Contracture related sx
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Excellent - I now have comprehensive data. Let me compile the full answer on contracture-related surgeries (sx).
Contracture-Related Surgeries (Sx)
Based on Campbell's Operative Orthopaedics 15th Ed 2026, here is a comprehensive overview of surgical procedures for contractures by anatomical region.
General Principles
- Simple fasciotomies correct only minor contractures; recurrence is common and they cannot correct severe contractures.
- Progressive correction using traction/splinting may be used before surgery to reduce the extent of operation and after surgery to increase correction.
- Once a contracture is corrected, the correction must be actively maintained, or it recurs.
- Surgery is indicated when the contracture interferes with function, hygiene, bracing, or ambulation.
1. Shoulder - Internal Rotation Contracture
Indication: Painful, fixed internal rotation contracture unresponsive to conservative care. In comparison studies, 10/13 treated patients showed significant improvement vs. 0/12 controls.
Surgical options:
-
Release of Internal Rotation Contracture (eTechnique 35.6):
- Anterior deltopectoral approach
- Identify and excise the subscapularis tendon (preserve the anterior capsule)
- Release the pectoralis major tendinous insertion with scissors passed distally along the humerus
- Postop: sling for comfort; ROM exercises within first few days; pulley exercises by day 5
-
Fractional Lengthening (eTechnique 35.7): Pectoralis major, latissimus dorsi, teres major
- Deltopectoral approach in beach-chair position
- Tendon divided at the musculotendinous junction
- Long head of triceps can also be lengthened if elbow extension correction is needed
Note: Contracture of the shoulder from cerebral palsy is usually not disabling enough to justify surgery. When it is, pectoralis major release alone or combined with latissimus dorsi release can improve axillary hygiene.
2. Elbow - Flexion Contracture
Indication: Fixed contracture ≥45 degrees interfering with forward reach in a patient with functional hand.
Release of Elbow Flexion Contracture (Technique 35.15):
- S-shaped incision over the antecubital flexor crease
- Expose and resect the lacertus fibrosus
- Identify and protect the lateral antebrachial cutaneous nerve
- Z-plasty lengthening of the biceps tendon
- Circumferential incision of the aponeurotic brachialis fibers distally
- Anterior elbow capsulotomy if needed
- Repair the biceps tendon; close subcutaneous tissue and skin
- Cast in maximum (not forceful) extension with forearm supinated; bivalve cast
Postop: Elevate arm 48 h; finger motion from day 1; elbow flexion-extension exercises from day 5; nighttime splinting for 6 months. Maximum extension achieved 3-5 months postop.
Caution: Acute full extension must be avoided to prevent stretch injury to the brachial artery and median nerve, which have also shortened.
3. Forearm - Pronation Contracture
Indication: Fixed pronation contracture due to supinator/pronator imbalance (poliomyelitis, CP). Correction alone if pronator teres not strong enough to transfer; if pronators and wrist flexors are active, combined with FCU transfer.
Rerouting of Biceps Tendon - Zancolli (eTechnique 36.29):
- If full passive pronation not yet possible: longitudinal incision on dorsum of forearm over radial shaft, divide the interosseous membrane
- Then detach and reroute the biceps tendon to convert it from a supinator to a neutral or pronating force
For fixed supination deformity:
- Rerouting of biceps tendon (Zancolli)
- Manual osteoclasia of middle thirds of radius and ulna (Blount) - for children <12 years with insufficient muscle power for tendon transfer
4. Hip Contractures
Flexion, Abduction, and External Rotation Contracture
Ober-Yount Procedure (Complete Release - eTechnique 36.18):
- Lateral position; transverse incision medial and distal to the anterior superior iliac spine
- Divide and excise 1 cm of the iliopsoas tendon distally
- Detach sartorius from ASIS; detach rectus femoris from AIIS
- Divide the tensor fasciae latae from its anterior border completely posteriorly
- For severe deformities: Campbell technique - complete release of all muscles from the iliac wing with transfer of the crest of the ilium
Iliotibial Band (ITB) Contracture - Deformities caused:
| Deformity | Mechanism |
|---|---|
| Flexion, abduction, external rotation of hip | ITB lies lateral and anterior to hip; contracture causes these |
| Genu valgum + knee flexion contracture | ITB acts as bowstring, gradually abducts and flexes tibia |
| Limb-length discrepancy | Related to neurologic/muscle dysfunction |
| External tibial torsion ± knee subluxation | Lateral attachment rotates tibia/fibula externally |
Abduction Contracture
Fascial Release (Technique 36.8):
- Incise skin along anterior 2/3 of iliac crest to ASIS
- Divide all thigh fascial/tendinous structures anterolaterally: fascia lata, gluteus medius/minimus fascia, tensor fasciae latae
- Fasciotomy of fascia lata distally (Yount) may also be required
- Hip spica cast in neutral abduction; removed at 2 weeks to begin ROM
Adduction Contracture
- Indicated when causing pelvic obliquity or interfering with sitting/walking
- Adductor Release (Technique 35.2)
5. Knee Contractures (Myelomeningocele)
Flexion Contracture
- 20-degree contractures at birth: mostly spontaneously correct
- >20 degrees + interferes with bracing/ambulation: surgical correction indicated
- Hamstring lengthening ± posterior capsular release: for 20-30 degree contractures in children walking with below-knee orthoses
- Supracondylar extension osteotomy of the femur: for >30-45 degree contractures in older community-walking children (after failed hamstring release)
- Anterior distal femoral hemiepiphysiodesis: newer effective method for growing children
Extension Contracture
- Less common than flexion
- May require quadriceps lengthening or V-Y plasty
6. Equinus Contracture (Ankle/Foot)
- Percutaneous Achilles tendon lengthening: for mild/moderate contractures
- Open Achilles tendon lengthening: for severe contractures; may also require lengthening/release of posterior tibial, flexor digitorum longus, and flexor hallucis longus tendons
- Post-correction: ankle-foot orthosis (AFO) required to maintain correction and allow ambulation
- In Duchenne muscular dystrophy: release may allow 2-3 more years of ambulation, but by age 12-13 most can no longer walk regardless
7. Volkmann Ischemic Contracture (Forearm)
Arises from untreated or inadequately treated compartment syndrome. Classic deformity: elbow flexion, forearm pronation, wrist flexion, thumb adduction, MCP extension, finger flexion.
