IBS D type
Reading File
Finding Sources
Searching PubMed
"irritable bowel syndrome" AND "diarrhea" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive IBS-D summary. Let me compile the full response:
IBS-D (Irritable Bowel Syndrome with Predominant Diarrhea)
Definition
IBS is characterized by chronic or recurrent abdominal pain associated with alterations in stool form and/or frequency. IBS-D is the subtype where loose/watery stools (Bristol types 6-7) predominate on days with abnormal stool consistency (>25% of such days), without the hard/lumpy stools that would define IBS-C.
Epidemiology
- Global prevalence: ~4.1% (Rome IV); higher with older criteria
- IBS-D and IBS-M (mixed) each account for 35-40% of all IBS patients
- Women affected more than men (5.2% vs 2.9%)
- Up to 50% of sufferers never seek care; still generates ~4.4 million annual physician visits
- Subtypes can transition over time in the same patient
Rome IV Diagnostic Criteria
Recurrent abdominal pain, at least 1 day/week on average in the last 3 months, associated with 2 or more of:
- Related to defecation
- Associated with a change in stool frequency
- Associated with a change in stool form (appearance)
Symptoms onset >6 months before diagnosis. For IBS-D specifically: >25% of bowel movements are loose/watery, and <25% are hard/lumpy.
Supporting symptoms (not required for diagnosis):
- Urgency
- Feeling of incomplete evacuation
- Passing mucus
- Bloating/abdominal distention
Alarm Features (Red Flags) - Rule Out Organic Disease
| Alarm Feature |
|---|
| New onset at age ≥50 years |
| Unintentional weight loss |
| Hematochezia or melena (not from hemorrhoids) |
| Nocturnal diarrhea |
| Anemia |
| Palpable abdominal mass or lymphadenopathy |
| Family history of colorectal cancer, IBD, or celiac disease |
Diagnostic Algorithm
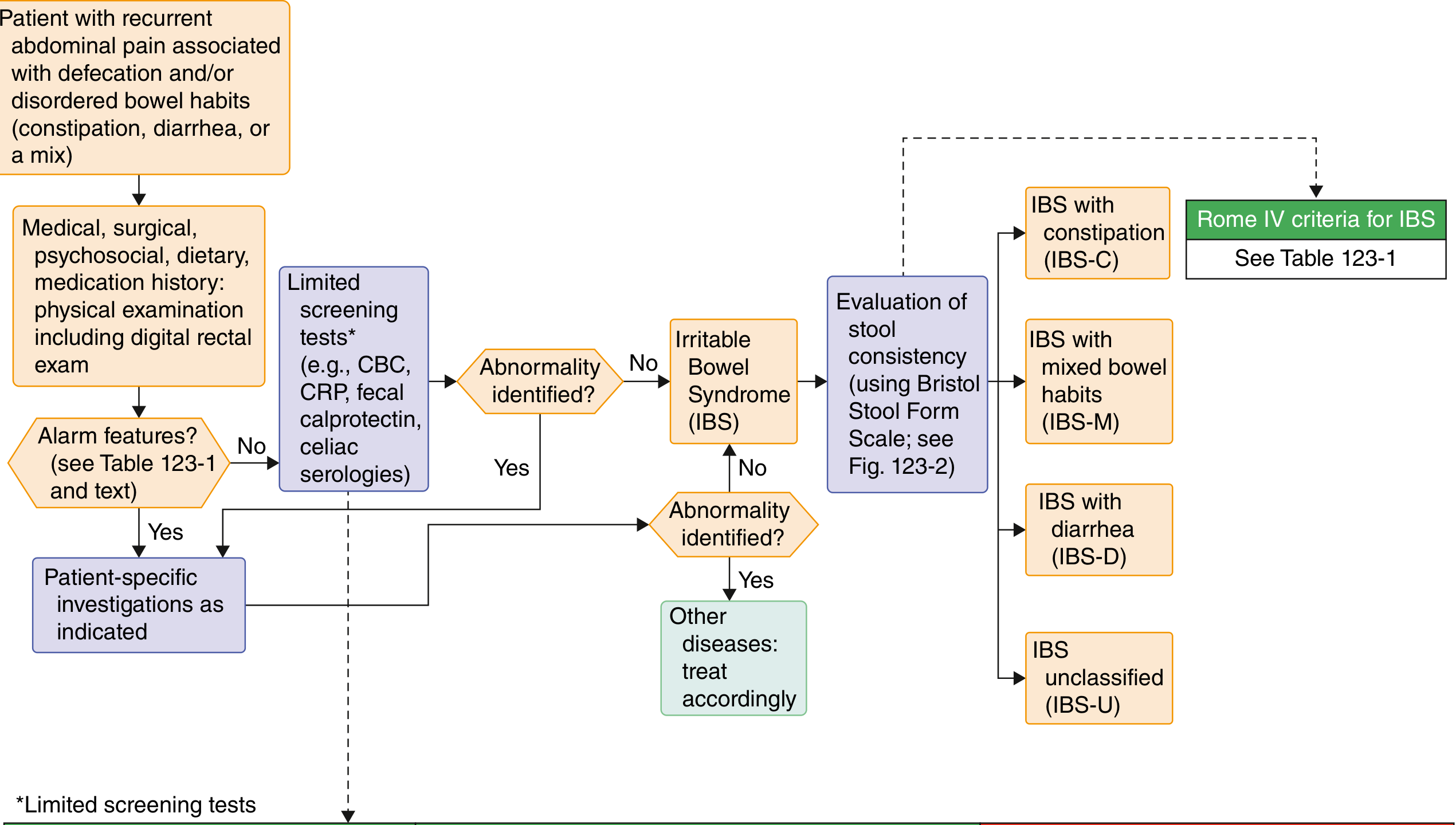
Recommended Investigations in IBS-D
| Test | Rationale |
