Write a notes on cardiac reflex for MD Anaesthesiology exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive, high-quality content from the best anaesthesia and physiology textbooks. Let me compile these into detailed, exam-oriented notes.
Cardiac Reflexes - Notes for MD Anaesthesiology
Sources: Miller's Anesthesia 10e, Barash's Clinical Anesthesia 9e, Costanzo Physiology 7e, Guyton & Hall
OVERVIEW
Cardiac reflexes are fast-acting reflex loops between the heart and the CNS that contribute to regulation of cardiac function and maintenance of physiologic homeostasis. Cardiac receptors are located in the atria, ventricles, pericardium, and coronary arteries. Extracardiac receptors are found in the great vessels and carotid artery. Afferent fibers travel along the vagus nerve (myelinated or unmyelinated). After central processing in the medulla, efferent signals provoke specific cardiovascular responses.
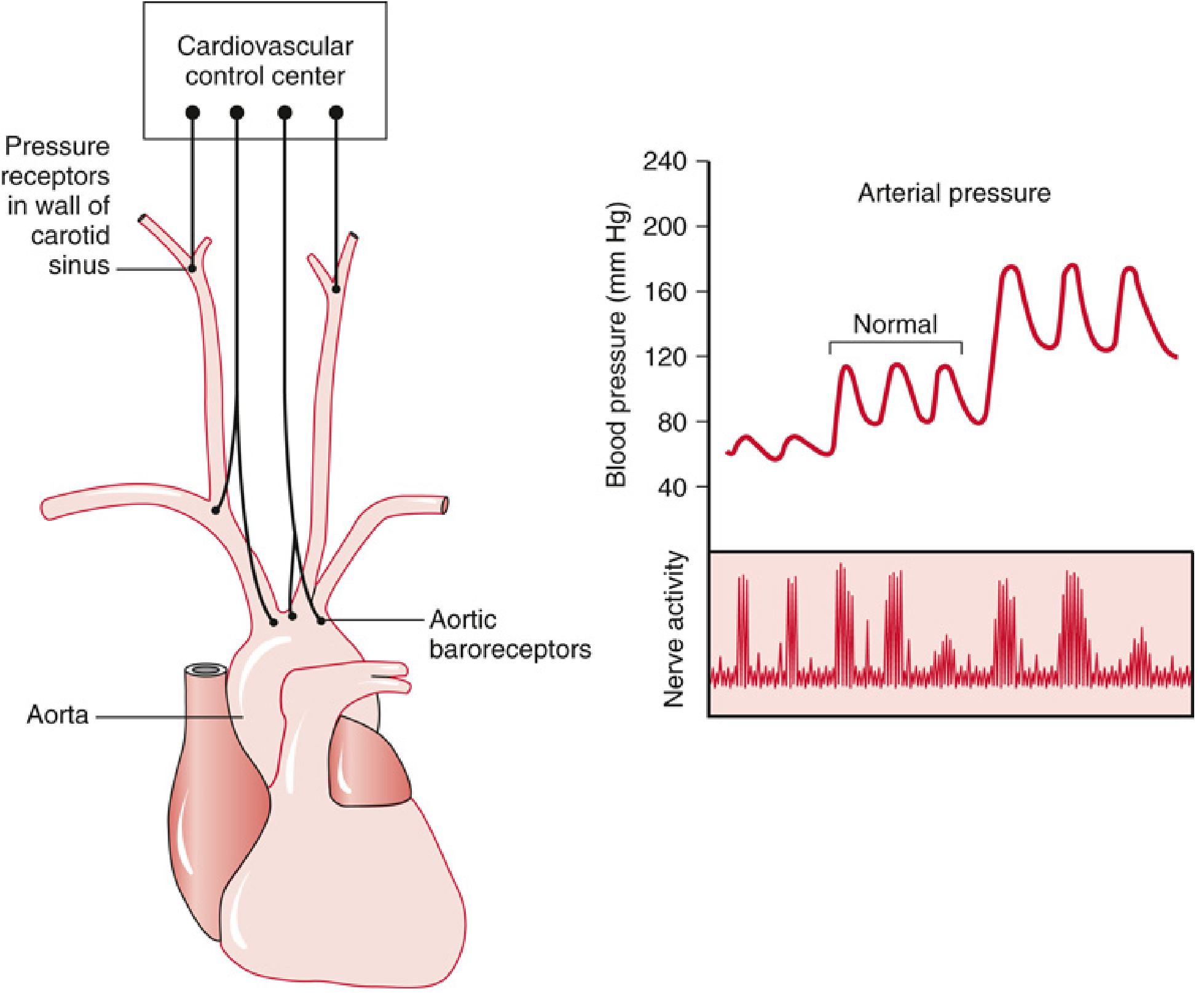
1. BARORECEPTOR REFLEX (Carotid Sinus Reflex)
Physiology
The baroreceptor reflex is the primary short-term regulator of arterial blood pressure, operating via a negative feedback loop.