| Severity | Features | Surgical Treatment |
|---|---|---|
| Mild (localized) | 2-3 fingers flexed, no sensory loss, no intrinsic contracture | Dynamic splinting first; after 3 months - muscle-tendon lengthening or muscle sliding operation |
| Moderate | FPL + wrist flexors involved; median/ulnar nerve sensory changes; intrinsic minus deformity | Muscle sliding operation + neurolysis of median/ulnar nerves + excision of fibrotic muscle |
| Severe | No useful finger flexor movement | Volar transfer of dorsal wrist extensors (brachioradialis, ECRL) + complete release of wrist and finger flexors |
Muscle Sliding Operation (for established Volkmann's):
- Detaches the origin of the flexor mass from the medial epicondyle and slides it distally
- Allows passive extension of fingers without tendon rupture
- Appropriate for mild-moderate cases
8. Dupuytren's Contracture (Hand)
Indications: PIP joint contracture ≥15 degrees OR MCP joint contracture ≥30 degrees causing disability. Timing matters - surgery ideally done when disease tissue is mature (lower recurrence risk).
Operative options (Box 80.3):
| Procedure | Use |
|---|---|
| Percutaneous needle aponeurotomy (PNA) | Subcutaneous cord division; least invasive; higher recurrence |
| Enzymatic aponeurotomy (collagenase Clostridium histolyticum) | Non-surgical cord lysis; outpatient |
| Partial (selective) fasciectomy | Most common surgical procedure; excises diseased fascia |
| Complete fasciectomy | Rarely done; higher morbidity |
| Fasciectomy + skin grafting | For severe skin involvement |
| Staged resection preceded by external fixation | Severe contractures with skin shortage |
| Joint resection and arthrodesis | Fixed joint contracture not correctable |
| Amputation | Last resort for severe, recurrent disease |
Key points:
- Appropriate procedure depends on: degree of contracture, palmar skin nutritional status, bony deformities, patient's age/occupation/general health
- More severe involvement requires more extensive surgery, done in stages if necessary
- Subcutaneous fasciotomy + joint extension therapy may precede definitive surgery for severe cases
9. Metacarpophalangeal Joint Capsulotomy (Hand)
Indication: Joint motion limited by secondary collateral ligament contracture.
Contraindication: When MCP joint motion is only 60 degrees (only 60-70 degrees expected after surgery).