|---|---|
| Celiac serologies | Celiac disease commonly mimics IBS-D |
| Fecal calprotectin / lactoferrin | Exclude IBD (elevated in inflammation) |
| C-reactive protein | Elevated in IBD, not IBS |
| Bile acid diarrhea testing | If bile acid malabsorption is suspected |
| Giardia stool antigen | If giardia is endemic |
Not routinely recommended: colonoscopy <45 yrs (unless alarm features), food allergy testing, lactulose/glucose hydrogen breath testing
Pathobiology (Multifactorial)
IBS-D results from dysregulation of gut-brain interactions, affecting:
| Mechanism | Detail |
|---|---|
| Visceral hypersensitivity | Lowered pain threshold to gut distension; key driver of abdominal pain |
| Altered motility | Accelerated colonic transit in IBS-D; exaggerated postprandial responses |
| Gut microbiota dysbiosis | Altered composition; post-infectious IBS (PI-IBS) is a well-defined trigger |
| Mucosal immune activation | Low-grade inflammation; increased mast cells and cytokines |
| Serotonin (5-HT) dysregulation | >95% of body 5-HT is in gut enterochromaffin cells; 5-HT3 and 5-HT4 receptors modulate motility and pain |
| Bile acid malabsorption | Excess bile acids in colon accelerate transit; accounts for a subset of IBS-D |
| CNS modulation | Abnormal descending pain inhibition; stress axis (HPA) dysregulation |
| Genetic factors | IBS clusters in families; several gene variants implicated |
| Post-infectious trigger | ~10% of IBS cases follow acute gastroenteritis (PI-IBS) |
Differential Diagnosis of IBS-D
- Celiac disease
- IBD (Crohn's disease, ulcerative colitis)
- Microscopic colitis
- Bile acid malabsorption
- Lactose/fructose intolerance
- Small intestinal bacterial overgrowth (SIBO)
- Thyroid dysfunction (hyperthyroidism)
- Giardiasis
- Functional diarrhea (no abdominal pain component)
Treatment
Treatment is stepwise, targeting the dominant symptom (diarrhea, pain, bloating).