Receptors:
- Located in the carotid sinus (bifurcation of common carotid artery) and aortic arch
- Mechanoreceptors sensitive to circumferential and longitudinal stretch
- Carotid sinus receptors respond to both increases AND decreases in pressure
- Aortic arch receptors respond primarily to increases in pressure
- Most sensitive to rapid changes in arterial pressure (rate of change > absolute level)
Afferent Pathway:
- Carotid sinus baroreceptors → Nerve of Hering → Glossopharyngeal nerve (CN IX)
- Aortic arch baroreceptors → Vagus nerve (CN X)
- Afferents synapse in the Nucleus Tractus Solitarius (NTS), located in the cardiovascular center of the medulla
Central Integration:
- The cardiovascular centre in the medulla has two functional areas:
- Depressor area (central/caudal): reduces BP; also integrates input from hypothalamus and limbic system
- Pressor area (lateral/rostral): increases BP
- Typical activation of stretch receptors occurs when systemic BP exceeds 170 mmHg
Efferent Response:
| Trigger | Sympathetic | Parasympathetic | Net Effect |
|---|---|---|---|
| High BP (stretch ↑) | ↓ activity | ↑ activity | ↓ HR, ↓ contractility, ↓ vascular tone |
| Low BP (stretch ↓) | ↑ activity | ↓ activity | ↑ HR, ↑ contractility, vasoconstriction |
Anaesthetic Relevance
- Acute blood loss/shock: baroreceptor reflex is beneficial (maintains BP)
- Reflex arc becomes non-functional when BP drops below 50 mmHg
- Volatile anaesthetic agents blunt the baroreceptor reflex in a dose-dependent manner
- Chronic hypertension: baroreceptors reset to a higher set point and maintain rather than correct the elevated pressure
- Sex differences (hormonal status) alter baroreceptor sensitivity
- During spinal anaesthesia - extensive sympathectomy (T5-L2) causes venous pooling; compensatory baroreceptor response above the block level triggers vasoconstriction and tachycardia, but this may be overcome at higher block levels
2. CHEMORECEPTOR REFLEX
Physiology
Receptors: Chemosensitive cells in the carotid bodies and aortic body
Stimuli:
- PaO2 < 50 mmHg (hypoxaemia)
- Acidosis (↓ pH)
Afferent Pathway:
- Sinus nerve of Hering → Glossopharyngeal nerve (CN IX) and Vagus nerve (CN X) → chemosensitive area of medulla
Response:
- Stimulates respiratory centres → ↑ ventilatory drive
- Activates parasympathetic system → ↓ HR, ↓ myocardial contractility
- With persistent hypoxia - direct CNS stimulation → ↑ sympathetic activity (overrides initial parasympathetic response)
Anaesthetic Relevance
- Hypoxia during anaesthesia may initially trigger bradycardia (parasympathetic) before sympathetic override
- Important consideration during induction in patients with severe hypoxaemia
3. BAINBRIDGE REFLEX
Physiology
Also known as the atrial reflex or tachycardia reflex.
Receptors: Stretch receptors in the right atrial wall and the cavoatrial junction
Stimulus: Increased right-sided filling pressure (↑ venous return, volume overload)
Pathway: Vagal afferent signals → cardiovascular center in medulla → inhibit parasympathetic outflow
Response:
- ↑ Heart rate (via two mechanisms):
- Inhibition of parasympathetic (vagal) activity
- Direct effect on SA node via atrial stretch
Important: The magnitude and direction of heart rate change depends on the baseline heart rate before stimulation.