Technique 72.28:
- Longitudinal incision 2.5 cm long over affected joint
- For multiple joints: second and fourth web space dorsal longitudinal incisions can release all four MCP joints
- Incise extensor hood dorsolaterally and dorsomedially (0.5 cm from tendon)
- Retract extensor hood and intrinsic tendons palmarward
- Longitudinal incision through dorsal capsule to expose metacarpal head
- Transect and remove dorsal joint capsule; excise portions of collateral ligaments sequentially to gain passive flexion (taking care not to destabilize joint)
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, blocks 14, 15, 37, 40
Images of contracture and reased sx
Finding Sources
Searching Content
"cdn.orris.care" in /textbooks/9780443117633
Searching Content
"cdn.orris.care" in /textbooks/9780443117633
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the images. Here is the comprehensive visual guide to contracture-related surgeries:
Images: Contracture-Related Surgeries
(Campbell's Operative Orthopaedics 15th Ed 2026)
1. Volkmann Ischemic Contracture - Forearm Anatomy
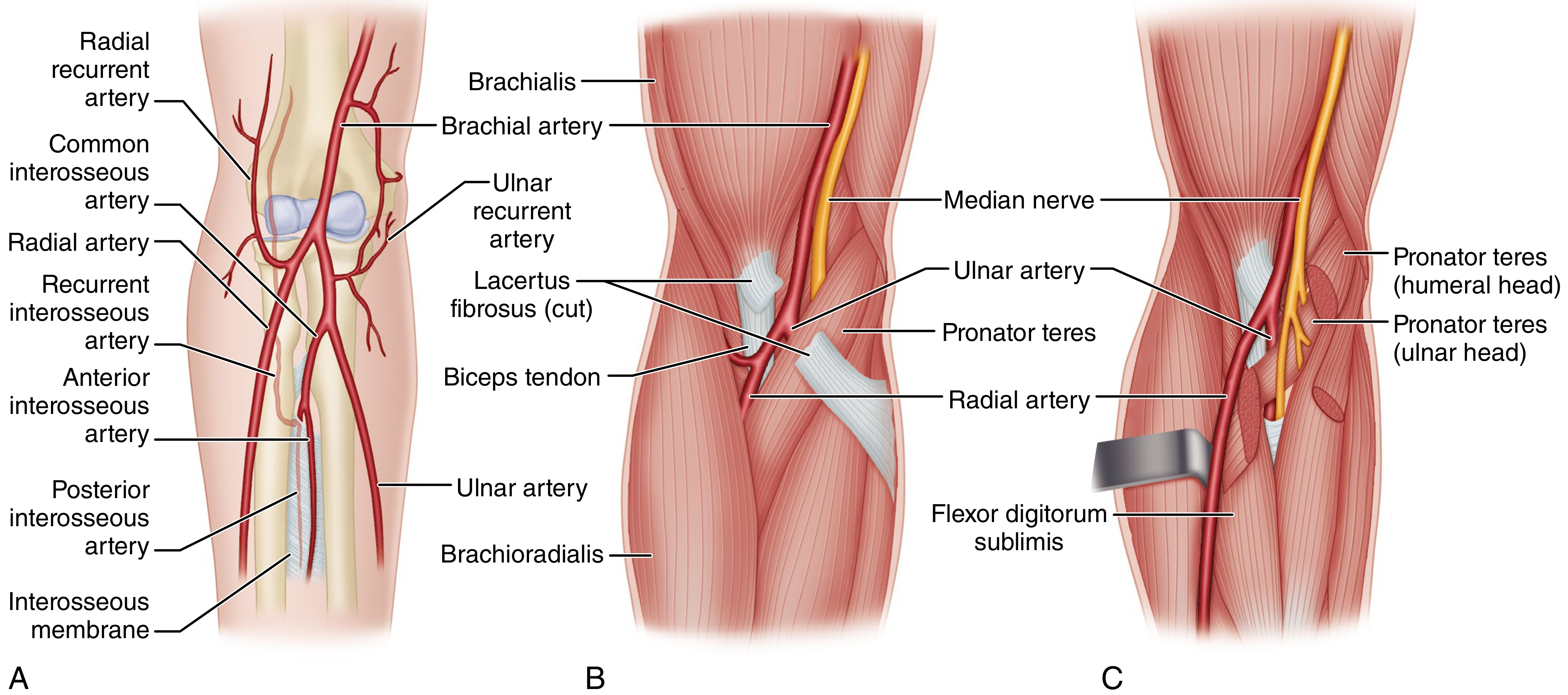
Fig 79.10 - Anatomy of Volkmann ischemia. (A) Elbow collateral circulation - does not communicate with vessels within the flexor compartment; they join the radial and ulnar arteries proximal to the pronator teres. (B) Brachial artery and median nerve enter the forearm through the tight opening formed by the biceps tendon (lateral) and pronator teres (medial), covered by the lacertus fibrosus - compression here causes Volkmann's. (C) Radial artery runs superficial to all flexor muscles; ulnar artery passes beneath pronator teres; median nerve passes between humeral and ulnar heads of pronator teres and is then compressed against the arcuate band of the flexor sublimis origin.