1. Lifestyle & Dietary Measures (First-line)
- Low FODMAP diet: most evidence-based dietary intervention; reduces fermentable carbohydrates
- Avoid food triggers (dairy, caffeine, high-fat meals, alcohol)
- Regular meals, adequate hydration
- Exercise
2. Pharmacological Treatment for IBS-D
| Drug | Dose | Mechanism/Notes |
|---|---|---|
| Loperamide | 2-4 mg up to 4x/day | Opioid µ-receptor agonist; reduces stool frequency and urgency; does NOT relieve pain |
| Eluxadoline (Viberzi) | 75-100 mg twice daily | Mixed µ-opioid agonist / δ-antagonist; reduces diarrhea AND abdominal pain; avoid if no gallbladder |
| Alosetron (Lotronex) | 0.5-1 mg twice daily | 5-HT3 antagonist; reduces urgency, pain, stool frequency; restricted use - risk of ischemic colitis; women with severe IBS-D only |
| Rifaximin (Xifaxan) | 550 mg three times daily x 14 days | Non-absorbed antibiotic; modulates gut microbiota; repeat courses allowed |
| Bile acid sequestrants (cholestyramine, colesevelam) | Variable | For suspected bile acid malabsorption subtype |
3. Antispasmodics (for Pain/Spasm)
| Drug | Dose |
|---|---|
| Peppermint oil | 1-2 capsules three times daily |
| Hyoscyamine | 0.125 mg three to four times daily or as needed |
| Dicyclomine | 10 mg three to four times daily |
4. Central Neuromodulators (Brain-Gut)
Used to treat IBS symptoms (not purely for psychiatric comorbidity):
- TCAs (amitriptyline, desipramine, nortriptyline): 10-25 mg at bedtime; slow GI transit - preferred in IBS-D; also treat pain; titrate up to 100 mg
- SSRIs (fluoxetine, paroxetine, sertraline, citalopram): may accelerate transit - better for IBS-C; can help with global well-being and comorbid anxiety/depression
- SNRIs (duloxetine): can address both pain and bowel function
5. Psychological Therapies
Strong evidence for:
- Cognitive behavioral therapy (CBT)
- Gut-directed hypnotherapy
- Mindfulness-based stress reduction
IBS-D Treatment Algorithm Summary
IBS-D Diagnosis Confirmed
↓
Diet (Low FODMAP) + Lifestyle
↓
Loperamide (diarrhea/urgency) + Antispasmodics (pain)
↓
Rifaximin (14-day course, repeatable)
↓
Eluxadoline (pain + diarrhea) OR Alosetron (severe, women only)
↓
TCAs (amitriptyline/desipramine) + Psychological therapy
Prognosis
- Symptoms fluctuate; exacerbations triggered by stress, dietary indiscretion, infections
- Natural history shows subtype can shift (IBS-D ↔ IBS-M ↔ IBS-C) over time
- Mortality not increased, but significant quality-of-life impairment and healthcare burden
Sources: Goldman-Cecil Medicine (27e), Chapter 123 | Sleisenger & Fordtran's GI and Liver Disease
Recent evidence note: A 2026 meta-analysis on IBS pharmacotherapy safety (PMID: 40471839) is available and may refine the safety profiles of agents like alosetron and eluxadoline - worth reviewing for the most current data.
IBS AND IBD difference
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative data for a complete IBS vs IBD comparison. Here is the full response:
IBS vs IBD - Key Differences
These two conditions are commonly confused because they share overlapping symptoms (abdominal pain, altered bowel habits), but they are fundamentally different in nature, pathology, investigation, and management.
