANT)
- Technique:
- Passive digital composite flexion
- Active digit flexion starting at ~25% of full range, progressively increasing
- Active extension to neutral within splint
- Blocking exercises: stabilize MCP and actively flex IP joints (maximizes FDP differential glide)
- Rationale: Active tendon contraction produces greatest tendon excursion (8-10 mm), most effectively prevents adhesions, and provides the strongest stimulation for intrinsic tendon healing
- Risk: Highest rupture risk if repair is insufficient (<4 strands) or patient unreliable
- Evidence: RCT (Ahmed et al., J Hand Ther 2025, PMID: 40090773) confirmed controlled active motion superior to early passive mobilization in achieving TAM in zone II repairs at 12 weeks
Phase II: Active Motion Phase (Weeks 3-6)
- Discontinue rubber band if modified Kleinert used
- Begin true active composite flexion exercises (hook fist, full fist, tabletop, straight fist positions)
- Tendon gliding exercises - critical for differential glide:
- Hook fist: MCPs extended, IPs fully flexed - maximizes FDP glide over FDS
- Full fist: All joints fully flexed
- Tabletop: MCPs flexed, IPs extended - maximizes FDS glide over FDP
- Straight fist: MCPs flexed, IPs extended at DIP - produces FDS differential glide
- Progressive wrist active ROM introduced at week 3
- Scar management: silicone gel, massage, compression
- Extension deficit monitoring: if PIPJ extension lag developing, commence night extension splinting at week 6
Phase III: Strengthening Phase (Weeks 6-12)
- Progressive resistance: putty (Theraputty), finger ladder, spring clips
- Grip strength measured with Jamar dynamometer; target 60-70% of contralateral by week 8
- Light functional activities without resistance from week 6
- Work hardening / vocational training from week 10
- Full return to activities including heavy loading by week 10-12
Phase IV: Return to Sport / Heavy Work (Weeks 10-16)
- Sport-specific and work-specific conditioning
- Reassessment with TAM (Strickland's formula) and grip dynamometry
- Functional outcome measures: DASH (Disabilities of Arm, Shoulder and Hand) questionnaire
PART E: ZONE-SPECIFIC MODIFICATIONS
| Zone | Specific Considerations |
|---|---|
| Zone I | FDP repair only; focus on active DIPJ flexion; risk of cross-adhesion with FDS and fixed flexion deformity; "jersey finger" avulsion requires surgical reattachment within 7-10 days |
| Zone II | "No Man's Land" - highest risk; 4-strand minimum + epitendinous suture mandatory for active protocols; differential tendon gliding exercises critical |
| Zone III | Lumbrical muscle adjacent; splint position: wrist 10-30° extension; MCP 30° flexion if no nerve injury; mobilize freely in absence of nerve injury |
| Zone IV | Carpal tunnel contents; bowstringing risk if pulleys disrupted; splint wrist at neutral; no passive wrist extension >0° if nerve repair present (for 6 weeks) |
| Zone V | Best prognosis; active protocols used from early; "spaghetti wrist" requires careful matching of all structures |
PART F: OUTCOME MEASUREMENT
- TAM% = [(Active PIP + DIP flexion) - (PIP + DIP extension lag)] ÷ 175 × 100
- Excellent: 85-100%; Good: 70-84%; Fair: 50-69%; Poor: <50%
- Rupture (most serious - typically days 7-21 of early motion; sudden loss of active flexion)
- Adhesions (poor TAM despite full passive ROM)
- Bowstringing (loss of A2/A4 pulley function; painful with active flexion)
- Quadrigia effect (over-advancement of one FDP limits flexion of adjacent digits)
- Lumbrical plus finger (paradoxical extension on flexion - lumbrical tight from proximal advancement)
RECENT ADVANCES (Critical for MPT)
-
WALANT (Wide Awake Local Anesthesia No Tourniquet) Surgery:
- Allows intraoperative active tendon gliding under local anesthesia + adrenaline
- Surgeon can verify completeness of repair, absence of impingement, and that the patient can achieve full active flexion before closing
- Directly personalizes the post-operative rehabilitation protocol
- RCT by El-Gammal et al. (J Hand Surg Am 2024, PMID: 39115486): WALANT zone II repair produces equivalent outcomes to general anesthesia with lower cost and better patient compliance with early active motion
- 2025 study (Emir et al., J Hand Surg Eur Vol, PMID: 39883802): WALANT + controlled true active motion in delayed primary zone II repair - excellent outcomes
-
Systematic Review - Zone II Evidence-Based Management (Douwes et al., Hand Surg Rehabil 2025, PMID: 40769262):
- Confirms multi-strand core suture + early active motion superior to passive protocols
- Supports CAM as preferred protocol in compliant patients with strong repairs
-
Controlled Active Motion vs. Place-and-Hold RCT (Ahmed et al. 2025, PMID: 40090773):
- CAM produced significantly better TAM than place-and-hold in zone II at 12 weeks
- No significant difference in rupture rates when repair was 4-strand minimum
-
Relative Motion Flexion Splinting (RMFS) for Flexor Tendons:
- Newington et al. systematic review (Hand Ther 2021, PMID: 37904882) and clinical application paper (J Hand Ther 2023, PMID: 37029053): RMFS positions the repaired digit's MCPJ in slight flexion relative to adjacent digits, reducing FDP/FDS tension at the repair site while allowing functional use
- Extends the relative motion splinting paradigm from extensor to flexor tendon rehabilitation
-
General Principles Update (Jo & Calfee, Hand Clin 2023, PMID: 37080645; Miller & Teal, Clin Plast Surg 2024, PMID: 39216932):
- Confirms that predictable outcomes require: strong multi-strand repair + skilled hand therapy + patient compliance - all three components equally essential
-
Telerehabilitation for Flexor Tendon Injuries:
- Post-pandemic evidence supports video-guided rehabilitation as adjunct (not replacement) for in-person hand therapy for monitoring compliance and exercise technique
SUMMARY TABLE: PT MANAGEMENT PROTOCOLS
| Protocol | Timing Start | Active Component | Indication | Risk |
|---|---|---|---|---|
| Modified Duran (passive) | Day 3-5 | None (passive only) | Vulnerable repair; unreliable patient | Adhesions |
| Place-and-Hold | Day 4-5 | Isometric hold | Moderate repair; reliable patient | Moderate rupture |
| Controlled Active Motion | Day 3-5 | True active flexion | 4-strand+ repair; highly compliant | Higher rupture risk |
| Immobilization (cast) | Day 0 | None | Children <7 years; severe non-compliance | High adhesion risk |
REFERENCES
- Miller's Review of Orthopaedics, 9th Ed. Principles of Flexor Tendon Repair.
- Sabiston Textbook of Surgery, 21st Ed. Chapter 119 (Flexor Tendon Injuries - Nerve Injuries).
- ASHT International. Rehabilitation of Flexor and Extensor Tendon Injuries in the Hand. Hand Ther. Sept 2023.
- University of Virginia Orthopaedic Surgery. Flexor Tendon Repairs Zones I-IV Early Active (Place and Hold) Motion Protocol. 2024.