2. Elbow Contracture Release - Surgical Approach (Morrey)
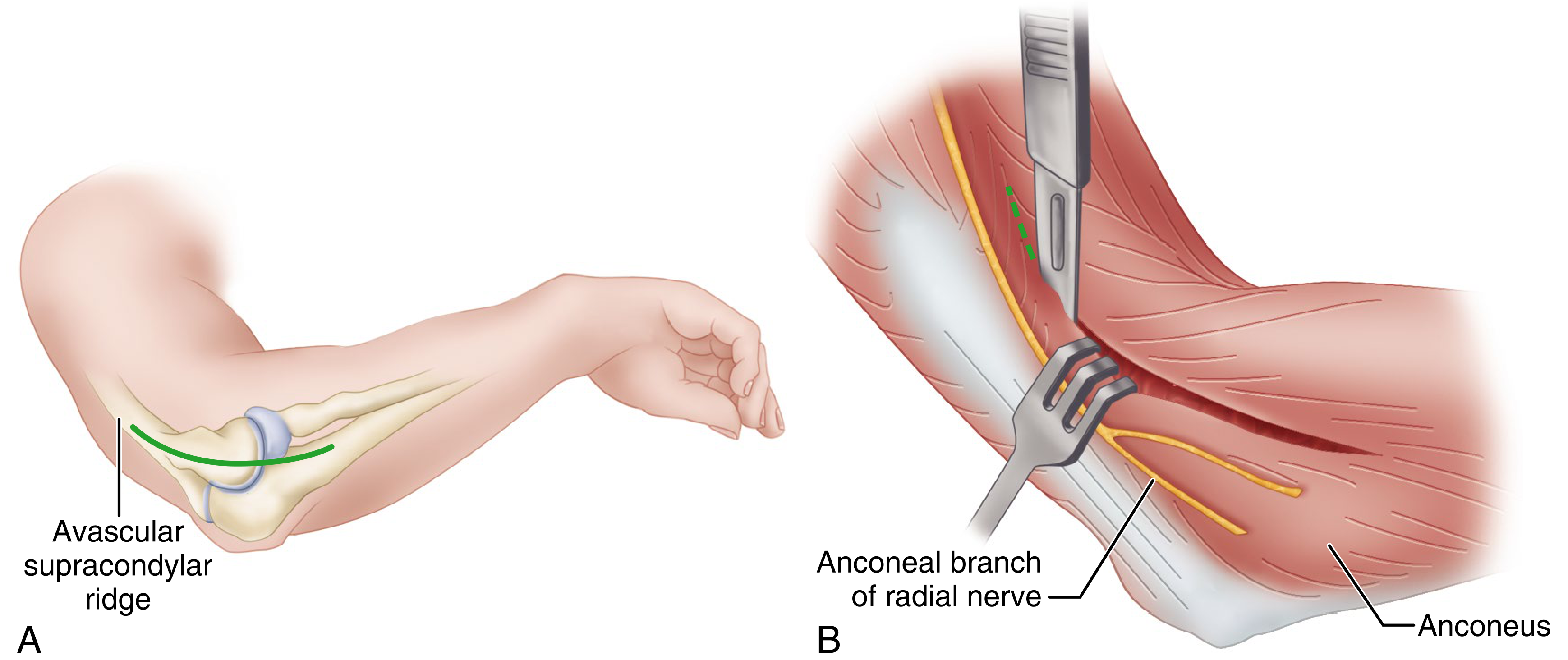
Fig 51.39 - Open anterior and posterior elbow contracture release.
- (A) Extended Kocher approach - 15 cm incision along the supracondylar ridge down to the lateral epicondyle, ending over the subcutaneous border of the ulna.
- (B) Deep dissection: brachialis elevated off the anterior joint capsule; retractors placed deep to brachioradialis and brachialis. The anconeal branch of the radial nerve is identified and protected. Green dashed line = incision line for anterior capsulectomy (from lateral to medial, preserving the lateral collateral ligament).
3. Percutaneous Needle Aponeurotomy (PNA) - Dupuytren's Contracture
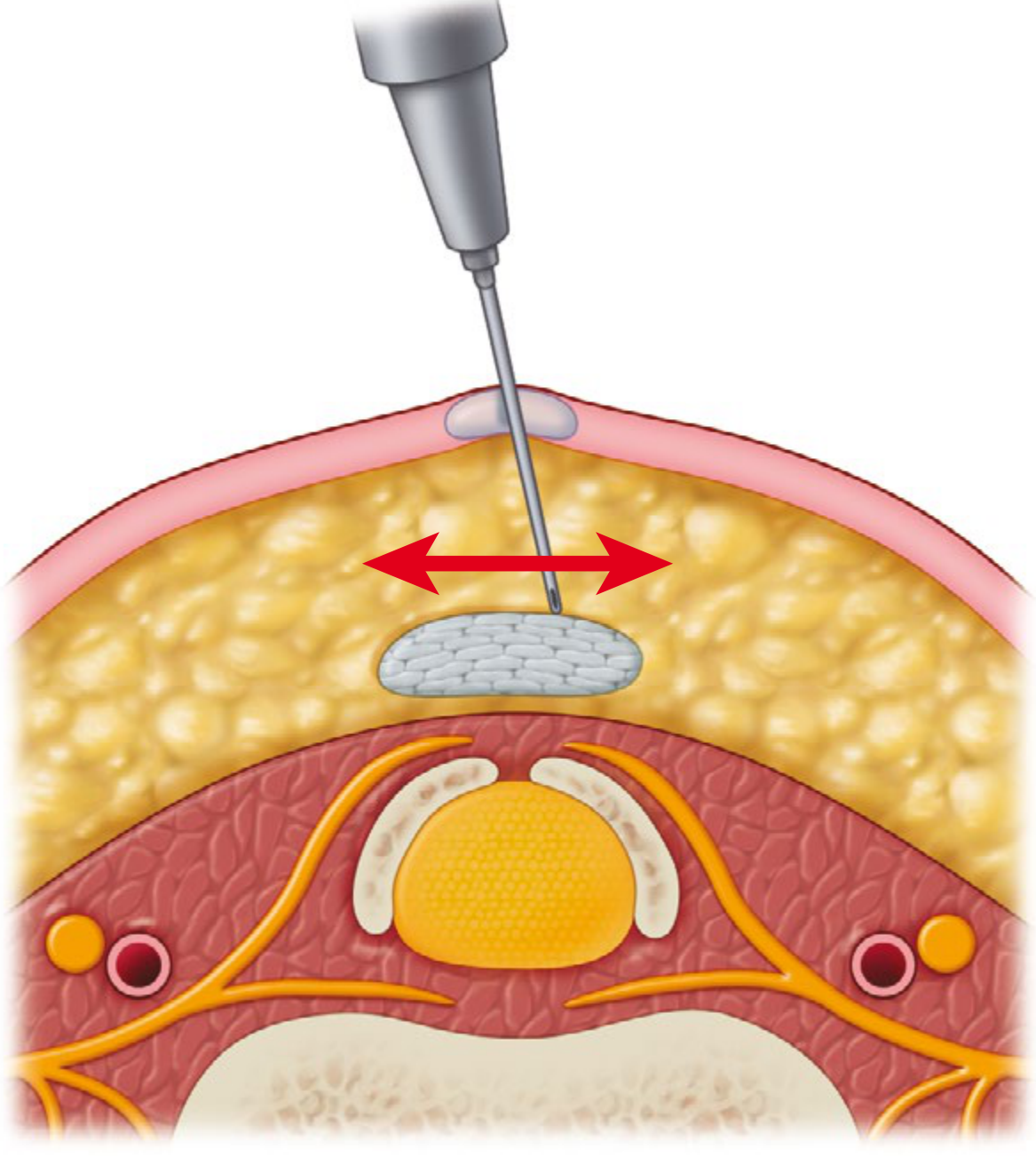
Fig 80.11 - Cross-section diagram of Percutaneous Needle Aponeurotomy maneuver for Dupuytren's contracture:
- Needle inserted percutaneously through the skin
