Types of dieabites mellitus and normal range of blood glucose
Reading File
Finding Sources
Searching the Web
types of diabetes mellitus classification blood glucose normal range 2024
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have excellent, comprehensive information from the medical textbooks. Let me compile the full answer.
Diabetes Mellitus: Types and Blood Glucose Reference Ranges
Classification of Diabetes Mellitus
Per the American Diabetes Association (ADA) classification (as cited in Tietz Textbook of Laboratory Medicine, 7th Ed. and Creasy & Resnik's Maternal-Fetal Medicine), diabetes mellitus is divided into four main clinical categories:
1. Type 1 Diabetes Mellitus (T1DM)
- Cause: Autoimmune destruction of pancreatic beta cells in the islets of Langerhans, leading to absolute insulin deficiency
- Sub-types:
- Immune-mediated (most common) - autoantibodies present (against islet cells, insulin, GAD65, tyrosine phosphatase IA-2)
- Idiopathic - no autoantibodies found
- Epidemiology: Accounts for ~5-10% of all diabetes cases; peak onset in childhood/adolescence (~75% before age 18), but can occur at any age
- Presentation: Abrupt onset of polyuria, polydipsia, rapid weight loss; ~30% present with diabetic ketoacidosis (DKA)
- Three stages:
- Stage 1: Normoglycemic but multiple islet autoantibodies present
- Stage 2: Dysglycemia (IFG/IGT) with autoantibodies
- Stage 3: Clinical diabetes with symptoms
2. Type 2 Diabetes Mellitus (T2DM)
- Cause: Progressive loss of beta cell insulin secretion, frequently on the background of insulin resistance
- Epidemiology: Most common type; strongly linked to obesity, sedentary lifestyle, age, and genetic predisposition
- Onset: Usually gradual; often diagnosed incidentally on routine screening
- Key feature: Relative (not absolute) insulin deficiency; patients may not require insulin initially
3. Gestational Diabetes Mellitus (GDM)
- Definition: Diabetes first diagnosed during pregnancy that was not clearly overt diabetes before gestation
- Prevalence: Occurs in approximately 6-8% of pregnancies in the US (~270,000 cases/year); 15.8% of live births worldwide are affected by hyperglycemia in pregnancy
- Risk: Women with GDM have a 30-67% lifetime risk of subsequently developing T2DM
- Postpartum: All GDM patients should be evaluated at 4-12 weeks postpartum and screened at least every 3 years thereafter
4. Other Specific Types of Diabetes
These result from identifiable, specific causes (Box 47.2, Tietz Textbook of Laboratory Medicine):
| Sub-category | Examples |
|---|---|
| A. Genetic defects of beta-cell function | MODY (Maturity-Onset Diabetes of the Young), neonatal diabetes |
| B. Genetic defects in insulin action | Type A insulin resistance, leprechaunism |
| C. Diseases of the exocrine pancreas | Chronic pancreatitis, cystic fibrosis, pancreatectomy, pancreatic cancer |
| D. Endocrinopathies | Cushing's syndrome, acromegaly, glucagonoma, pheochromocytoma |
| E. Drug or chemical-induced | Glucocorticoids, HIV/AIDS treatment, post-organ transplant immunosuppression |
| F. Infections | Congenital rubella, cytomegalovirus |
| G. Uncommon immune-mediated forms | Stiff-man syndrome, anti-insulin receptor antibodies |
| H. Other genetic syndromes | Down syndrome, Turner syndrome, Wolfram syndrome |
Blood Glucose Reference Ranges
(Based on ADA diagnostic criteria, as cited in Tietz Textbook of Laboratory Medicine, 7th Ed.)
Normal (Euglycemia)
| Test | Normal Value |
|---|---|
| Fasting Plasma Glucose (FPG) | < 100 mg/dL (< 5.6 mmol/L) |
| 2-hr Plasma Glucose (OGTT) | < 140 mg/dL (< 7.8 mmol/L) |
| HbA1c | < 5.7% |
| Random Plasma Glucose | No specific cutoff; typically < 140 mg/dL |
Prediabetes (Increased Risk for Diabetes)
| Category | Test | Value |
|---|---|---|
| Impaired Fasting Glucose (IFG) | FPG | 100-125 mg/dL (5.6-6.9 mmol/L) |
| Impaired Glucose Tolerance (IGT) | 2-hr OGTT | 140-199 mg/dL (7.8-11.0 mmol/L) |
| Prediabetes | HbA1c | 5.7%-6.4% |
Note: The WHO and some other organizations use a slightly higher IFG lower cutoff of 110 mg/dL (6.1 mmol/L).