- Douwes TA, et al. Flexor tendon repair in zone II: Evidence-based management. Hand Surg Rehabil. 2025. [PMID: 40769262]
- Ahmed E, et al. RCT comparing controlled active motion vs. passive mobilization for zone II FT repair. J Hand Ther. 2025. [PMID: 40090773]
- Jo S & Calfee RP. General Principles of Flexor Tendon Repair. Hand Clin. 2023. [PMID: 37080645]
- Miller EA & Teal L. Principles for Achieving Predictable Outcomes in Flexor Tendon Repair. Clin Plast Surg. 2024. [PMID: 39216932]
- El-Gammal TA, et al. Zone II Repair Under WALANT vs General Anesthesia: RCT. J Hand Surg Am. 2024. [PMID: 39115486]
- Emir Z, et al. Delayed primary FT repair in zone II using WALANT and controlled active motion. J Hand Surg Eur Vol. 2025. [PMID: 39883802]
- Newington L, et al. Relative motion flexion splinting for flexor tendon repairs: Systematic Review. Hand Ther. 2021. [PMID: 37904882]
- Newington L, et al. Relative motion flexion following zone I-III FT repair: concepts, evidence and practice. J Hand Ther. 2023. [PMID: 37029053]
- Chevalley S, et al. Passive mobilization vs active motion therapy after FT repair: RCT. J Hand Surg Am. 2022. [PMID: 35190217]
EXAMINER TIPS (MPT Topper Insight)
- Open with the "deceptive simplicity" - examiners appreciate the awareness that these are difficult
- Present all 7 principles in clear numbered format - each principle must have its biomechanical rationale stated
- Zone table + Deformity pathomechanics table = high marks
- RMS as current evidence-based standard (Buhler 2023, Cela-Lopez 2026) + Tang JB strong repair concept (2025) = recent advance marks
- "No Man's Land" (Zone II) biology should anchor the answer - it explains WHY the protocols are designed as they are
- Three main rehabilitation protocols (Duran, Place-and-Hold, CAM) must be distinguished clearly with their indications
- The 3-phase timeline (inflammatory/proliferative/remodelling) + biology table earns high marks at MPT level
- End with WALANT + evidence-based superiority of CAM (Douwes 2025, Ahmed 2025) = full marks for advances
1. Explain how biomechanics of hip joint will influence clinical decision making and treatment. 20 M(Summer 2023) 2. Explain in brief biomechanics of hip joint and hip abductor mechanism. 20 M(Summer 2021) 3. Describe the pathomechanics and management of hip dysfunction in geriatric population. 30M MPT level Topper answer with reference books and recent advances
hip biomechanics clinical decision making rehabilitation
hip dysfunction geriatric population pathomechanics physiotherapy management
hip osteoarthritis exercise therapy elderly systematic review
hip abductor strength Trendelenburg gait rehabilitation
hip fracture elderly rehabilitation falls prevention
resistance exercise hip osteoarthritis pain function meta-analysis
hip osteoarthritis physical therapy exercise pain function older adults
hip joint biomechanics Pauwels lever arm abductor mechanism clinical implications physiotherapy MPT level
total hip replacement versus resistance exercise severe hip osteoarthritis
hip osteoarthritis geriatric pathomechanics physiotherapy management 2024 guidelines OARSI NICE
progressive resistance training neuromuscular exercise hip osteoarthritis multicenter RCT
MPT-Level Answers: MUHS Hip Biomechanics & Geriatric Hip Dysfunction
QUESTION 1 & 2 (COMBINED)
Biomechanics of the Hip Joint, Hip Abductor Mechanism, and Clinical Decision Making
(20M Summer 2023 + 20M Summer 2021)
INTRODUCTION
PART A: ANATOMY OF THE HIP JOINT - BIOMECHANICAL FRAMEWORK
Osseous Architecture
| Axis | Plane | Movement | Normal Range |
|---|---|---|---|
| Transverse | Sagittal | Flexion / Extension | 120-140° / 0-20° |
| Sagittal | Frontal | Abduction / Adduction | 40-45° / 20-30° |
| Longitudinal | Horizontal | Internal / External rotation | 30-40° / 40-60° |
- Neck-shaft (cervicodiaphyseal) angle: Normal 125-135°. Coxa valga (>135°) shortens abductor lever arm; coxa vara (<120°) lengthens it
- Femoral anteversion: Normal 10-15°. Excessive anteversion causes in-toeing gait and altered hip muscle moment arms
- Acetabular inclination (CE angle of Wiberg): Normal 25-35°. Reduced = dysplasia; increased = impingement
- Femoral offset: Perpendicular distance from center of femoral head to femoral shaft axis. Determines abductor moment arm length
Stabilizing Structures
- Iliofemoral ligament (Y-ligament of Bigelow): Strongest ligament in the body; resists extension and external rotation
- Pubofemoral ligament: Resists abduction and external rotation
- Ischiofemoral ligament: Resists internal rotation
- Acetabular labrum: Fibrocartilaginous rim that deepens the socket by ~21%; enhances stability, acts as a fluid seal improving joint lubrication and load distribution; damage → instability and pain
- Hip flexors (iliopsoas): anterior stabilization
- Hip abductors (gluteus medius, minimus, TFL): lateral pelvic stabilization
- Deep external rotators (piriformis, obturator, gemelli, quadratus femoris): posterior stabilization (analogous to rotator cuff of the hip)
PART B: HIP JOINT BIOMECHANICS - THE LEVER ARM MODEL
The Hip as a First-Class Lever
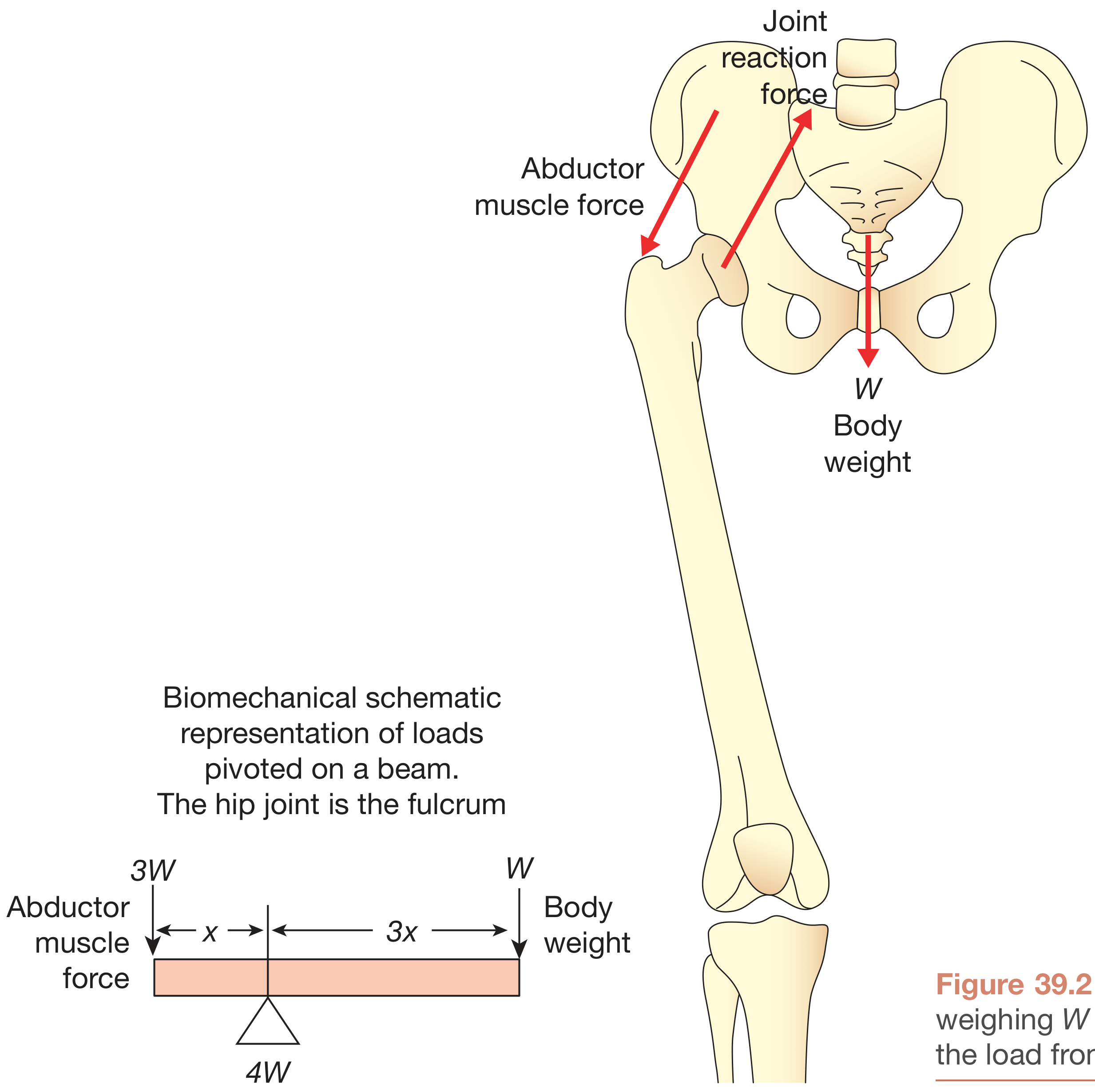
- Body Weight (W): Acts downward through the center of gravity (CoG), displaced medially from the hip center. Its moment arm "a" = distance from CoR to CoG vector (~8-10 cm from hip center)
- Abductor Muscle Force (M): Acts upward and medially from the greater trochanter. Its moment arm "b" = distance from CoR to greater trochanter (~5 cm from hip center)
- Joint Reaction Force (R): Acts upward through the femoral head
Hip Joint Reaction Forces at Different Activities
| Activity | Joint Reaction Force |
|---|---|
| Lying supine (straight leg raise) | 1.5 × Body Weight |
| Standing on one leg (single limb stance) | 3-4 × Body Weight |
| Walking (stance phase) | 2.5-3 × Body Weight |
| Jogging | 5-6 × Body Weight |
| Running | 8 × Body Weight |
| Hopping / Jumping | 8-10 × Body Weight |
PART C: THE HIP ABDUCTOR MECHANISM
Anatomical Components
- Gluteus medius (primary abductor - most important): originates from the outer surface of the ilium between the posterior and anterior gluteal lines; inserts into the greater trochanter. Particularly the anterior fibers are critical for pelvic stabilization in stance.