- Side-to-side sweeping maneuver (red arrows) releases the cord from superficial to deep
- Key layers visible: skin (pink), subcutaneous fat (yellow), Dupuytren's cord (grey/white ovoid), neurovascular bundles (orange), flexor tendon (central white), and underlying bone
4. Dupuytren's Contracture - Decision Algorithm for Surgery
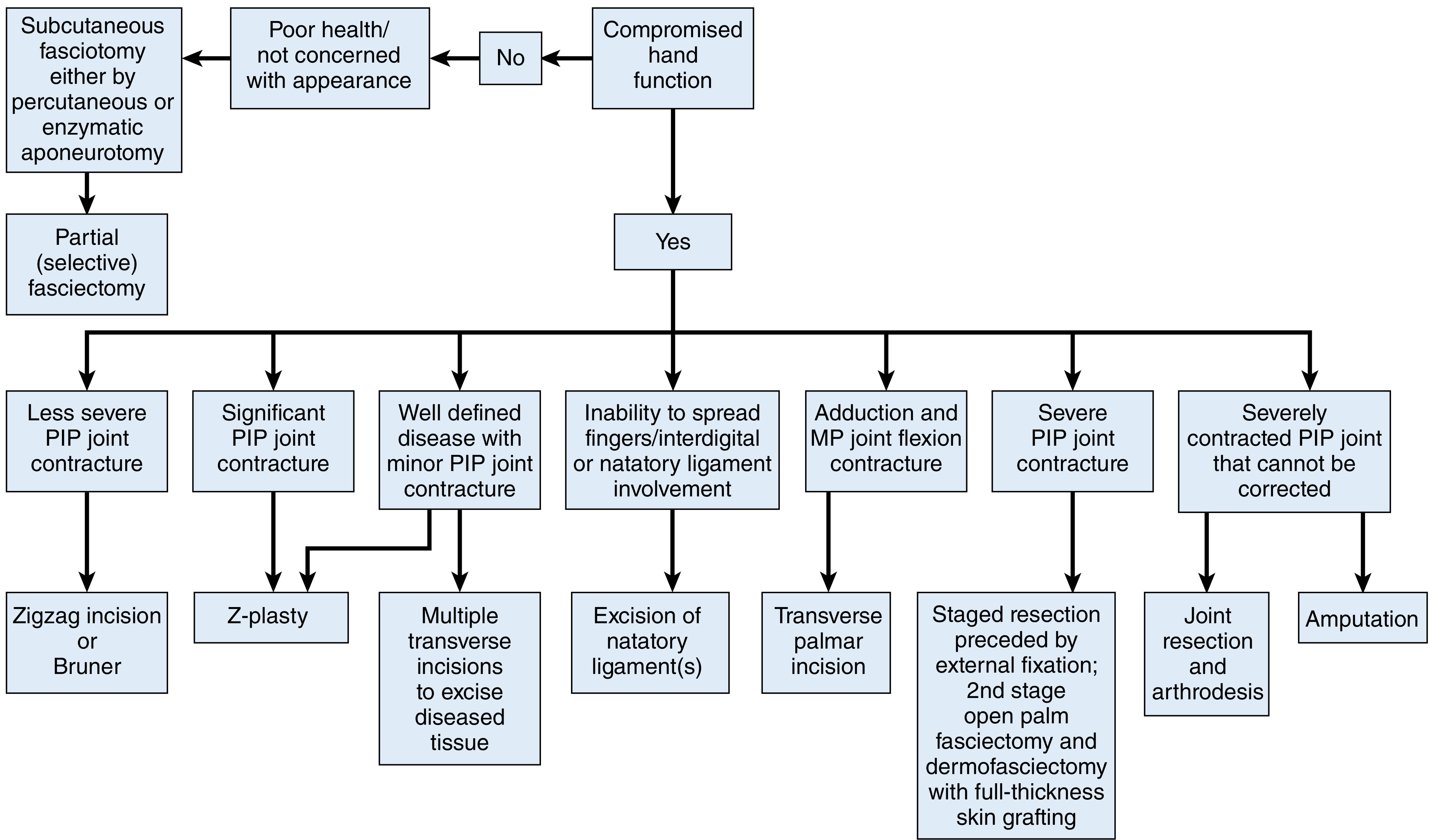
Fig 80.12 - Decision algorithm for surgical treatment of Dupuytren disease:
- Poor health / not concerned with appearance → Subcutaneous fasciotomy (percutaneous or enzymatic aponeurotomy) → Partial (selective) fasciectomy
- Compromised hand function (Yes) → multiple branches based on pattern:
- Less severe PIP contracture → Zigzag (Bruner) incision
- Significant PIP contracture → Z-plasty
- Well-defined disease + minor PIP contracture → Multiple transverse incisions to excise diseased tissue