Diabetes Mellitus (Diagnostic Thresholds)
Any one of the following criteria is sufficient for diagnosis:
| Test | Diabetic Value |
|---|---|
| Fasting Plasma Glucose (FPG) | ≥ 126 mg/dL (≥ 7.0 mmol/L) |
| 2-hr Plasma Glucose (75g OGTT) | ≥ 200 mg/dL (≥ 11.1 mmol/L) |
| HbA1c | ≥ 6.5% |
| Random Plasma Glucose | ≥ 200 mg/dL (≥ 11.1 mmol/L) with classic hyperglycemic symptoms |
Summary Table
| Category | FPG (mg/dL) | 2-hr OGTT (mg/dL) | HbA1c (%) |
|---|---|---|---|
| Normal | < 100 | < 140 | < 5.7 |
| Prediabetes | 100-125 | 140-199 | 5.7-6.4 |
| Diabetes | ≥ 126 | ≥ 200 | ≥ 6.5 |
Sources:
- Tietz Textbook of Laboratory Medicine, 7th Edition (Box 47.2; Classification and Diagnostic Criteria)
- Creasy & Resnik's Maternal-Fetal Medicine (ADA Classification of DM, 4 clinical types)
- ADA Standards of Care in Diabetes 2024 (PMC article)
What is diabetes mellitus? What are the types of diabetes mellitus and the normal range of blood glucose?
Reading File
Finding Sources
Finding Sources
Searching the Web
diabetes mellitus definition pathophysiology types ADA 2024
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive, textbook-sourced answer. Here it is:
Diabetes Mellitus
What Is Diabetes Mellitus?
Diabetes mellitus is a common chronic metabolic disorder characterized by elevated blood glucose concentrations (hyperglycemia). It results from defects in insulin secretion, insulin action, or both. Without adequate insulin, cells cannot take up glucose from the blood, forcing the body to mobilize alternative fuels - amino acids from muscle and free fatty acids from adipose tissue - which are converted by the liver into glucose and ketones, worsening hyperglycemia further.
"Diabetes mellitus is a common chronic metabolic disorder that is characterized by elevated blood glucose concentrations."
- Goldman-Cecil Medicine, International Edition
Pathophysiology of Insulin Deficiency
The diagram below illustrates what happens when insulin is deficient:
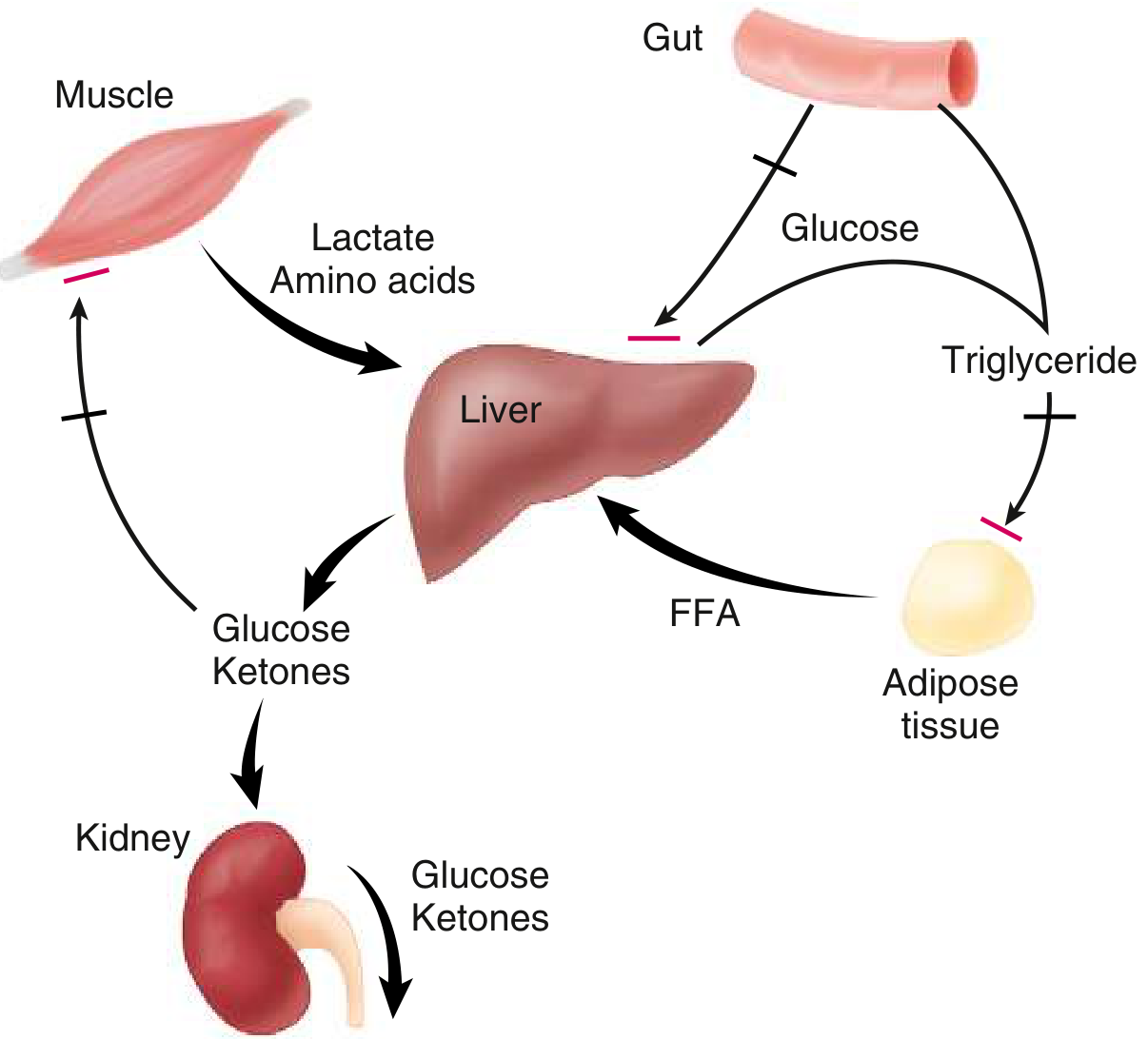
Figure: In insulin deficiency, muscle breaks down to lactate and amino acids, adipose tissue releases free fatty acids (FFA), and the liver converts these into glucose and ketones. The kidney then spills these into urine, causing polyuria, polydipsia, and weight loss. (Goldman-Cecil Medicine)
Classic Symptoms ("The 3 Polys + weight loss")
- Polyuria - frequent, excessive urination (osmotic diuresis from glucosuria)
- Polydipsia - excessive thirst (secondary to polyuria)