Core Concept
| Feature | IBS | IBD |
|---|---|---|
| Nature | Functional disorder (gut-brain dysregulation) | Organic/structural inflammatory disease |
| Inflammation | No true mucosal inflammation | Yes - actual intestinal inflammation/tissue damage |
| Structural damage | None | Mucosal ulceration, fibrosis, strictures, fistulas |
| Subtypes | IBS-C, IBS-D, IBS-M, IBS-U | Crohn's disease (CD), Ulcerative colitis (UC) |
| Malignancy risk | Not increased | Significantly increased (colorectal cancer) |
| Reversibility | Symptoms fluctuate; no structural damage | Can cause permanent bowel damage, may require surgery |
Epidemiology
| Feature | IBS | IBD |
|---|---|---|
| Global prevalence | ~4.1% (Rome IV) | ~0.3% (UC) / ~0.3% (CD) |
| Sex | Women > Men (5.2% vs 2.9%) | CD: F slightly > M; UC: Equal |
| Peak age of onset | Any age; most common 18-45 yrs | CD: 15-30 (+ 2nd peak 7th decade); UC: 20-40 |
Pathophysiology
IBS
- Gut-brain axis dysregulation - no structural damage
- Visceral hypersensitivity (lowered pain threshold)
- Altered colonic motility (faster in IBS-D, slower in IBS-C)
- Gut microbiota dysbiosis
- Low-grade mucosal immune activation (not destructive)
- Serotonin pathway abnormalities (5-HT3/5-HT4)
- Triggered by stress, diet, prior infections (PI-IBS)
IBD
- True autoimmune/dysregulated mucosal immunity
- Inappropriate activation of T-cells against gut flora
- Transmural inflammation (in Crohn's) or mucosal/submucosal (in UC)
- Cytokine-driven tissue destruction (TNF-α, IL-6, IL-12/23)
- Genetic factors: NOD2 gene mutations in Crohn's
- Environmental triggers: smoking (protective in UC, harmful in CD), appendectomy, diet
Crohn's vs Ulcerative Colitis (Within IBD)
| Characteristic | Crohn's Disease | Ulcerative Colitis |
|---|---|---|
| GI tract involvement | Esophagus to anus ("mouth to anus") | Colon only |
| Pattern | Skip lesions (patchy) | Continuous from rectum proximally |
| Inflammation depth | Transmural (full thickness) | Mucosal/submucosal only |
| Ulcer type | Usually discrete | Continuous |
| Fistula | Yes (common) | No |
| Stricture | Yes | No |
| Perianal disease | Yes | No |
| Peak age | 15-30 yrs (+ 2nd peak 7th decade) | 20-40 yrs |
| Sex ratio (F:M) | 1.2:1 | 1:1 |
Clinical Features Compared
| Symptom/Sign | IBS | IBD |