- Inability to spread fingers / natatory ligament → Excision of natatory ligaments
- Adduction + MP flexion contracture → Transverse palmar incision
- Severe PIP contracture → Staged resection with external fixation + open palm fasciectomy + dermafasciectomy with full-thickness skin graft
- Severely contracted PIP that cannot be corrected → Joint resection and arthrodesis
- Last resort → Amputation
5. Dupuytren's Subcutaneous Cordotomy - Step-by-Step Intraoperative Photos
A - Pretendinous cord visible with 60° MP contracture:

Well-defined pretendinous Dupuytren cord in the ring finger with 60-degree metacarpophalangeal joint contracture. A No. 15 scalpel blade is positioned to be inserted between skin and cord.
B - Scalpel blade inserted between skin and pretendinous cord:
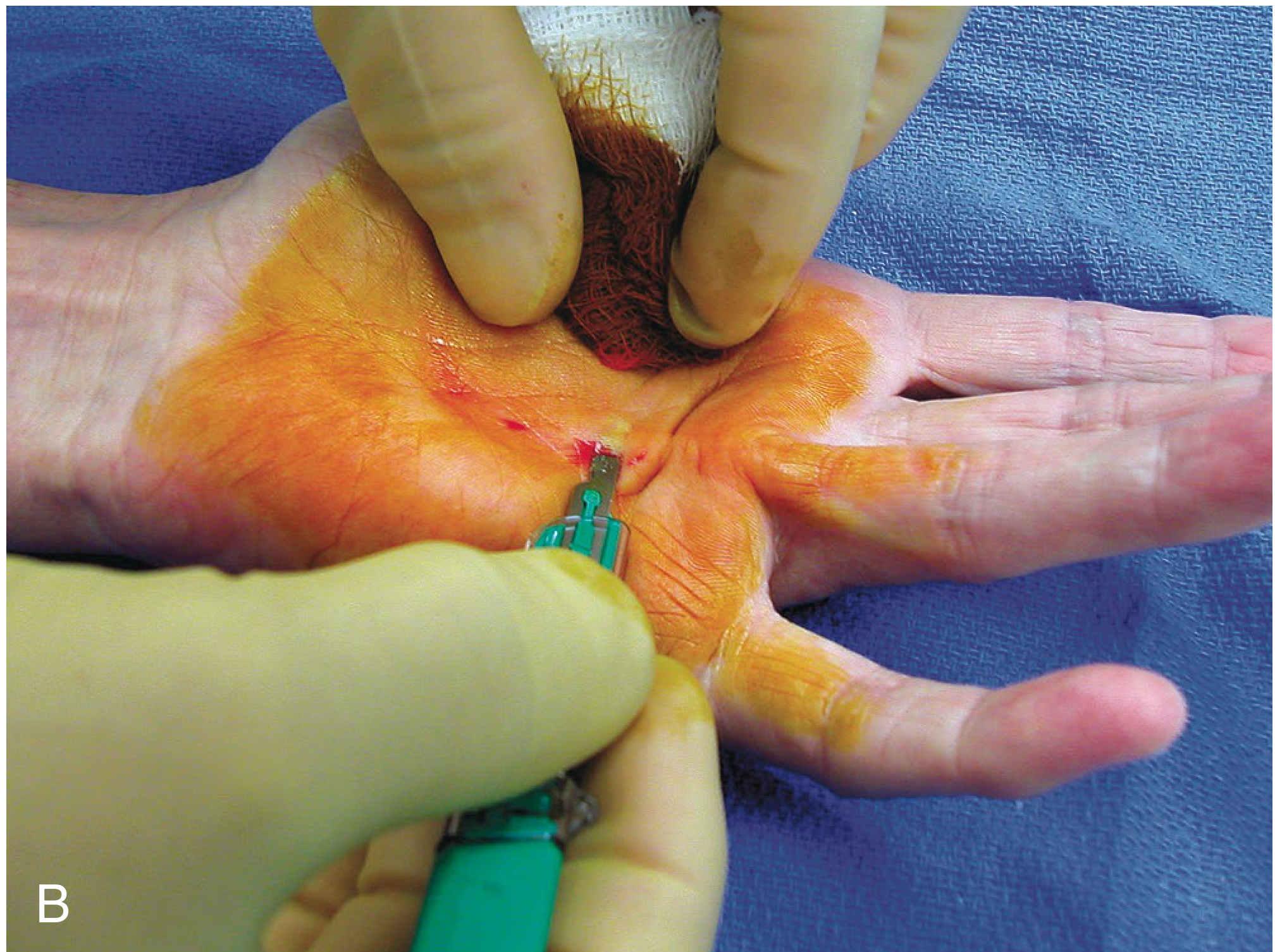
No. 15 scalpel blade inserted between skin and the pretendinous cord. The blade is held at 90 degrees to the tight cord.