Anaesthetic Relevance
- Explains tachycardia with rapid IV fluid administration
- Relevant during procedures with large fluid shifts
- Operates in opposition to the baroreceptor reflex (one tends to slow heart, the other to speed it)
- The interplay between Bainbridge and baroreceptor reflexes determines the net heart rate response during fluid loading
4. BEZOLD-JARISCH REFLEX
Physiology
Receptors: Chemoreceptors and mechanoreceptors within the left ventricular wall (and coronary arteries)
Stimulus: Noxious ventricular stimuli - hypotension, empty ventricle, ischaemia, serotonin, veratridine, capsaicin, certain drugs
Afferent Pathway: Unmyelinated vagal afferent type C fibres → reflexively increase parasympathetic tone
Classic Triad of Response:
- Hypotension
- Bradycardia
- Coronary artery dilatation
Modulation:
- ANP and BNP receptors may modulate the reflex; therefore it may be less pronounced in patients with cardiac hypertrophy or atrial fibrillation
- Serotonin (5-HT3) can trigger the reflex (hence interest in ondansetron as a modulator)
Physiologic role: Considered a cardioprotective reflex - thought to reduce myocardial work in ischaemia/infarction
Clinical Anaesthetic Relevance - HIGH YIELD
-
Spinal anaesthesia-induced cardiac arrest - particularly in young, healthy, conscious patients. Mechanism: hypovolemia + extensive spinal block → small end-systolic LV volume → mechanoreceptor-mediated bradycardia via Bezold-Jarisch reflex
-
Neuraxial anaesthesia (subarachnoid block):
- Cardiac accelerator fibers (T1-T4) blocked → vagal predominance → bradycardia
- Decrease in cardiac filling pressures → further stimulation via Bezold-Jarisch reflex
- Cardiac arrest has been reported; early use of epinephrine is critical in resuscitation
-
Shoulder surgery (beach chair/sitting position):
- Ventricular underfilling → Bezold-Jarisch reflex → sudden bradycardia and hypotension
- Intraoperative use of epinephrine, fentanyl, hydralazine, propofol implicated
-
Serotonin modulation: Ondansetron (5-HT3 antagonist) has been studied to blunt spinal anaesthesia-induced hypotension via modulation of this reflex
-
Myocardial ischaemia/infarction, thrombolysis, reperfusion: Reflex activation causes vagal bradycardia post-MI
5. OCULOCARDIAC REFLEX (OCR) - HIGH YIELD
Definition
A trigeminovagal reflex first described by Aschner and Dagnini in 1908.
Physiology
Stimulus: Pressure on the globe, traction on extraocular muscles (especially medial rectus), stimulation of orbital contents/periosteum, orbital injection, retrobulbar block, ocular trauma, pressure on orbital apex tissue after enucleation
Afferent Limb (Trigeminal):
Pain/pressure/traction impulses → Short and long ciliary nerves → Ciliary ganglion → Ophthalmic division of trigeminal nerve (CN V1) → Gasserian (trigeminal) ganglion → Sensory nucleus of trigeminal nerve → Motor nucleus of vagus
Efferent Limb (Vagal):
Motor nucleus of vagus → Vagus nerve → Heart (↓ HR, ↓ contractility)
Cardiac Manifestations (spectrum):
- Sinus bradycardia (most common)
- Junctional rhythm
- Ectopic atrial rhythm
- Atrioventricular block
- Ventricular bigeminy / multifocal PVCs
- Wandering pacemaker
- Idioventricular rhythm
- Ventricular tachycardia
- Asystole
Incidence: 30-90% during ophthalmic surgery; higher in children (16-82% variability in literature); children have higher vagal tone
Tachyphylaxis: The reflex is attenuated with repeated stimulation (fatigue at cardioinhibitory centre level); heart rate returns to baseline within ~20 seconds of stopping stimulation
Factors that Exacerbate OCR
- Hypoxaemia
- Hypercapnia
- Inadequate depth of anaesthesia
- Young age
- Use of opioids (fentanyl, alfentanil, remifentanil)
- Regional eye block (paradoxically can also elicit it)
Management
Prophylaxis:
- IV atropine (20 mcg/kg) within 30 minutes of surgery - reduces incidence
- IV glycopyrrolate (0.01 mg/kg) - less tachycardia than atropine; useful alternative
- IM anticholinergics in premedication are ineffective for prophylaxis
- Note: prophylactic atropine in adults is generally NOT recommended routinely due to its own dysrhythmogenic potential (VF, VT, LBBB reported)
- Ketamine induction (vs. propofol) associated with lower OCR incidence in children (Choi et al.)