- Gluteus minimus: deep to medius; assists abduction and internal rotation
- Tensor fasciae latae (TFL): contributes via the iliotibial band
- Iliotibial band (ITB) - Pauwels' tension band: Functions as a lateral tension band, converting bending moments in the femoral neck into compressive forces (reduces femoral neck bending stress by up to 50%)
- Upper gluteus maximus fibers: accessory contribution
Biomechanical Function During Gait - Single Limb Stance
- The unsupported side of the pelvis tends to drop due to gravity (contralateral body weight moment)
- The hip abductors of the weight-bearing limb must contract forcefully to prevent pelvic drop
- They generate an external abduction torque equal and opposite to the gravitational torque of the body weight
The Trendelenburg Sign - Clinical Application of Abductor Biomechanics
- Ask the patient to stand on one limb
- Negative (normal): The contralateral pelvis remains level or rises slightly (gluteus medius of the stance limb holds pelvis level)
- Positive: Contralateral pelvis drops >2° (abductor weakness or pain inhibition)
- Gluteus medius weakness (superior gluteal nerve palsy, L4-L5 lesion)
- Pain inhibition (hip OA, bursitis - patient avoids loading)
- Short lever arm for abductors (coxa valga, reduced femoral offset)
- Developmental/structural: CDH, AVN with head collapse
- Patient shifts trunk toward the affected side during stance
- This shifts the CoG toward the hip center, reducing the body weight lever arm "a"
- Net effect: reduces the required abductor force and thus the joint reaction force
- Biomechanically protective but abnormal and energy-expensive
PART D: CLINICAL DECISION MAKING BASED ON HIP BIOMECHANICS
1. Weight Management and Joint Load Reduction
- The cane's ground reaction force creates an external abduction moment on the ipsilateral hip
- Reduces gluteus medius effort required for pelvic stability
- Can reduce hip JRF by 30-40% (up to 1-2× body weight)
- Contra: placing the cane in the ipsilateral hand (incorrect) is ineffective biomechanically
2. Exercise Prescription - Biomechanically Rational Selection
| Exercise | JRF | Abductor Load | Indication |
|---|---|---|---|
| Swimming / hydrotherapy | Very low (buoyancy) | Low | Acute flare, severe OA |
| Cycling (seated) | Low (~1.3BW) | Low | Moderate OA, endurance |
| Walking (level) | 2.5-3BW | Moderate | Maintenance, general conditioning |
| Stair climbing | 3-5BW | High | Avoided in moderate-severe OA |
| Running | 8BW | Very high | Contraindicated in OA |
- Strengthening abductors increases the abductor moment arm contribution relatively, reducing the JRF required for equivalent pelvic control
- Reduces Trendelenburg gait and associated energy cost
- Reduces pain via improved joint congruence
3. Total Hip Arthroplasty (THA) Design - Biomechanical Implications
| Surgical Decision | Biomechanical Rationale |
|---|---|
| Restore femoral offset | Increases abductor moment arm "b" → reduces abductor force required → reduces JRF; prevents Trendelenburg gait post-THA |
| Medialize acetabular component | Reduces body weight moment arm "a" → reduces JRF |
| Restore leg length | Equalizes lever arms; prevents pelvic tilt and compensatory gait |
| Cemented vs. cementless | Load transfer mechanism; modulus matching to prevent stress shielding |
| Head size | Larger head → greater range of motion but higher surface area friction |
4. Coxa Valga vs. Coxa Vara - Clinical Biomechanics
| Feature | Coxa Valga (angle >135°) | Coxa Vara (angle <120°) |
|---|---|---|
| Abductor lever arm "b" | Shorter | Longer |
| Required abductor force | Higher | Lower |
| JRF | Higher | Lower |
| Gait | Trendelenburg gait | Relatively better |
| OA risk | Higher | Lower |
| Clinical decision | Priority: abductor strengthening; avoid high-load activities | Generally better prognosis |
5. Femoral Neck Stress Fractures - Load Analysis
- Inferior (compressive) surface: Cortex undergoes compression - greater bone density here
- Superior (tensile) surface: Cortex undergoes tension - weaker; fractures initiate here
- The ITB (Pauwels) converts bending to compression; ITB dysfunction = increased tensile stress = fatigue fracture risk
6. Rehabilitation Post-Hip Surgery - Weight-Bearing Biomechanics
- Non-weight-bearing (NWB) / Toe-touch: Reduces JRF to ~1.5W; used immediately post-op
- Partial weight-bearing (PWB): Gradual progression; JRF ~2W
- Full weight-bearing: JRF 3-4W; commenced when bone healing or implant osseointegration allows
- No hip flexion >90°, adduction, or internal rotation
- Biomechanical basis: posterior capsule and external rotators (repaired at surgery) are under maximum tension in these positions - risk of dislocation
7. Gait Deviations - Biomechanical Analysis and PT Intervention
| Gait Deviation | Biomechanical Cause | Intervention |
|---|---|---|
| Trendelenburg (contralateral pelvic drop) | Gluteus medius weakness | Abductor strengthening; cane in contralateral hand |
| Antalgic gait (shortened stance phase) | Pain avoidance; reduced loading time | Pain management; aquatic therapy |
| Stiff-hip gait (reduced sagittal motion) | Hip flexor tightness / OA stiffness | Hip flexor stretching; Thomas test-guided ROM |
| Trunk lean toward affected side | Compensated Trendelenburg | Core and abductor strengthening |
| Hip hitching (pelvic elevation in swing) | Hip flexor weakness / shortening | Hip flexor stretching; gait retraining |
PART E: BIOMECHANICAL ASSESSMENT TOOLS
| Assessment | Biomechanical Parameter | Clinical Use |
|---|---|---|
| Trendelenburg test | Gluteus medius strength/function | Screen for abductor mechanism dysfunction |
| Thomas test | Hip flexor length / flexion contracture | Limb length discrepancy compensation; gait deviation source |
| Modified Thomas test | Iliotibial band length | Trochanteric bursitis, ITB syndrome |
| Ober's test | TFL/ITB tightness | Hip abductor mechanism dysfunction |
| FABER / FADIR | Labral pathology, FAI, OA | Joint pathology screening |
| 30-second Chair Stand Test | Lower limb power and function | Functional capacity in geriatric patients |
| Gait analysis (3D / instrumented) | JRF, abductor moment, pelvic kinematics | Research; complex gait deviation analysis |
QUESTION 3
Pathomechanics and Management of Hip Dysfunction in the Geriatric Population (30 Marks)
INTRODUCTION
PART A: AGE-RELATED CHANGES AFFECTING HIP BIOMECHANICS (Pathophysiological Basis)
1. Sarcopenia and Muscle Changes
- Progressive loss of skeletal muscle mass and strength with aging (sarcopenia): 1-2% muscle mass loss per year after age 50; up to 3-5% per decade in strength
- Gluteus medius and gluteus maximus are among the earliest and most severely affected hip muscles
- Result: Reduced abductor moment, Trendelenburg gait, increased JRF (paradoxically worsened by compensatory trunk lean)
- Hip muscle strength decreases by 20-40% between age 60-80 years
2. Osteoporosis and Bone Quality
- Bone mineral density (BMD) declines after age 35; accelerates in postmenopausal women (~3-5% per year in first 5 years post-menopause)
- Femoral neck, intertrochanteric region, and Ward's triangle are the critical regions of vulnerability
- The trabeculae of the femoral neck thin and reorient - the principal compressive and tensile trabeculae become sparse, reducing the ability of the bone to resist bending moments
- Singh Index (Grade I-VI) on AP pelvis X-ray grades trabecular loss severity
3. Articular Cartilage Degeneration - Hip Osteoarthritis (OA)
- Water content initially increases (failure of proteoglycan to retain water) → cartilage softening and reduced stiffness
- Collagen network disruption; chondrocytes attempt repair but cannot keep pace with degradation
- Proteoglycan (aggrecan) loss; matrix metalloprotease (MMP) upregulation
- Fibrillation and surface irregularity
- Increased coefficient of friction → cartilage wear under repeated loading
- Sub-chondral bone stress increase → microfractures, bone remodeling → sclerosis
- Joint space narrowing (superior, often superolateral in hip OA)
- Osteophyte formation (Wolff's Law response - bone remodels along stress lines)
- Femoral head deformity; loss of sphericity
- Capsular contracture → hip flexion-adduction-external rotation contracture
4. Reduced Proprioception and Neuromuscular Control
- Aging reduces the density and sensitivity of mechanoreceptors in joint capsule, ligaments, and muscle spindles
- Results in delayed muscle activation, impaired balance responses, increased fall risk
- Labral degeneration (common in elderly) further reduces proprioceptive input
5. Hip Flexion Contracture
- Age-related shortening of iliopsoas and rectus femoris (sitting posture dominant)
- Even 10° of fixed flexion contracture dramatically alters lower limb biomechanics:
- Increased anterior pelvic tilt
- Compensatory lumbar hyperlordosis
- Increased hip extensor moment demand during gait
- Reduced stride length and walking speed
PART B: COMMON HIP DYSFUNCTIONS IN THE ELDERLY
1. Hip Osteoarthritis (Most Common)
- Deep groin or anterior thigh pain; referred to knee (L3 pattern)
- Morning stiffness <30 minutes (distinguish from RA >60 minutes)
- Pain on rising from seated, on stairs, with prolonged walking
- Loss of internal rotation and flexion (first movements lost)
- Positive FABER/FADIR test; Antalgic gait; Thomas test positive for flexion contracture
| Grade | Features |
|---|---|
| 0 | Normal |
| I | Possible osteophytes; no joint space loss |
| II | Definite osteophytes; minimal JSN |
| III | Moderate JSN; sclerosis; possible deformity |
| IV | Severe JSN; subchondral cysts; definite deformity |
2. Hip Fractures
- Intracapsular (femoral neck): Blood supply to femoral head at risk → AVN; treated with hemiarthroplasty (displaced) or cannulated screws (undisplaced)
- Extracapsular (intertrochanteric, subtrochanteric): Blood supply intact; treated with DHS or intramedullary nail
- Elderly fall due to tripping, postural instability, or syncope