- Polyphagia - excessive hunger
- Unexplained weight loss
Complications of Chronic Hyperglycemia
| Type | Examples |
|---|---|
| Microvascular | Retinopathy, Nephropathy, Neuropathy |
| Macrovascular | Coronary artery disease, Peripheral vascular disease, Stroke |
| Acute, life-threatening | Diabetic ketoacidosis (DKA), Hyperglycemic hyperosmolar state (HHS), Hypoglycemia |
Types (Classification) of Diabetes Mellitus
Per the American Diabetes Association (ADA) classification, there are 4 main clinical types (Tietz Textbook of Laboratory Medicine, 7th Ed.; Creasy & Resnik's Maternal-Fetal Medicine):
Type 1 — Type 1 Diabetes Mellitus (T1DM)
- Mechanism: Autoimmune destruction of pancreatic beta cells → absolute insulin deficiency
- Sub-types:
- Immune-mediated (most common): autoantibodies present - against islet cells, insulin, GAD65, tyrosine phosphatase IA-2
- Idiopathic: no autoantibodies detected
- Who: ~5-10% of all diabetes cases; typically children/adolescents (~75% onset before age 18), but can occur at any age
- Onset: Abrupt - polyuria, polydipsia, rapid weight loss; ~30% present with DKA
- Treatment: Insulin replacement is mandatory for survival
Three Stages of T1DM:
| Stage | Features |
|---|---|
| Stage 1 | Normoglycemic but multiple islet autoantibodies present |
| Stage 2 | Dysglycemia (IFG/IGT) with autoantibodies, no symptoms |
| Stage 3 | Clinical diabetes with overt hyperglycemia and symptoms |
Type 2 — Type 2 Diabetes Mellitus (T2DM)
- Mechanism: Progressive loss of beta cell insulin secretion + insulin resistance (relative insulin deficiency)
- Who: Most common type (~85-90% of all cases); linked to obesity, physical inactivity, aging, and family history
- Onset: Gradual, often silent; diagnosed incidentally on routine testing
- Risk factors: Obesity (especially central/abdominal), sedentary lifestyle, age >45, family history, history of GDM
- Treatment: Lifestyle modification, oral hypoglycemic agents, GLP-1 agonists, and/or insulin in later stages
Type 3 — Gestational Diabetes Mellitus (GDM)
- Definition: Diabetes first diagnosed during pregnancy that was not clearly overt before gestation
- Prevalence: 6-8% of pregnancies in the US (~270,000 cases/year); globally, 15.8% of live births are affected by hyperglycemia in pregnancy
- Risk: Women with GDM have a 30-67% lifetime risk of developing T2DM
- Follow-up: All GDM patients should be evaluated at 4-12 weeks postpartum and screened at least every 3 years thereafter
Type 4 — Other Specific Types of Diabetes