- Retrobulbar block: not uniformly effective; can itself trigger OCR
Treatment of established OCR:
- Ask surgeon to immediately stop surgical stimulation
- Assess depth of anaesthesia
- Check and correct ventilation status (oxygenation and CO2)
- If arrhythmia persists after above:
- IV Glycopyrrolate 0.1-0.2 mg (paediatric: 10 mcg/kg)
- IV Atropine 10-20 mcg/kg
- If severe bradycardia or asystole: IV Epinephrine
6. VALSALVA MANEUVER
A useful test of baroreceptor and autonomic function.
Phases
| Phase | Event | Cardiovascular Response |
|---|---|---|
| I (strain onset) | ↑ intrathoracic pressure | Transient ↑ BP (chest compression) |
| II (sustained strain) | ↓ venous return | ↓ CO, ↓ BP → baroreceptor reflex → ↑ HR, vasoconstriction |
| III (strain release) | ↓ intrathoracic pressure | Brief further ↓ BP |
| IV (after release) | ↑ venous return → vigorous contraction | ↑ BP → baroreceptor reflex → ↓ HR (reflex bradycardia) |
Key points:
- Phase IV overshoot + reflex bradycardia confirms intact baroreceptor reflex
- Absent phase IV response indicates autonomic dysfunction (e.g., diabetic neuropathy, spinal cord injury)
- Valsalva terminates paroxysmal supraventricular tachycardia via vagal stimulation
7. CUSHING REFLEX (Vasopressor Response)
Physiology
Trigger: Cerebral ischaemia due to raised intracranial pressure (ICP)
Mechanism:
- Raised ICP → cerebral ischaemia at medullary vasomotor center
- Initial activation of sympathetic nervous system → ↑ HR, ↑ BP, ↑ myocardial contractility (to improve cerebral perfusion)
- High vascular tone → detected by baroreceptors → reflex bradycardia via parasympathetic activation
Classic Cushing Triad:
- Hypertension (widened pulse pressure)
- Bradycardia
- Irregular respirations
Anaesthetic Relevance
- Sign of severely raised ICP and impending brainstem herniation
- Do not treat the hypertension in isolation - treat the underlying ICP
- Seen in neurosurgical emergencies and head injuries
SUMMARY TABLE
| Reflex | Receptor Location | Afferent | Efferent | Key Response | Anaesthetic Importance |
|---|---|---|---|---|---|
| Baroreceptor | Carotid sinus, Aortic arch | CN IX, X → NTS | Sympathetic + Parasympathetic | BP homeostasis | Blunted by volatiles; spinal anaesthesia |
| Chemoreceptor | Carotid/aortic bodies | CN IX, X | Parasympathetic (then sympathetic) | ↑ Ventilation; ↓ HR initially | Hypoxia-induced bradycardia |
| Bainbridge | RA wall, cavoatrial junction | Vagal afferents | Parasympathetic inhibition | ↑ HR with ↑ venous return | Fluid loading tachycardia |
| Bezold-Jarisch | LV wall (C-fibres) | Vagal C-fibres | Parasympathetic | Hypotension + Bradycardia + Coronary dilation | Spinal anaesthesia cardiac arrest; sitting position surgery |
| Oculocardiac | Extraocular muscles/globe | CN V1 (trigeminal) | CN X (vagus) | Bradycardia to asystole | Ophthalmic surgery; treat: stop stimulation, atropine/glycopyrrolate |
| Valsalva | Baroreceptors | CN IX, X | Sympathetic/Parasympathetic | Phase IV bradycardia | Tests autonomic integrity; treats SVT |
| Cushing | Medullary vasomotor centre | Direct ischaemia | Sympathetic then baroreceptor | Hypertension + Bradycardia | Raised ICP emergency; do not treat BP alone |
KEY EXAM POINTS
- OCR afferent = CN V (trigeminal); efferent = CN X (vagus) - the most commonly asked fact
- OCR is more common in children (higher vagal tone); tachyphylaxis occurs with repeated stimulation
- First step in OCR management = ask surgeon to stop stimulation (not atropine)
- Bezold-Jarisch reflex triad = hypotension + bradycardia + coronary dilatation; most relevant in spinal anaesthesia, beach chair position
- Bainbridge reflex explains tachycardia with rapid IV fluid administration
- Baroreceptor reflex set point is reset upward in chronic hypertension
- Baroreceptor reflex loses function when BP < 50 mmHg
- Cushing reflex = raised ICP triad: hypertension + bradycardia + irregular respirations