- Ground reaction force exceeds bone strength at the femoral neck
- Reduced protective reflexes (slowed muscle activation) fail to attenuate the impact
- Reduced fat padding over the trochanter in elderly women increases fracture risk
3. Avascular Necrosis (AVN) of Femoral Head
- Blood supply disruption → osteonecrosis → subchondral fracture → femoral head collapse
- Ficat-Arlet classification (Stage I-IV)
- Stage I-II: non-weight-bearing + bisphosphonates + physiotherapy for ROM/strength
- Stage III-IV: total hip arthroplasty
4. Trochanteric Bursitis (Greater Trochanteric Pain Syndrome)
- Gluteal tendinopathy (primarily gluteus medius tendon) ± bursal involvement
- Compressive loads on the tendon during hip adduction in stance
- Common in obese elderly women with OA of contralateral hip
- Positive Ober's test; pain on palpation of greater trochanter
5. Femoroacetabular Impingement (FAI)
- Now recognized in the elderly as a precursor to hip OA
- Cam type: aspherical femoral head
- Pincer type: acetabular over-coverage
- Causes labral tears and chondral damage with repetitive motion
PART C: PHYSIOTHERAPY MANAGEMENT OF HIP DYSFUNCTION IN THE ELDERLY
FRAMEWORK: ICF-BASED APPROACH
- Body functions/structures: Pain, ROM, muscle strength, proprioception
- Activity limitations: Walking, rising from chairs, stair climbing
- Participation restrictions: ADL, social engagement, quality of life
I. PHYSIOTHERAPY MANAGEMENT OF HIP OSTEOARTHRITIS
Phase 1: Pain Management and Acute Phase (0-4 weeks)
- TENS/IFC: Analgesic via gate control; enables exercise participation
- Ultrasound (therapeutic): Thermal effects increase tissue extensibility; useful pre-exercise for capsular tightness
- Short-wave diathermy: Deep heating; reduces morning stiffness
- Hip mobilization (Maitland Grade I-II): Oscillatory techniques for pain relief; reduces joint pressure via synovial fluid circulation
- Longitudinal distraction of hip: Reduces compressive forces within the joint; improves capsular extensibility
- Hip posteroanterior mobilization: Restores posterior glide (lost in hip flexion contracture)
- Walking aid prescription (cane in contralateral hand - see biomechanical rationale above)
- Activity modification: avoid high-JRF activities (running, heavy lifting, prolonged stairs)
Phase 2: ROM and Flexibility (Weeks 2-8)
- Thomas stretch (hip flexor / anterior capsule): critical for addressing flexion contracture
- Hip internal rotation stretch: most restricted movement in hip OA
- Hip adductor stretching: often tight due to coxa valgus posture
- Piriformis/external rotator stretch
Phase 3: Strengthening (Weeks 4-16)
- Hip abductors (gluteus medius, minimus) - PRIMARY
- Hip extensors (gluteus maximus)
- Hip flexors (iliopsoas)
- Quadriceps and hamstrings - for knee-hip kinematic chain
| Stage | Exercises | Resistance | Frequency |
|---|---|---|---|
| Early | Side-lying abduction; clamshells; supine hip extension | Body weight | 3×/week |
| Mid | Resistance band abduction; mini-squats; step-ups | Low-moderate resistance | 3×/week |
| Late | Functional lunges; lateral band walks; step-ups with load | Moderate-heavy | 3×/week |
Phase 4: Neuromuscular and Proprioceptive Training
- Single-leg balance on firm → foam surface → rocker board
- Perturbation training
- Dual-task balance training (cognitive + motor)
- Otago Exercise Programme: evidence-based home fall prevention program specifically validated in elderly
Phase 5: Aerobic and Functional Training
- Hydrotherapy/aquatic therapy: Warmwater (33-35°C) buoyancy reduces JRF to <1BW; ideal for severely painful joints or post-operative early rehabilitation; improves cardiovascular fitness without high joint loads (Centurião et al., systematic review, Physiother Res Int, 2024, PMID: 37602930)
- Cycling: Low JRF (~1.3BW); excellent for hip OA
- Nordic Walking: Reduces hip loading compared to standard walking
II. PHYSIOTHERAPY MANAGEMENT AFTER HIP FRACTURE AND HIP ARTHROPLASTY
Acute Phase (Day 1-3 post-surgery)
- Bed-to-chair transfers with hip precautions
- Deep breathing exercises (DVT prevention, atelectasis prevention)
- Ankle pumps (circulatory)
- Isometric gluteal and quadriceps contractions
- Active ankle and knee ROM within bed
Sub-acute Phase (Day 3 - Week 6)
- Progressive weight-bearing as per surgical protocol (NWB → PWB → WBAT → FWB)
- Gait training with appropriate walking aid (Zimmer frame → crutches → cane)
- Hip precautions for posterior approach THA:
- No flexion >90°, adduction past midline, internal rotation
- Raised toilet seat, chair adaptations
- Straight leg raises, hip abduction in lying
- Quadriceps sets, terminal knee extensions
Recovery Phase (Week 6-12+)
- Progressive hip abductor and extensor strengthening
- Normalization of gait pattern (Trendelenburg correction)
- Balance and proprioceptive retraining
- Fall prevention education
III. FALLS PREVENTION - CRITICAL IN GERIATRIC HIP MANAGEMENT
- Gait speed test (<0.8 m/s = high fall risk)
- Timed Up-and-Go (TUG) test (>12 sec = high fall risk)
- Berg Balance Scale
- Medication review (polypharmacy, antihypertensives, sedatives)
- Balance training (Otago programme): 35% reduction in falls in RCTs
- Home hazard modification advice
- Appropriate footwear guidance
- Vitamin D optimization (reduces falls and fracture risk)
PART D: OARSI / NICE / AAOS GUIDELINES - EVIDENCE HIERARCHY
NICE Guidelines 2022 (NG226) for Hip OA:
- Core treatments (for all patients): Therapeutic exercise + patient education + weight management
- Adjuncts: Manual therapy as supplement to exercise; walking aids
- Not recommended: TENS, ultrasound, pulsed shortwave, laser therapy alone (insufficient evidence)
- Pharmacological: Topical NSAIDs first; oral NSAIDs second
- Surgical: THA for severe refractory OA
- Strong recommendation for exercise therapy (aerobic + strengthening)
- Moderate recommendation for weight loss
- NSAIDs preferred over opioids
- Physical therapy recommended both conservatively and postoperatively
RECENT ADVANCES (Critical for MPT marks)
-
Landmark RCT - THA vs. Resistance Training (Frydendal et al., NEJM 2024, PMID: 39476341):
- First RCT comparing THA vs. 12-week progressive resistance training in severe hip OA
- THA superior to resistance training alone at 1 year for pain and function
- BUT resistance training produced clinically significant improvements even in severe OA
- Clinical implication: physiotherapy should be maximally trialed before THA, and THA outcome is further improved by perioperative physiotherapy
-
Progressive Resistance Training Equivalent to Neuromuscular Exercise (Kjeldsen et al., Ann Intern Med 2024, PMID: 38588540):
- Multicenter cluster RCT: progressive resistance training (PRT) vs. neuromuscular exercise (NEMEX) for hip OA
- Both equally effective for pain relief and functional improvement
- PRT simpler to implement in community settings
-
AAOS Hip OA Guidelines Update 2024:
- Three strong recommendations: exercise therapy, weight loss, patient education
- Updated to include consideration of hip-spine relationship in THA planning
-
Exercise Volume-Response in Hip OA (Marriott et al., Arthritis Care Res 2024, PMID: 38317328):
- Higher exercise adherence = better outcomes; dose-response relationship confirmed
- Minimum: 3 sessions/week × 8 weeks for clinically meaningful improvement
-
GRASP Taxonomy applied to Hip Assessment: AI-driven gait analysis systems now quantify hip abductor moment, JRF, and pelvic kinematics during walking - enabling personalized exercise prescription based on individual biomechanical profiles.
-
Fragility Hip Fracture Pattern Characterization (Lim et al. 2024, PMID: 39277968): Falls causing lateral impact on greater trochanter in the elderly → intertrochanteric > femoral neck fractures. Hip protectors + fall-prediction algorithms may reduce fracture burden.
-
Exercise Dropout in OA (Vancampfort et al., Arch Phys Med Rehabil 2024, PMID: 38484833):
- ~25% dropout from exercise programs in hip OA
- Predictors: pain severity, low self-efficacy, lack of social support
- Physiotherapy implication: behavioral change strategies and motivational interviewing are as important as exercise technique
REFERENCES
- Bailey and Love's Short Practice of Surgery, 28th Edition. Chapter 39: Biomechanics of the Hip Joint. pp. 572-573.
- THIEME Atlas of Anatomy: General Anatomy and Musculoskeletal System. Section 1.15: Movements and Biomechanics of the Hip Joint.
- Pauwels F. Biomechanics of the Locomotor Apparatus. Berlin: Springer, 1980.
- Norkin CC & Levangie PK. Joint Structure and Function: A Comprehensive Analysis. 5th Ed. F.A. Davis, 2011.
- Rockwood and Green's Fractures in Adults, 10th Ed. 2025. Ligamentous Anatomy of the Hip.
- Marriott KA, et al. Resistance Exercise for Hip and Knee OA: Systematic Review and Meta-Analysis. Arthritis Care Res. 2024. [PMID: 38317328]
- Frydendal T, et al. Total Hip Replacement or Resistance Training for Severe Hip OA. N Engl J Med. 2024. [PMID: 39476341]
- Kjeldsen T, et al. Progressive Resistance Training or Neuromuscular Exercise for Hip OA: RCT. Ann Intern Med. 2024. [PMID: 38588540]
- Sinatti P, et al. Patient Education for Hip and Knee OA: Systematic Review. IJERPH. 2022. [PMID: 35627729]
- Caduda SDS, et al. Physical exercise for hip OA: systematic review with meta-analysis. J Bodyw Mov Ther. 2025. [PMID: 39663077]
- Montero-Odasso MM, et al. Clinical Practice Guidelines on Fall Prevention: Systematic Review. JAMA Netw Open. 2021. [PMID: 34910151]
- Lim SK, et al. Fragility hip fracture-related falls in older adults: Systematic Review. J Nutr Health Aging. 2024. [PMID: 39277968]
- Centurião JHVM, et al. Aquatic exercises after THA: Systematic Review. Physiother Res Int. 2024. [PMID: 37602930]
- NICE Guideline NG226. Osteoarthritis in over 16s: diagnosis and management. 2022.
- AAOS Clinical Practice Guideline: Hip Osteoarthritis. Updated 2024.
- Koc TA et al. Hip Pain and Mobility Deficits - Hip OA: Revision 2025. Clinical Practice Guidelines, Academy of Orthopaedic Physical Therapy. 2025.