Caused by identifiable conditions:
| Sub-category | Examples |
|---|---|
| A. Genetic defects of beta-cell function | MODY (Maturity-Onset Diabetes of the Young), neonatal diabetes |
| B. Genetic defects in insulin action | Type A insulin resistance, leprechaunism |
| C. Diseases of the exocrine pancreas | Chronic pancreatitis, cystic fibrosis, pancreatectomy, pancreatic cancer |
| D. Endocrinopathies | Cushing's syndrome, acromegaly, glucagonoma, pheochromocytoma, hyperthyroidism |
| E. Drug or chemical-induced | Glucocorticoids, HIV treatment, post-transplant immunosuppression, thiazides |
| F. Infections | Congenital rubella, cytomegalovirus |
| G. Uncommon immune-mediated forms | Stiff-man syndrome, anti-insulin receptor antibodies |
| H. Other genetic syndromes | Down syndrome, Turner syndrome, Wolfram syndrome, Klinefelter syndrome |
Blood Glucose Reference Ranges
(ADA Diagnostic Criteria, as cited in Tietz Textbook of Laboratory Medicine, 7th Ed. and ADA Standards of Care 2024)
At a Glance
| Category | Fasting Plasma Glucose | 2-hr OGTT (75g) | HbA1c |
|---|---|---|---|
| Normal | < 100 mg/dL (< 5.6 mmol/L) | < 140 mg/dL (< 7.8 mmol/L) | < 5.7% |
| Prediabetes | 100-125 mg/dL (5.6-6.9 mmol/L) | 140-199 mg/dL (7.8-11.0 mmol/L) | 5.7-6.4% |
| Diabetes | ≥ 126 mg/dL (≥ 7.0 mmol/L) | ≥ 200 mg/dL (≥ 11.1 mmol/L) | ≥ 6.5% |
Prediabetes (Intermediate Categories)
- Impaired Fasting Glucose (IFG): FPG of 100-125 mg/dL (5.6-6.9 mmol/L)
- Impaired Glucose Tolerance (IGT): 2-hr OGTT of 140-199 mg/dL (7.8-11.0 mmol/L)
- HbA1c 5.7-6.4% = prediabetes
Note: The WHO uses a slightly higher lower cutoff for IFG at 110 mg/dL (6.1 mmol/L), while the ADA uses 100 mg/dL.
Diagnosing Diabetes
Any one of the following is sufficient:
- FPG ≥ 126 mg/dL (7.0 mmol/L) - fasting = no caloric intake for at least 8 hours
- 2-hr plasma glucose ≥ 200 mg/dL (11.1 mmol/L) during 75g OGTT
- HbA1c ≥ 6.5%
- Random plasma glucose ≥ 200 mg/dL (11.1 mmol/L) with classic hyperglycemic symptoms
In the absence of unequivocal hyperglycemia, criteria 1-3 should be confirmed by repeat testing.
Sources:
- Goldman-Cecil Medicine, International Edition - Definition and pathophysiology
- Tietz Textbook of Laboratory Medicine, 7th Ed. - Classification (Box 47.2) and diagnostic criteria
- Creasy & Resnik's Maternal-Fetal Medicine - ADA 4-type classification
- ADA Standards of Care in Diabetes 2024 - Current diagnostic thresholds
This is a shared conversation. Sign in to Orris to start your own chat.