- Ondansetron may mitigate spinal anaesthesia hypotension by blocking 5-HT3-mediated Bezold-Jarisch activation
- Volatile agents blunt the baroreceptor reflex in a dose-dependent manner
Sources: Miller's Anesthesia 10e (Chapter 13, 16, 26) | Barash's Clinical Anesthesia 9e (Chapters 17, 35) | Costanzo Physiology 7e (Chapter 4) | Guyton & Hall Textbook of Medical Physiology
Also add one more reflex of related with anal surgery in it
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
ano-cardiac reflex anal surgery bradycardia anaesthesia mechanism vasovagal
Reading Web Page
ano-cardiac reflex anal surgery bradycardia mechanism treatment
Finding Sources
I now have all the information needed. The reflex specifically associated with anal surgery is the Ano-cardiac reflex (also referred to as the recto-vagal reflex or perineo-cardiac reflex) - it is a well-known vasovagal phenomenon in anaesthetic practice during anal/perianal procedures. Here is the complete addition to your notes:
8. ANO-CARDIAC REFLEX (Recto-Vagal / Perineo-Cardiac Reflex)
Definition
The ano-cardiac reflex is a vasovagal reflex triggered by stimulation of the highly innervated anal canal, perianal region, or rectum during surgical procedures - most commonly hemorrhoidectomy, anal fissure surgery, anal dilatation, perianal abscess drainage, proctoscopy, and rubber band ligation of hemorrhoids.
Anatomy and Innervation of the Anal Canal
The anal canal has a rich innervation that makes it one of the most sensitive areas to vasovagal trigger:
- Above dentate line: Autonomic innervation - sympathetic (L1-L2) and parasympathetic (S2-S4 via pelvic splanchnic nerves)
- Below dentate line: Somatic innervation via the inferior rectal branch of the pudendal nerve (S2-S4) - carries pain, pressure, and stretch sensations
- The perianal skin and lower anal canal have dense sensory nerve endings that are exquisitely sensitive to stretch, traction, and pressure
Pathway
Afferent limb:
Stretch/pain/traction in anal canal or perianal region → Inferior rectal nerves (branch of pudendal nerve, S2-S4) → Pelvic splanchnic nerves → Sacral spinal cord → Ascending pathways → Medullary cardiovascular centre (nucleus tractus solitarius / dorsal motor nucleus of vagus)
Efferent limb:
Dorsal motor nucleus of vagus → Vagus nerve (CN X) → SA node → ↓ HR, ↓ BP
Response
The classic vasovagal triad:
- Bradycardia (sinus bradycardia, sometimes severe; junctional rhythm; asystole in extreme cases)
- Hypotension (due to vasodilation + reduced cardiac output)
- Pallor, sweating, nausea (in awake/sedated patients)
The response is essentially identical to the Bezold-Jarisch/vagal reflex pattern but triggered from the perineal/anorectal region rather than cardiac receptors.
Clinical Settings - HIGH YIELD
| Procedure | Mechanism |
|---|---|
| Hemorrhoidectomy | Traction on hemorrhoidal pedicles; injection of sclerosant |
| Rubber band ligation | Stretch of anal canal/submucosal tissue |
| Anal dilatation (Lord's procedure) | Forceful dilatation of internal sphincter |
| Anal fissure surgery / sphincterotomy | Traction and cutting of sphincter muscle |
| Perianal abscess incision & drainage | Pressure and pain in the anal region |
| Proctoscopy / rigid sigmoidoscopy | Rectal distension |
| Injection sclerotherapy | Chemical irritation of submucosal plexus |
| Transrectal ultrasound-guided biopsy | Probe insertion and manipulation in anal canal |
Predisposing Factors (Same as General Vasovagal)
- High vagal tone (young, athletic patients)
- Anxiety or pain prior to/during procedure
- Inadequate depth of anaesthesia or inadequate regional block
- Hypovolemia / inadequate preload
- Use of propofol or opioids (fentanyl, remifentanil) - enhance vagal tone
- Performing under sedation/local anaesthesia (greater sensory awareness)
- Hypoxia and hypercapnia (exacerbate vagal response)
Interaction with Neuraxial Anaesthesia