EXAMINER TIPS (MPT Topper Insight)
- The lever arm diagram/calculation must be included - it demonstrates MPT-level biomechanical depth
- Connect EVERY biomechanical concept to a clinical decision (the "therefore" rule: "abductor lever arm is short → therefore cane in contralateral hand reduces JRF by X%")
- Tables for gait deviations, JRF at activities, and THA decisions earn structured marks
- Cover Pauwels' lever arm model with the equation clearly stated
- Trendelenburg sign and gait with clear biomechanical explanation earns major marks
- Coxa valga vs. vara comparison table differentiates from average answers
- Mandatory sections: Sarcopenia, Osteoporosis, OA Pathomechanics, Hip Fracture, Management (with phases), Falls Prevention
- ICF framework shows clinical reasoning sophistication
- Recent 2024-2025 RCTs (NEJM 2024 - THA vs. resistance training; Ann Intern Med 2024 multicenter RCT) are highly examinable
- Outcome measures (TUG, Berg, WOMAC, VAS, Stair Climb Test) must be mentioned
4. Analyse the effect of hip pathology on gait and discuss management for the same. 30 M(Summer 2018) 5. Hip abductor mechanism and its clinical application. 10 M(Winter 2017) MPT level topper answer with references and recent advances
hip pathology gait deviation biomechanics analysis
gluteus medius hip abductor strength gait Trendelenburg
hip osteoarthritis gait kinematics kinetics alterations
hip abductor strengthening exercise clinical outcomes rehabilitation
hip osteoarthritis gait speed walking functional outcomes exercise
hip pathology gait deviation antalgic Trendelenburg stiff hip short limb gait biomechanical analysis management physiotherapy
hip osteoarthritis gait stage-specific deviations biomechanics
total hip arthroplasty gait kinematics functional improvement wearable sensor
hip abductor strengthening Trendelenburg gait rehabilitation exercise program
hip abductor mechanism clinical applications Pauwels lever arm THA offset gait training physiotherapy 2024
hip OA gait training neuromuscular exercise progressive resistance outcomes RCT
MPT-Level Answers: MUHS Summer 2018 & Winter 2017
QUESTION 4
Analyse the Effect of Hip Pathology on Gait and Discuss Management (30 Marks)
INTRODUCTION
PART A: NORMAL GAIT - THE REFERENCE FRAMEWORK
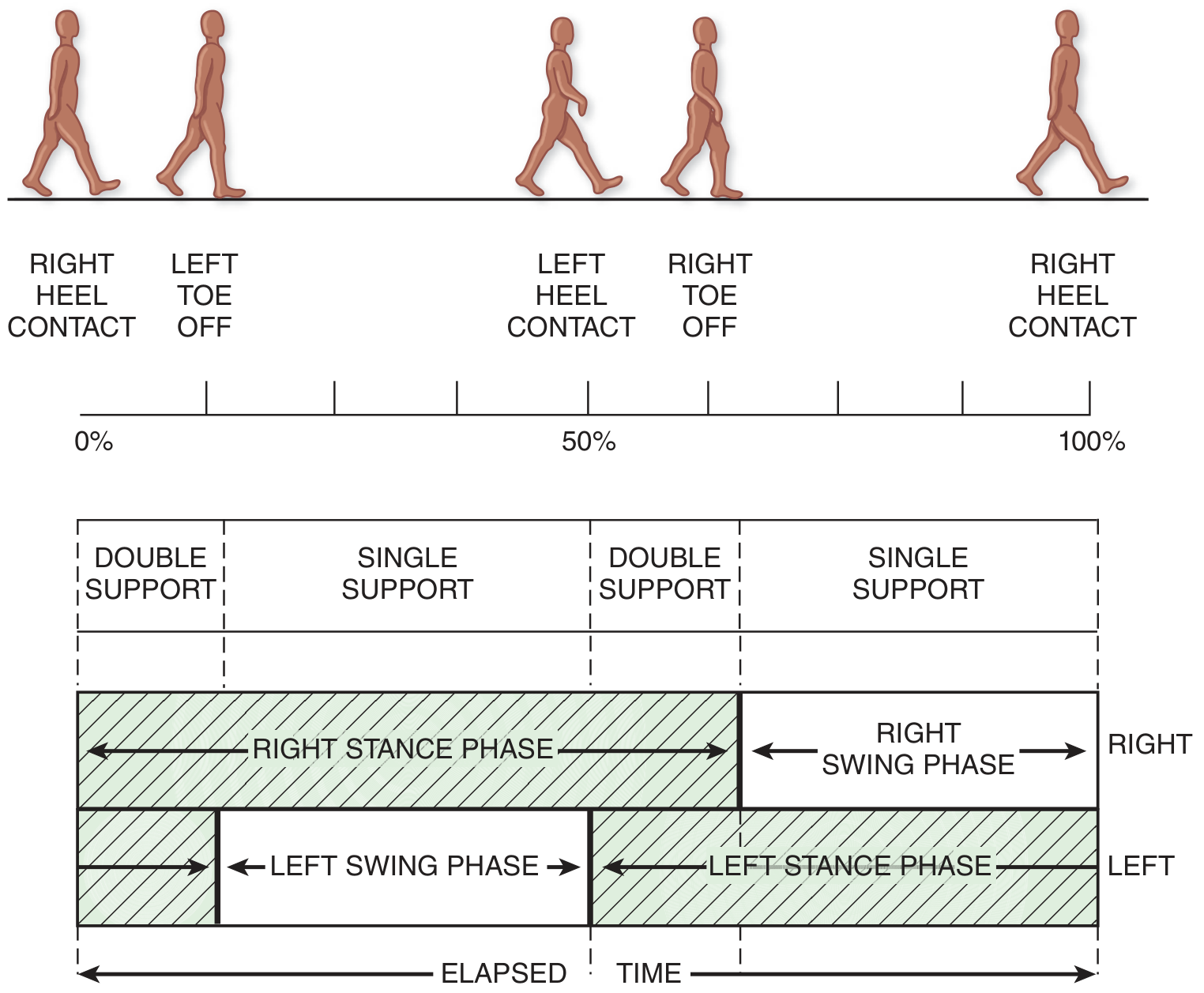
Gait Cycle Components
| Parameter | Normal Value |
|---|---|
| Gait cycle duration | ~1.0 second |
| Stance phase | 60-65% of cycle |
| Swing phase | 35-40% of cycle |
| Double limb support | 20-25% of cycle (two periods of ~10-12% each) |
| Cadence | 90-120 steps/minute |
| Walking speed | 1.3-1.5 m/second (adults) |
| Step length | 0.65-0.75 m |
| Stride width | 7-9 cm |
Normal Hip Kinematics During Gait
| Phase | Event | Hip Motion |
|---|---|---|
| Initial contact (heel strike) | Heel contacts ground | 25-30° flexion |
| Loading response | Weight accepted | Flexion → loading |
| Mid-stance | Opposite toe-off; single limb support | Decreasing flexion; abductor active (pelvis level) |
| Terminal stance | Heel rise | 0-10° extension; power generated by hip extensors |
| Pre-swing | Toe-off | Maximum extension; passive hip flexion begins |
| Swing phase | Limb advancing | 0-30° flexion; limb clearance |
Hip Muscles Active During Normal Gait
| Phase | Muscle | Function |
|---|---|---|
| Heel strike | Gluteus maximus, Hamstrings | Decelerate forward swing; hip extension moment |
| Mid-stance | Gluteus medius, minimus | Pelvic stabilization (contralateral pelvis level) |
| Push-off / Terminal stance | Iliopsoas | Hip flexion initiation |
| Swing phase | Iliopsoas, Rectus femoris | Limb advancement; hip flexion |
- Antigravity support of the body
- Stepping
- Maintenance of equilibrium
- Propulsion
PART B: PATHOLOGICAL GAIT PATTERNS DUE TO HIP PATHOLOGY
1. ANTALGIC GAIT (Painful Gait)
- Pain arises during weight-bearing stance, when the hip joint reaction force (JRF) peaks at 3-4× body weight
- The nervous system reduces pain by minimizing time and force of loading on the affected side
- The patient accelerates through the painful stance phase (shortened stance) and decelerates on the contralateral healthy side (prolonged contralateral stance)
- "Dot-dash" rhythm: short on affected side (dot), long on unaffected side (dash)
- Reduced stride length on the affected side
- Decreased walking speed
- Reduced hip extension and flexion ROM on the affected side
- Increased double support time (patient spends more time with both feet on ground to reduce single-limb loading demands)
- Trunk lean toward affected side (reduces JRF by shortening body weight lever arm - see biomechanical rationale)
- Cadence: reduced
- Step length affected side: significantly shortened
- Walking speed: markedly reduced
- Single limb support time: shortened on affected side
2. TRENDELENBURG GAIT (Abductor Weakness Gait)
- The gluteus medius cannot generate sufficient torque (abductor force × lever arm) to counterbalance the gravitational torque of body weight (body weight × body weight lever arm)
- The contralateral pelvis drops (positive Trendelenburg)
- The center of gravity deviates toward the unsupported side
- Patient cannot generate abductor force sufficient to level pelvis
- Contralateral pelvis drops visibly during stance
- Seen in severe gluteus medius weakness, superior gluteal nerve palsy
- Patient shifts trunk toward the affected side during stance
- This shifts the CoG laterally over the stance hip, reducing the body weight moment arm ("a" in Pauwels' equation)
- Reduces the required abductor force and thus the JRF
- An energy-expensive compensation; associated with secondary lumbar spine loading
- Visible lateral trunk lurch toward affected side on each stance phase
- Waddling or rolling gait bilaterally when bilateral (e.g., bilateral hip OA, bilateral superior gluteal nerve injury)
- Positive Trendelenburg test
3. STIFF HIP GAIT (Circumduction Gait)
- Normal hip requires ~25-30° of flexion at heel strike and ~10-15° extension at push-off
- Loss of hip flexion → reduced swing limb advancement → foot dragging risk
- Compensation: patient hikes the pelvis (elevation) and circumducts (swings the limb out in an arc) to clear the foot during swing phase
- Reduced hip flexion and extension ROM during gait
- Increased pelvic tilt and rotation to compensate
- Circumduction or hip hitching (pelvic elevation) during swing
- Reduced step length
- Reduced walking speed
4. SHORT LIMB GAIT (Leg Length Discrepancy Gait)
- Real LLD: difference in femoral/tibial length (e.g., post-femoral neck fracture with shortening, congenital)
- Apparent LLD: adduction/abduction contracture tilting the pelvis (common in hip OA)
- Shorter limb stance: pelvis drops on shorter side (similar to Trendelenburg)
- Compensatory mechanisms: equinus of shorter limb (toe walking), vaulting over longer limb in swing, lateral trunk sway
- Asymmetric pelvic movement
- Increased lumbar scoliosis (concave on longer limb side)
- Increased energy expenditure
5. INTERNAL ROTATION (IN-TOEING) GAIT
- Femoral anteversion (normal = 10-15°; excess = >20°) causes internal rotation of the femur during gait
- Patient walks with feet turned in; risk of tripping as the foot of the swing limb catches the back of the stance leg calf
- Common in children; usually resolves by age 8-10 years
- Persistent adult anteversion: associated with hip OA (altered joint congruence)
6. HYPER-LORDOTIC GAIT (Hip FLEXION CONTRACTURE COMPENSATION)
- Hip flexion contracture (iliopsoas, anterior capsule) prevents full hip extension during terminal stance
- Prevents normal contralateral limb advancement
- Patient compensates by increasing lumbar lordosis during stance (anterior pelvic tilt)
- Results in abnormal loading of lumbar spine - associated with low back pain
- Thomas test positive for flexion contracture
- Exaggerated lumbar lordosis during walking (especially visible from the side)
- Reduced stride length
- Characteristic "swayback" appearance
7. GLUTEUS MAXIMUS GAIT
- Gluteus maximus generates the hip extension moment at heel strike and loading response
- Weakness → uncontrolled hip flexion after heel strike; risk of jackknife collapse
- Compensation: patient leans the trunk posteriorly at heel strike (shifts CoG posterior to the hip joint center) - creating an external extension moment that substitutes for gluteus maximus
- Backward trunk lean at heel strike
- "Gluteus maximus lurch" posteriorly
- Appears as "pump-handle" motion of trunk
SUMMARY TABLE: GAIT DEVIATIONS IN HIP PATHOLOGY
| Gait Deviation | Primary Impairment | Compensation | Typical Cause |
|---|---|---|---|
| Antalgic | Pain during weight bearing | Shortened stance; lateral trunk lean | Hip OA, fracture, infection |