|---|---|---|
| Abdominal pain | Yes - relieved by defecation | Yes - may NOT be relieved by defecation |
| Diarrhea | Yes (IBS-D/IBS-M) | Yes - often bloody in UC |
| Rectal bleeding | No | Yes (especially UC) |
| Nocturnal symptoms | Rare / absent | Common (wakes patient from sleep) |
| Weight loss | Absent | Present (especially Crohn's) |
| Fever | Absent | Present with active disease |
| Mucus in stool | Sometimes | Often (with blood in UC) |
| Bloating/gas | Prominent | Less prominent |
| Extraintestinal manifestations | None | Yes (see below) |
| Perianal disease | Absent | Crohn's: fissures, fistulas, skin tags |
IBD Extraintestinal Manifestations (NOT seen in IBS)
| System | Manifestation |
|---|---|
| Joint | Arthropathy, ankylosing spondylitis, sacroiliitis (10-20%) |
| Skin | Erythema nodosum (10-15%), pyoderma gangrenosum (1-2%) |
| Eye | Uveitis, episcleritis (5-15%) |
| Liver | Primary sclerosing cholangitis (2-7.5%; strongly linked to UC) |
| Bone | Osteoporosis, osteomalacia |
| Renal | Nephrolithiasis (calcium oxalate; uric acid) |
| Blood | Thromboembolic disease, B12 deficiency (Crohn's) |
Investigations
| Test | IBS | IBD |
|---|---|---|
| Fecal calprotectin | Normal (<60 µg/g) | Elevated (>150 µg/g) |
| CRP | Normal | Elevated in active disease |
| CBC | Normal | Anemia, leukocytosis, thrombocytosis |
| ESR | Normal | Elevated |
| Colonoscopy | Normal mucosa | Ulceration, erythema, friability, pseudopolyps |
| Histology | Normal or mild changes | Cryptitis, crypt abscesses (UC); granulomas (Crohn's) |
| Imaging (CT/MRI) | Normal | Bowel wall thickening, fistulas, strictures (Crohn's) |
| Stool cultures | Normal | Can co-exist with infection |
| Celiac serologies | Done to exclude celiac | Not typically primary test |
Fecal Calprotectin Algorithm (Key Differentiator)
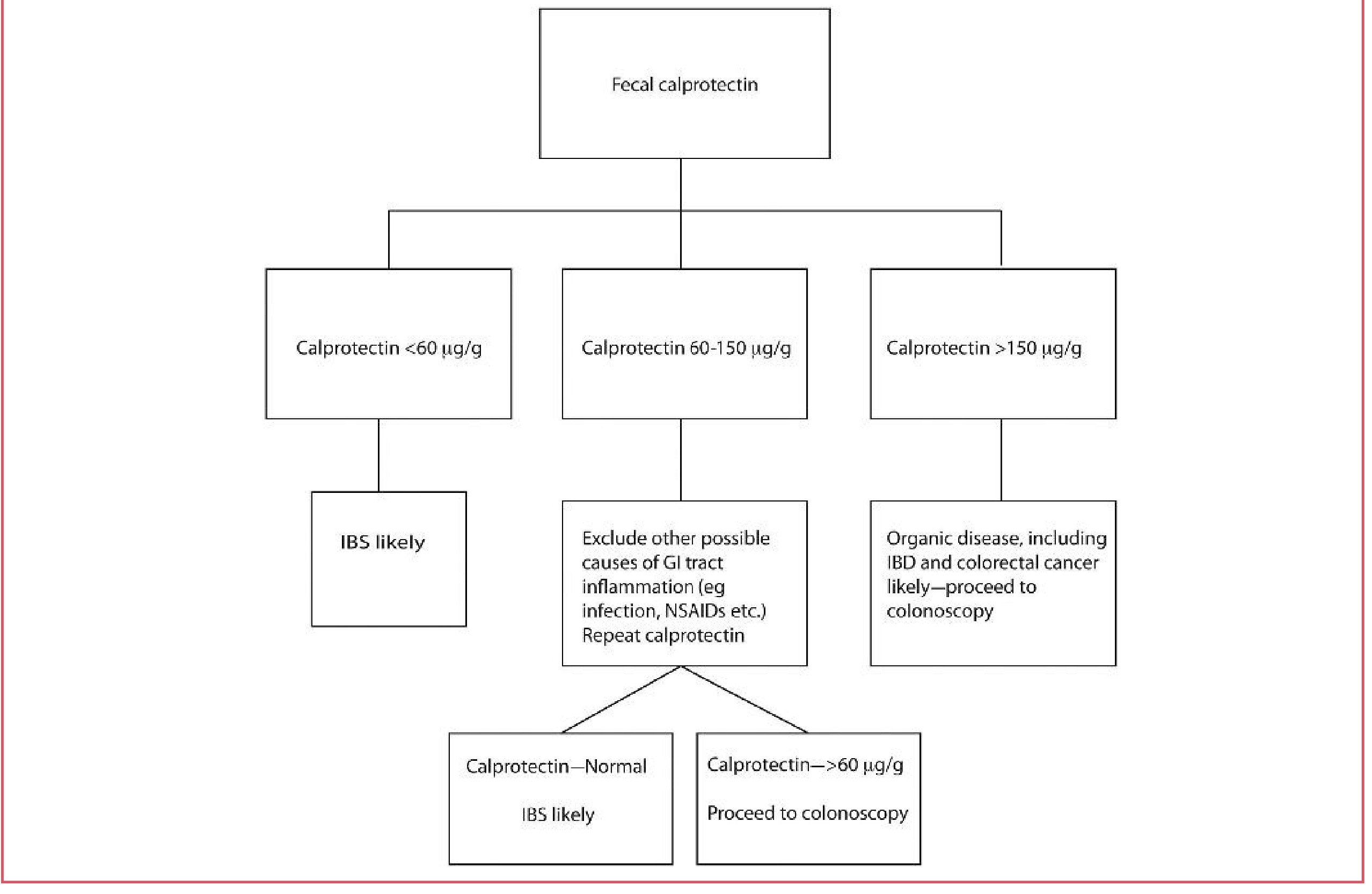
- <60 µg/g → IBS likely
- 60-150 µg/g → Exclude other GI inflammation (NSAIDs, infection); repeat test
- >150 µg/g → Organic disease (IBD, colorectal cancer) likely → proceed to colonoscopy
Diagnosis
| IBS | IBD | |
|---|---|---|
| Basis | Clinical (Rome IV criteria) - diagnosis of exclusion | Endoscopic + histological confirmation required |
| Key criteria | Recurrent abdominal pain ≥1 day/week, associated with defecation or stool change; onset >6 months | Colonoscopy showing mucosal changes + biopsy |