C - Forceful extension delivers cord onto blade:
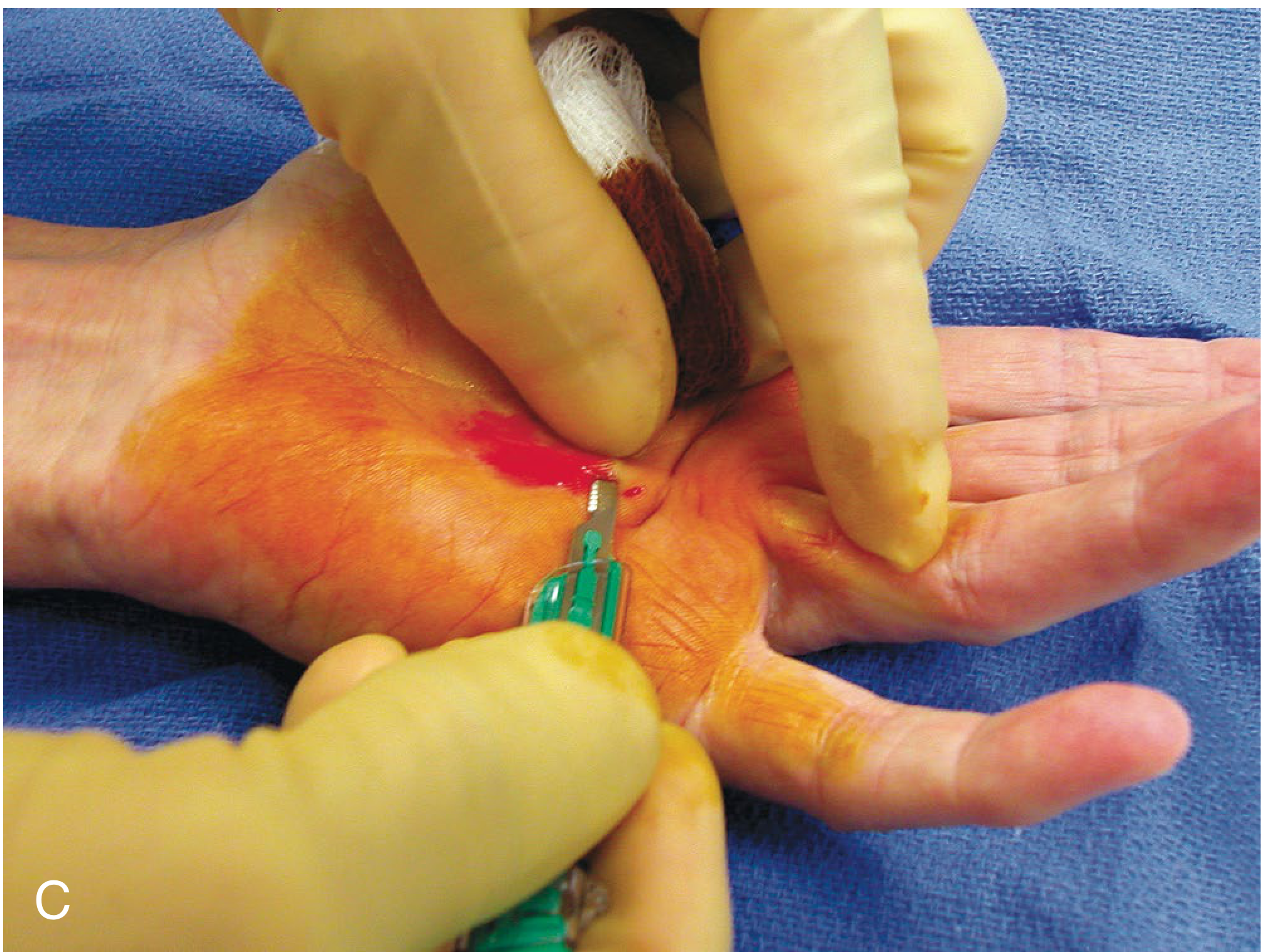
Forceful extension of the finger effectively delivers the superficially abnormal cord onto the scalpel blade, dividing it.