| Trendelenburg | Gluteus medius weakness | Lateral trunk shift toward affected side | Hip OA, nerve palsy, CDH |
| Stiff hip / Circumduction | Reduced hip ROM | Pelvic hike / circumduction | Severe OA, ankylosis |
| Short limb | Limb length discrepancy | Equinus; lateral pelvic tilt | Fracture shortening, CDH |
| In-toeing | Femoral anteversion | None / trip risk | Anteversion, OA |
| Flexion contracture | Hip flexor tightness | Lumbar hyperlordosis | OA, prolonged immobility |
| Gluteus maximus lurch | Hip extensor weakness | Posterior trunk lean | Nerve injury, post-surgery |
PART C: GAIT ANALYSIS METHODS
1. Observational Gait Analysis (OGA)
- Clinical standard; used by physiotherapists
- Observe from front, back, both sides during normal walking
- Evaluate: symmetry, trunk sway, pelvic tilt, stride length, cadence, arm swing
- Tools: Edinburgh Gait Score, Rancho Los Amigos Observational Gait Analysis (most comprehensive clinical tool)
2. Temporal-Spatial Parameters
- Comfortable gait speed: Best single predictor of functional outcome; <0.8 m/s = high risk in elderly
- Step length, stride length, cadence, step width
- Double support time: Increased in pain, weakness, balance impairment
3. Kinematic Analysis (3D Motion Capture)
- Gold standard for research
- Vicon, Motion Analysis systems: measures joint angles in all planes
- Hip kinematics in OA: Reduced hip flexion in swing, reduced hip extension in terminal stance, reduced transverse plane rotation, increased pelvis obliquity and rotation
4. Kinetic Analysis (Force Plates)
- Measures Joint Reaction Force (JRF), moments, and powers
- Hip abductor moment: Reduced in hip OA and after Trendelenburg gait (reduced demand due to trunk compensation)
- Hip power: Reduced at push-off; key marker of hip OA functional deficit
5. Wearable Sensor Technology (Recent Advance)
- Inertial Measurement Units (IMUs) on the thigh, shank, and pelvis
- Allow continuous, real-world gait monitoring outside the laboratory
- Kaufmann et al. (J Orthop Res 2023, PMID: 35880355): IMU-derived gait kinematics correlated significantly with patient-reported outcomes after THA
- Atelšek et al. (Sensors 2026, PMID: 42122452): Low-cost sensors reliably quantified gait improvements after THA and TKA in clinical settings
PART D: MANAGEMENT OF HIP PATHOLOGY AFFECTING GAIT
PHASE 1: ASSESSMENT AND GOAL SETTING
- Observational gait analysis (describe deviation, pattern, compensation)
- Temporal-spatial measures (TUG, 10MWT, 6MWT)
- Hip ROM measurement (goniometry; Thomas test for flexion contracture)
- Hip muscle strength testing (MRC scale; dynamometry for abductors)
- Trendelenburg test (static and dynamic)
- Leg length measurement (real: ASIS to medial malleolus; apparent: navel to medial malleolus)
- Body functions: Improve hip ROM, reduce pain (VAS), improve abductor strength (MRC/dynamometry)
- Activity: Normalize gait speed, stride length, eliminate limp
- Participation: Return to community ambulation, work, leisure
PHASE 2: PAIN MANAGEMENT (Addressing Antalgic Gait)
- TENS (gate control analgesia): reduces pain during ambulation
- Ultrasound (thermal): pre-exercise to improve capsular extensibility
- IFC: deep muscle analgesia
- Hip mobilization (Maitland Grade I-II oscillations): pain neurophysiology effects
- Soft tissue release: iliopsoas, piriformis, TFL
- Cane in the contralateral hand for antalgic gait: reduces JRF by 30-40%
- Bilateral crutches for severe pain (PWB or NWB)
- Cane promotes normalized stance phase duration on affected side
PHASE 3: RANGE OF MOTION RESTORATION (Addressing Stiff Hip / Flexion Contracture Gait)
- Thomas stretch (kneeling lunge): anterior hip capsule and iliopsoas
- Hip internal rotation stretch: most restricted in OA
- Piriformis stretch: "figure 4" position; addresses external rotator tightness
- TFL/ITB stretch: modified Ober's position; relieves lateral hip compressive loading
- Posterior-inferior long-axis distraction: reduces compressive joint stress; improves flexion and abduction
- Anterior-posterior hip glide: improves internal rotation
- Maitland Grade III-IV: to restore ROM in stiff joints
PHASE 4: HIP ABDUCTOR STRENGTHENING (Addressing Trendelenburg Gait - PRIMARY INTERVENTION)
- Increases abductor torque capacity at the hip
- Reduces required trunk compensation (lateral trunk shift)
- Normalizes pelvic stability in stance
- Reduces JRF by improving mechanical efficiency
| Stage | Exercise | Load | Position |
|---|---|---|---|
| Stage 1 (0-2 weeks) | Side-lying hip abduction (leg raises) | Body weight | Non-weight-bearing |
| Stage 1 | Clamshells | Body weight | Side-lying |
| Stage 2 (2-4 weeks) | Resistance band side-stepping | Theraband | Standing |
| Stage 2 | Side-lying abduction with resistance band | Theraband | Side-lying |
| Stage 3 (4-8 weeks) | Single-leg mini-squat | Body weight | Standing |
| Stage 3 | Lateral band walks | Theraband | Standing/functional |
| Stage 4 (8-12 weeks) | Step-ups (lateral and forward) with load | Dumbbell/vest | Functional/closed chain |
| Stage 4 | Single-leg stance with perturbation | Bodyweight | Proprioceptive |
- Patellofemoral pain syndrome (hip abductor weakness → femoral internal rotation → patella maltracking)
- Knee OA (Thomas et al. meta-analysis, BMC Musculoskeletal Disorders 2022, PMID: 35768802): hip abductor strengthening reduces knee pain in knee OA
- Iliotibial band syndrome (strong abductors reduce excessive hip adduction during running)
PHASE 5: GAIT RETRAINING
| Gait Deviation | Retraining Strategy |
|---|---|
| Antalgic gait | Normalize stance phase duration with visual/tactile feedback; metronome-paced walking |
| Trendelenburg gait | Lateral trunk shift correction with mirror feedback; theraband resisted lateral walking; single-leg balance |
| Stiff hip gait | Hip ROM exercises pre-gait; visual feedback to increase step length; treadmill training |
| Short limb gait | Heel raise orthosis for true LLD <2 cm; custom orthosis for >2 cm; gait retraining for apparent LLD |
| Flexion contracture gait | Hip flexor stretching; posterior pelvic tilt exercises; lumbar extension exercises |
- Visual feedback: Full-length mirrors or video gait analysis
- Auditory feedback: Metronome for cadence normalization
- Tactile feedback: Theraband around pelvis for pelvic stability cues
- Treadmill training: Allows controlled progressive loading; facilitates longer step length
- Nordic walking: Poles reduce hip loading (~25%) while encouraging normal gait mechanics
PHASE 6: NEUROMUSCULAR AND PROPRIOCEPTIVE TRAINING
- Single-leg balance on firm surface → foam pad → wobble board: Progressively challenges proprioceptive pathways
- Perturbation training: Unexpected platform shifts; trains rapid neuromuscular response
- Dual-task training: Walking while performing cognitive tasks; reduces dual-task interference that exacerbates gait deviations in elderly
PHASE 7: FUNCTIONAL TRAINING AND RETURN TO ADL
- Chair rise training: Eccentric quadriceps + hip extensor loading
- Stair training: Step-over-step; progressive height
- Community ambulation tasks: Curbs, slopes, uneven ground
- Occupational and vocational tasks: Progressive activity tolerance
PHASE 8: POST-OPERATIVE REHABILITATION (Post-THA)
- Surgical trauma to abductor muscles
- Pain inhibition
- Dislocation precautions
- Altered hip geometry (if offset not restored)
- Early mobilization (Day 1): standing, weight-bearing as tolerated
- Hip precautions compliance: no flexion >90°, adduction, internal rotation (posterior approach)
- Progressive gait training with walker → crutches → cane (contralateral)
- Hip abductor strengthening: priority from week 2 onwards
- Normalize gait by 6-12 weeks
PART E: OUTCOME MEASURES FOR GAIT ASSESSMENT IN HIP PATHOLOGY
| Outcome Measure | Parameter | Interpretation |
|---|---|---|
| 10-Meter Walk Test (10MWT) | Comfortable gait speed | <0.8 m/s = high risk; >1.2 m/s = community ambulator |
| Timed Up and Go (TUG) | Functional mobility | <10 sec = normal; 10-20 sec = problem; >20 sec = severely limited |
| 6-Minute Walk Test (6MWT) | Walking endurance | Reflects cardiovascular and functional capacity |
| Berg Balance Scale | Balance during gait and stance | <45/56 = fall risk |
| Harris Hip Score | Hip function (pain, ROM, gait) | Standard surgical outcome measure |
| WOMAC (Western Ontario McMaster) | OA-specific pain, stiffness, function | Most validated hip OA outcome |
| HOOS (Hip disability and Osteoarthritis Outcome Score) | Patient-reported hip function | 5 subscales; comprehensive |
RECENT ADVANCES
-
Stage-Specific Gait Deviations in Hip OA (Subasinghe et al., Gait Posture 2025, PMID: 40288032):
- First study to characterize gait deviations according to Kellgren-Lawrence OA stage