Red flags that suggest IBD over IBS:
- Rectal bleeding
- Nocturnal diarrhea
- Unintentional weight loss
- Fever
- Age >50 at new onset
- Elevated inflammatory markers (CRP, calprotectin, ESR)
- Anemia
Treatment
IBS Treatment (Functional - no inflammation to treat)
- Dietary modification (low-FODMAP diet)
- Antispasmodics (peppermint oil, hyoscyamine)
- Loperamide (for IBS-D)
- Rifaximin, eluxadoline, alosetron (for IBS-D)
- TCAs / SSRIs (brain-gut neuromodulators)
- Psychological therapy (CBT, gut-directed hypnotherapy)
IBD Treatment (Anti-inflammatory / Immunosuppressive)
| Step | Drugs |
|---|---|
| Mild-moderate | Aminosalicylates (mesalazine/5-ASA) - especially UC |
| Moderate-severe | Corticosteroids (prednisone, budesonide) for induction |
| Maintenance | Thiopurines (azathioprine, 6-mercaptopurine), methotrexate |
| Biologics | Anti-TNF (infliximab, adalimumab), anti-integrin (vedolizumab), anti-IL12/23 (ustekinumab) |
| Small molecules | JAK inhibitors (tofacitinib, upadacitinib) for UC |
| Surgery | Colectomy (UC can be curative); bowel resection in Crohn's complications |
Cancer Risk
| IBS | IBD | |
|---|---|---|
| Colorectal cancer risk | Not increased | Significantly increased |
| UC risk | - | Begins after 7-10 years; ~15-18% at 30 years |
| Crohn's risk | - | 4-20x increased in ileocolitis |
| Surveillance colonoscopy | Not routinely required | Required (every 1-2 years after 8-10 years of disease) |
Summary Table
| Feature | IBS | IBD |
|---|---|---|
| Inflammation | None | Yes |
| Bleeding | No | Yes (especially UC) |
| Weight loss | No | Yes |
| Fever | No | Yes |
| Nocturnal symptoms | No | Yes |
| Biomarkers (CRP/calprotectin) | Normal | Elevated |
| Colonoscopy | Normal | Abnormal |
| Extra-intestinal manifestations | None | Yes (joints, skin, eyes, liver) |
| Cancer risk | None | Increased |
| Treatment | Symptomatic/functional | Anti-inflammatory/immunosuppressive |
| Curative surgery | Not applicable | Available for UC (colectomy) |
Sources: Goldman-Cecil Medicine (27e), Chapters 123 & 127 | Sleisenger & Fordtran's GI and Liver Disease | Tietz Textbook of Laboratory Medicine (7e)
This is a shared conversation. Sign in to Orris to start your own chat.