Anal surgery is commonly performed under spinal anaesthesia (saddle block/low spinal) or caudal anaesthesia. In this setting, the reflex risk is compounded:
- Sympathectomy from the spinal block reduces compensatory vasoconstriction
- Bezold-Jarisch reflex may be co-triggered by reduced venous return
- Cardiac arrest under spinal anaesthesia for perianal surgery has been reported in the literature (vasovagal + Bezold-Jarisch combination)
Prevention and Management
Preventive Measures:
- Adequate depth of anaesthesia or effective regional block - ensures the afferent limb is suppressed
- Saddle block (hypobaric or hyperbaric) - appropriate level for perineal surgery while limiting hemodynamic instability
- IV atropine (10-20 mcg/kg) or glycopyrrolate (0.01 mg/kg) - prophylactic anticholinergic, especially in high-risk patients
- Optimal preloading with IV fluids before neuraxial block
- Gentle surgical technique - avoid forceful traction, rapid distension
- Avoid unnecessary stretch of anal canal
- Patient positioning - avoid excessive lithotomy with legs elevated (reduces venous return further)
Treatment of Established Reflex:
- Ask surgeon to immediately stop surgical stimulation (first and most important step)
- Lay patient flat / Trendelenburg position (↑ venous return)
- Ensure adequate oxygenation (100% O2)
- Check depth of anaesthesia / block adequacy
- IV Atropine 0.6 mg (or glycopyrrolate 0.2 mg) - anticholinergic
- IV Ephedrine (mixed alpha + beta agonist) - if hypotension is significant
- If cardiac arrest: commence CPR + ALS algorithm; IV Epinephrine early
UPDATED SUMMARY TABLE (All 8 Reflexes)
| Reflex | Receptor Location | Afferent | Efferent | Key Response | Anaesthetic Importance |
|---|---|---|---|---|---|
| Baroreceptor | Carotid sinus, Aortic arch | CN IX, X → NTS | Sympathetic + Parasympathetic | BP homeostasis | Blunted by volatile agents; spinal block |
| Chemoreceptor | Carotid/aortic bodies | CN IX, X | Parasympathetic then Sympathetic | ↑ Ventilation; ↓ HR initially | Hypoxia-induced bradycardia |
| Bainbridge | RA wall, cavoatrial junction | Vagal afferents | Parasympathetic inhibition | ↑ HR with ↑ venous return | Fluid loading tachycardia |
| Bezold-Jarisch | LV wall (C-fibres) | Vagal C-fibres | Parasympathetic ↑ | Hypotension + Bradycardia + Coronary dilation | Spinal arrest; beach chair; hypovolemia |
| Oculocardiac | Extraocular muscles/globe | CN V1 → trigeminal nucleus | CN X (vagus) | Bradycardia to asystole | Ophthalmic surgery; stop stimulation first |
| Valsalva | Baroreceptors | CN IX, X | Sympathetic/Parasympathetic | Phase IV bradycardia | Autonomic testing; treats SVT |
| Cushing | Medullary vasomotor centre | Direct ischaemia | Sympathetic then baroreceptor | Hypertension + Bradycardia + Irregular respiration | Raised ICP emergency |
| Ano-cardiac | Anal canal, perianal skin, rectum | Pudendal nerve (S2-S4), pelvic splanchnics | CN X (vagus) | Vasovagal: Bradycardia + Hypotension | Hemorrhoidectomy, anal surgery; stop stimulation + atropine |
Key Exam Points for Ano-Cardiac Reflex
- Also known as the recto-vagal reflex or perineo-cardiac reflex - a form of vasovagal syncope specific to perianal surgery
- Afferent = pudendal nerve (S2-S4); efferent = vagus nerve (CN X)
- Most dangerous when anal surgery is performed under spinal anaesthesia - compound risk with Bezold-Jarisch reflex
- First step in management = stop surgical stimulation (identical to OCR management principle)
- Unlike OCR, tachyphylaxis does NOT reliably occur with this reflex
- Rubber band ligation of hemorrhoids can elicit this reflex even under local anaesthesia - monitor patients for at least 20-30 minutes post-procedure
Sources: Miller's Anesthesia 10e | Barash's Clinical Anesthesia 9e | Kinsella SM & Tuckey JP, Br J Anaesth 2001 (perioperative bradycardia and vasovagal reflex) | PMC10384961 (case report: syncope during spinal anaesthesia for perianal abscess)
This is a shared conversation. Sign in to Orris to start your own chat.