- Mild OA: reduced hip extension in terminal stance
- Moderate OA: additional reduction of walking speed and cadence
- Severe OA: marked circumduction, Trendelenburg, and antalgic pattern
- Clinical implication: gait assessment should guide staging and intervention timing
-
Progressive Resistance Training = Neuromuscular Exercise for Hip OA (Kjeldsen et al., Ann Intern Med 2024, PMID: 38588540):
- Multicenter cluster RCT: both equally effective for improving gait-related functional outcomes
- Simplifies clinical decision-making
-
THA vs. Resistance Exercise for Severe Hip OA (Frydendal et al., NEJM 2024, PMID: 39476341):
- THA superior at 1 year for severe OA
- However, resistance training produced meaningful gait and functional improvements even in severe OA
- Physiotherapy pre-THA ("prehabilitation") and post-THA together optimize outcomes
-
Wearable IMU-Based Gait Analysis:
- Low-cost IMU sensors can quantify gait speed, step length, trunk sway, and pelvic obliquity in real-world settings (Atelšek et al. 2026, PMID: 42122452)
- Enables remote monitoring of rehabilitation progress; personalized gait training feedback
-
Gluteus Maximus Transfer for Irreparable Abductor Deficiency (Song et al., J Arthroplasty 2024, PMID: 37879422):
- Meta-analysis: gluteus maximus transfer restores Trendelenburg gait in patients with irreparable gluteus medius tears post-THA
- Post-operative PT essential: abductor strengthening and gait retraining
QUESTION 5
Hip Abductor Mechanism and Its Clinical Applications (10 Marks)
INTRODUCTION
ANATOMY OF THE HIP ABDUCTOR MECHANISM
Primary Muscles
- Origin: Outer surface of ilium, between posterior and anterior gluteal lines
- Insertion: Lateral surface of greater trochanter
- Nerve supply: Superior gluteal nerve (L4, L5, S1)
- Function:
- Anterior fibers: abduction + internal rotation
- Middle fibers: pure abduction
- Posterior fibers: abduction + external rotation
- During stance phase: primary pelvic stabilizer in frontal plane
- Origin: Outer ilium between anterior and inferior gluteal lines
- Insertion: Anterior surface of greater trochanter
- Nerve: Superior gluteal nerve (L4, L5, S1)
- Function: Assists abduction and internal rotation; deep pelvic stabilizer
- Origin: ASIS and iliac crest
- Insertion: Iliotibial band → lateral condyle of tibia
- Nerve: Superior gluteal nerve (L4, L5)
- Function: Assists abduction; stabilizes knee in extension via ITB
- Accessory abductor during resisted movements
Secondary Component: Iliotibial Band (Pauwels' Tension Band)
- Acts as a lateral tension band of the femoral shaft
- Converts bending moments in the femoral neck into compressive forces
- Reduces the magnitude of abductor force required for pelvic stability by ~30-50%
- Pauwels (1976) incorporated the ITB into his updated static biomechanical model: the ITB helps the abductors by acting as a passive stabilizer, sharing the load during stance
BIOMECHANICS OF THE ABDUCTOR MECHANISM
The Lever Arm Equation (Pauwels)
What Determines the Abductor Lever Arm Length?
- Neck-shaft angle: Coxa vara (decreased angle) → increases abductor lever arm → reduces required abductor force; Coxa valga (increased angle) → decreases abductor lever arm → increases required abductor force
- Femoral offset: Perpendicular distance from hip center to femoral shaft. Greater offset = longer abductor lever arm = less abductor force needed = reduced JRF
- Position of greater trochanter: More lateral position → longer abductor lever arm
- Pelvis width: Wider pelvis → longer body weight lever arm → greater abductor force needed (reason women have higher hip JRF than men)
CLINICAL ASSESSMENT OF THE ABDUCTOR MECHANISM
1. Trendelenburg Test (Static)
- Patient stands on the affected limb; opposite limb lifted
- Observe the contralateral pelvis level
- Positive: Contralateral pelvis drops >2° - indicates abductor weakness or pain inhibition
- Negative: Contralateral pelvis remains level or rises - abductors intact
| Category | Specific Cause |
|---|---|
| Muscle weakness | Superior gluteal nerve palsy (L4, L5, S1), poliomyelitis |
| Pain inhibition | Hip OA, trochanteric bursitis, fractured neck of femur |
| Short abductor lever arm | Coxa valga, CDH with proximal femoral deformity |
| Bone pathology | AVN with femoral head collapse, Perthes disease |
| Post-surgical | THA with inadequate offset restoration, post-osteotomy |
2. Hip Abduction Strength Testing
- Manual Muscle Test (MRC 0-5): Side-lying hip abduction against gravity and resistance
- Dynamometry (hand-held): Most reliable; standard position: side-lying, hip neutral
- Normal values: ~30-40 kg in adults; side-to-side difference >15% is clinically significant
- Trendelenburg threshold: When abductor strength falls below ~50% of normal, Trendelenburg gait typically develops
3. Functional Tests
- 30-second Chair Stand Test: Tests global lower limb power including abductors
- Single-leg balance test: Duration of balance on affected limb (normal >10 sec)
- Lateral step-up test: Eccentric abductor loading; reveals weakness not apparent in isolated testing
- Ober's Test: Tests TFL/ITB tightness, relevant to abductor mechanism function
CLINICAL APPLICATIONS OF HIP ABDUCTOR MECHANISM KNOWLEDGE
1. Diagnosis and Classification of Gait Deviations
- Trendelenburg gait from antalgic gait (clinical and biomechanical distinction)
- Pain-inhibited abductor dysfunction (resolves with pain management) from true abductor weakness (requires strengthening)
- Structural abductor insufficiency (post-THA with inadequate offset) from neuromuscular abductor weakness (responds to exercise)
2. Walking Aid Prescription
- Reduces required abductor muscle force
- Reduces JRF by 30-40% (~1-1.5× body weight)
- Walking aid prescription should be based on abductor strength and Trendelenburg status
- Severe abductor weakness or Trendelenburg: Walker frame (bilateral) → crutches → cane (contralateral)
- Mild to moderate: Single cane in contralateral hand
3. Total Hip Arthroplasty - Surgical Planning
| Surgical Decision | Biomechanical Effect |
|---|---|
| Restore/increase femoral offset | Longer abductor lever arm → less abductor force needed → reduced JRF; prevents Trendelenburg post-THA |
| Medialize acetabular cup | Shortens body weight lever arm → reduces JRF |
| Correct leg length inequality | Equalizes lever arms; prevents pelvic tilt and secondary gait deviations |
| Avoid abductor muscle damage during approach | Preserves abductor force-generating capacity |
4. Post-THA Abductor Rehabilitation
- Directly traumatized during posterior or lateral approach
- Detached and reattached (greater trochanter osteotomy - historical)
- Protected by direct anterior approach (DAAT approach avoids abductor dissection - advantage for early abductor function)
- Week 0-2: Isometric gluteal sets; supine hip abduction in pain-free range
- Week 2-6: Side-lying progressive hip abduction; resistance band abduction
- Week 6-12: Functional abductor loading: step-ups, lateral band walks
- Week 12+: Single-leg stance; return to community activities
5. Gluteal Tendinopathy - Compression Model
- Greater trochanteric pain syndrome results from compressive load on the gluteal tendons where they wrap around the greater trochanter
- Hip adduction in standing and during gait (crossing midline) increases compressive load on the gluteus medius tendon
- Management: avoid adduction postures (not "crossing legs", not standing with hip dropped); progressive tendon loading exercises; modify gait to reduce hip adduction moment
6. Knee Osteoarthritis - Hip Abductor Connection
- Weak hip abductors → femoral internal rotation and adduction during stance → increased medial compartment knee loading → medial knee OA progression
- Patellofemoral pain: hip abductor weakness → femoral internal rotation → lateral patellar maltracking
7. Low Back Pain - Abductor Connection
- Gluteus medius weakness → Trendelenburg gait → contralateral trunk lean → asymmetric lumbar loading
- Unilateral abductor weakness → pelvic obliquity → scoliosis → lumbar facet joint loading
- Assessment of hip abductors is essential in all low back pain patients with gait deviations
8. Femoroacetabular Impingement (FAI) and Labral Tears
- Hip abductor weakness is a common finding in FAI patients
- Increased femoral neck stress during single-limb stance in the presence of cam or pincer morphology
- Abductor strengthening as part of conservative FAI management reduces impingement by improving dynamic joint congruence
RECENT ADVANCES
-
Stage-Specific Gait Deviations - Abductor Mechanism (Subasinghe et al., 2025, PMID: 40288032): Abductor moment deficits correlate with OA severity; even mild OA shows measurable abductor moment reduction before overt Trendelenburg develops.