D - Resultant MCP extension achieved after cordotomy:

Full metacarpophalangeal joint extension achieved after cordotomy. Note the corrected finger position.
6. Luck Subcutaneous Fasciotomy - Cross-Section Diagram
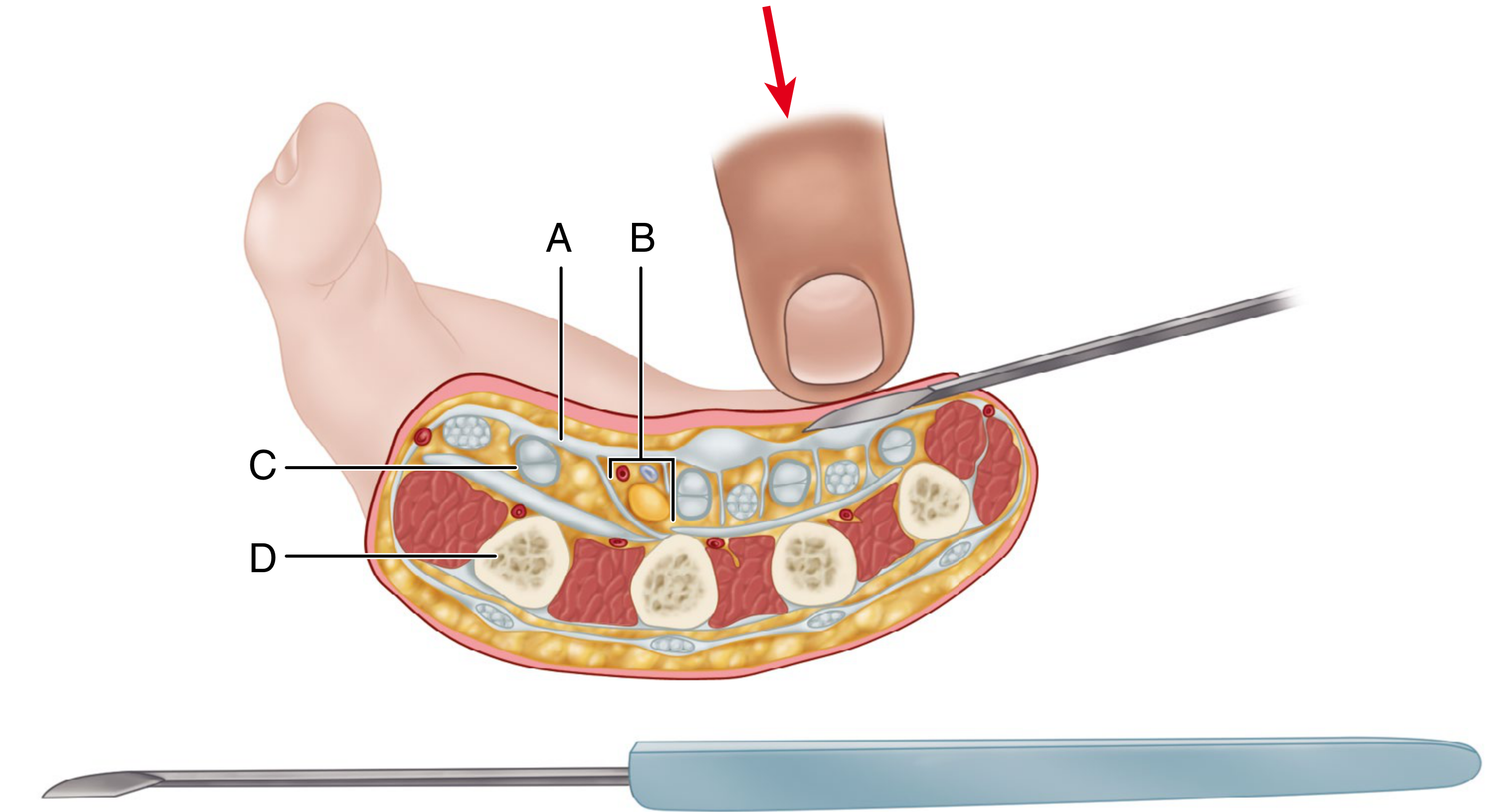
Fig 80.14 - Luck subcutaneous fasciotomy technique. Cross-section of the hand showing relations of the palmar fascia:
- (A) Palmar fascia (grey band - the target)
- (B) Neurovascular bundle (red dots)
- (C) Neurovascular bundle (labelled in diagram)
- (D) Flexor tendons (white ovals) and metacarpals (yellow)
The fasciotome (or No. 15 blade) is pressed through the palmar skin superficial to the fascia, then turned dorsally to divide the cord. Below: the Luck fasciotome instrument.
All images from Campbell's Operative Orthopaedics 15th Ed 2026 (ISBN 9780443117633)
This is a shared conversation. Sign in to Orris to start your own chat.