-
Gluteus Maximus Transfer for Irreparable Abductor Deficiency (Song et al., J Arthroplasty 2024, PMID: 37879422): Systematic review confirming that gluteus maximus transfer is effective for irreparable gluteus medius tears post-THA; post-operative PT is essential for retraining the transferred muscle's abductor function.
-
Effort, Fulcrum, and Lever Failures Framework (2024): New conceptual framework categorizing abductor mechanism failure as: (a) Effort failure (muscle weakness), (b) Fulcrum failure (bone pathology at femoral head), (c) Lever failure (reduced abductor lever arm). This framework enables more targeted rehabilitation (strengthening vs. gait modification vs. surgical/orthotic correction).
-
Hip Abductor Connection to Knee and Spine: Growing evidence confirms that the abductor mechanism is the common link in a kinematic chain affecting the lumbo-pelvic-hip-knee complex - validating comprehensive lower extremity rehabilitation approaches.
-
WALANT Surgery and Intraoperative Abductor Assessment: WALANT technique allows surgeons to assess intraoperative active hip abduction, verifying that the abductor mechanism is intact and guiding post-operative rehabilitation expectations.
REFERENCES
- Bailey and Love's Short Practice of Surgery, 28th Edition. Chapter 35: Table 35.11 Common Limps; Chapter 39: Biomechanics of the Hip Joint.
- Adams and Victor's Principles of Neurology, 12th Edition. Chapter 6: Normal Gait Cycle. pp. 132-134.
- Norkin CC & Levangie PK. Joint Structure and Function: A Comprehensive Analysis. 5th Ed. F.A. Davis.
- Pauwels F. Biomechanics of the Locomotor Apparatus. Berlin: Springer, 1980.
- Inman VT, Ralston HJ, Todd F. Human Walking. Williams & Wilkins, 1981.
- Perry J & Burnfield JM. Gait Analysis: Normal and Pathological Function. 2nd Ed. SLACK Inc., 2010.
- Subasinghe Arachchige RSS, et al. Stage-specific gait deviations in individuals with hip OA. Gait Posture. 2025. [PMID: 40288032]
- Kjeldsen T, et al. Progressive Resistance Training or Neuromuscular Exercise for Hip OA: RCT. Ann Intern Med. 2024. [PMID: 38588540]
- Frydendal T, et al. Total Hip Replacement or Resistance Training for Severe Hip OA. N Engl J Med. 2024. [PMID: 39476341]
- Song BM, et al. Gluteus Maximus Transfer for Irreparable Hip Abductor Deficiency: Systematic Review and Meta-Analysis. J Arthroplasty. 2024. [PMID: 37879422]
- Thomas DT, et al. Hip abductor strengthening in patients with knee OA: Systematic Review and Meta-Analysis. BMC Musculoskelet Disord. 2022. [PMID: 35768802]
- Kaufmann M, et al. Functional assessment of THA using IMU: gait kinematics and patient-reported outcomes. J Orthop Res. 2023. [PMID: 35880355]
- Atelšek L, et al. Gait biomechanics after THA/TKA using low-cost sensors. Sensors. 2026. [PMID: 42122452]
- Grimaldi A & Fearon A. Gluteal tendinopathy: Integrating pathomechanics and clinical features in assessment and management. J Orthop Sports Phys Ther. 2015.
- NICE Guideline NG226. Osteoarthritis in over 16s: Diagnosis and Management. 2022.
EXAMINER TIPS (MPT Topper Insight)
- The NORMAL gait cycle must open the answer (establishes the reference baseline)
- Describe EACH gait deviation with: (1) Definition, (2) Biomechanical basis, (3) Clinical features, (4) Gait parameter changes, (5) Causes
- The Summary Table is essential for 30M answers - examiners can award structured marks
- Management must be organized by phases (Assessment → Pain → ROM → Strengthening → Gait retraining → Neuromuscular → Functional)
- Recent advances: Stage-specific gait deviations 2025, NEJM 2024 THA vs. exercise, IMU gait monitoring
- Equal weight on anatomy + biomechanics + clinical applications
- The Pauwels lever arm equation MUST be presented with the mathematical derivation (M = 3W)
- List 6-8 clinical applications - this differentiates MPT from BPT level
- Trendelenburg sign testing with interpretation table earns high marks
- Recent advance: gluteus maximus transfer (Song 2024 meta-analysis) + Effort-Fulcrum-Lever framework
1. Write an essay on physiotherapy assessment of low back pain and explain differential diagnosis with clinical reasoning. 30 M (Summer 2023) 2. Discuss management of lumbar stenosis. 10 M(Summer 2023) 3. Discuss evidence based treatment for groin soft tissue injuries. 10 M(Summer 2023) 4. Discuss pain assessment, modulation and management in non-specific chronic LBP. 30 M(Winter 2022) 5. Neural tissue mobilisation assessment and treatment techniques used in LBP. 30 M(Summer 2016) MPT level topper answers with references and recent advances
"low back pain" AND "physiotherapy assessment" AND "clinical reasoning"
"lumbar spinal stenosis" AND "physical therapy" AND treatment
groin injury adductor strain rehabilitation exercise evidence
"chronic low back pain" AND "pain neuroscience" AND "central sensitization"
"neural mobilization" AND "low back pain" AND neurodynamics
NICE guidelines low back pain 2024 physiotherapy assessment differential diagnosis red flags
groin pain adductor rehabilitation Copenhagen exercise athletes
"low back pain" AND clinical guidelines AND physiotherapy management
neurodynamic mobilization sciatic nerve radiculopathy outcomes
Copenhagen adductor exercise groin injury prevention rehabilitation evidence 2024 2025
pain neuroscience education chronic low back pain disability outcomes
neural tissue mobilization neurodynamics low back pain sciatic radiculopathy
neurodynamic assessment treatment Butler Shacklock low back pain sciatic nerve sliders tensioners evidence 2024
Examiner Tips: How These Answers Score at MPT Level
- Opens with the biopsychosocial framework - this is what separates MPT from BPT
- Red flags with the "TUNA FISH" mnemonic is highly memorable and marks complete
- Differential diagnosis table at the end earns structured marks efficiently
- Including Grainger & Allison (disc herniation incidental MRI findings in 20-36% of asymptomatic adults) demonstrates textbook depth
- Yellow/Blue/Orange flags and SBST stratification show contemporary clinical reasoning
- The neurogenic vs. vascular claudication table is a must - examiners expect it
- Citing three systematic reviews (Ammendolia 2022, Temporiti 2022, Kirker 2023) on PT interventions demonstrates evidence-based depth
- The bicycle test and shopping trolley sign as specific clinical features show clinical insight
- Doha Agreement 2015 classification is the expected opening - shows international currency
- Holmich Protocol RCT is the landmark evidence that every examiner expects mentioned
- Copenhagen Exercise 2025 meta-analysis (PMID: 40827942) shows awareness that current evidence is nuanced - it strengthens but doesn't prevent groin injury alone
- Return-to-sport criteria (>80% limb symmetry, >90% adductor:abductor ratio) adds clinical specificity
- The five pain dimensions table and mechanism-based pain classification (nociceptive/neuropathic/nociplastic) is the theoretical backbone
- Central Sensitization Inventory (CSI) + Conditioned Pain Modulation (CPM) demonstrates advanced neuroscience knowledge
- Citing four systematic reviews on PNE (2023-2025) as a cluster is strong
- Nociplastic pain (IASP 2021) taxonomy is the most contemporary concept
- The Coppieters & Butler (2008) slider vs. tensioner analysis is foundational - must be cited
- Structural differentiation explained with an example demonstrates true understanding
- The clinical decision algorithm (irritability → technique selection) shows clinical reasoning
- Contraindications and precautions are frequently missed but earn marks