Whipple sx
Reading File
Finding Sources
Finding Sources
Searching PubMed
pancreaticoduodenectomy Whipple procedure outcomes
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer.
Whipple Procedure (Pancreaticoduodenectomy)
Overview
Pancreaticoduodenectomy (PD) is the most common operation for tumors of the periampullary region. It involves removal of the pancreatic head, duodenum, gallbladder, and distal bile duct, with or without removal of the gastric antrum (pylorus-preserving vs. standard Whipple). - Current Surgical Therapy 14e
Indications
- Pancreatic head adenocarcinoma (most common)
- Periampullary malignancies: ampullary carcinoma, distal cholangiocarcinoma, duodenal adenocarcinoma
- Cystic neoplasms of the pancreatic head (IPMN with high-risk features)
- Chronic pancreatitis with inflammatory mass in the head (selected cases)
- Pancreas divisum with failed minor duct sphincteroplasty and chronic pancreatitis changes in the head
Preoperative Workup
- Pancreatic-protocol CT scan within 1 month of planned surgery - cornerstone of staging
- Assess tumor relationship to SMA, SMV-PV, celiac axis, and hepatic artery
- Look for aberrant arterial anatomy (replaced right/left hepatic artery)
- Note IMV insertion and first jejunal branch (anterior vs. posterior to SMA)
- Diagnostic laparoscopy before laparotomy - ~10% of patients have small-volume metastases missed on imaging
The Six Steps of Resection
Step 1 - Define the infrapancreatic SMV
The greater omentum is elevated, hepatic flexure mobilized, and the lesser sac entered. The visceral peritoneum along the inferior pancreatic border is incised to expose the SMV and the middle colic vein junction. A "tunnel" is established anterior to the portal-SMV confluence to assess vascular involvement before committing to resection.
Step 2 - Kocher maneuver
The duodenum and pancreatic head are mobilized medially to the level of the left renal vein. The peritoneum posterior to the mesenteric vessels is divided, exposing the aorta and facilitating SMA dissection.
Step 3 - Portal dissection
The common hepatic artery is identified and the hepatic artery lymph node is removed. A top-down cholecystectomy is performed to identify the junction of the cystic duct and common bile duct. The GDA is ligated and divided (after test clamping to confirm adequate hepatic inflow).
Step 4 - Gastric/duodenal transection
- Pylorus-preserving: Duodenum divided ~2 cm distal to the pylorus - preferred for small periampullary tumors
- Standard (classic): Antrectomy performed at the level of the 3rd/4th transverse lesser curvature vein - used for bulky pancreatic head tumors or duodenal tumors involving the 1st/2nd portion; also recommended if preoperative radiation given
Step 5 - Jejunal transection
The ligament of Treitz is taken down (preserving the inferior mesenteric vein). Jejunum is divided ~10 cm distal to the ligament of Treitz and the devascularized duodenum-jejunum segment is reflected under the mesenteric vessels to the right abdomen.
Step 6 - Pancreatic neck transection and SMA dissection
The pancreatic neck is transected at the level of the PV with electrocautery. Vessel loops are passed around the SMV, PV, and splenic vein. The SMA is directly exposed posteriorly, and the inferior pancreaticoduodenal arteries are individually ligated. The head of the pancreas is then separated from the SMV-PV by careful ligation of venous tributaries.
Reconstruction
The reconstruction involves three anastomoses performed in sequence on a single Roux limb of jejunum:
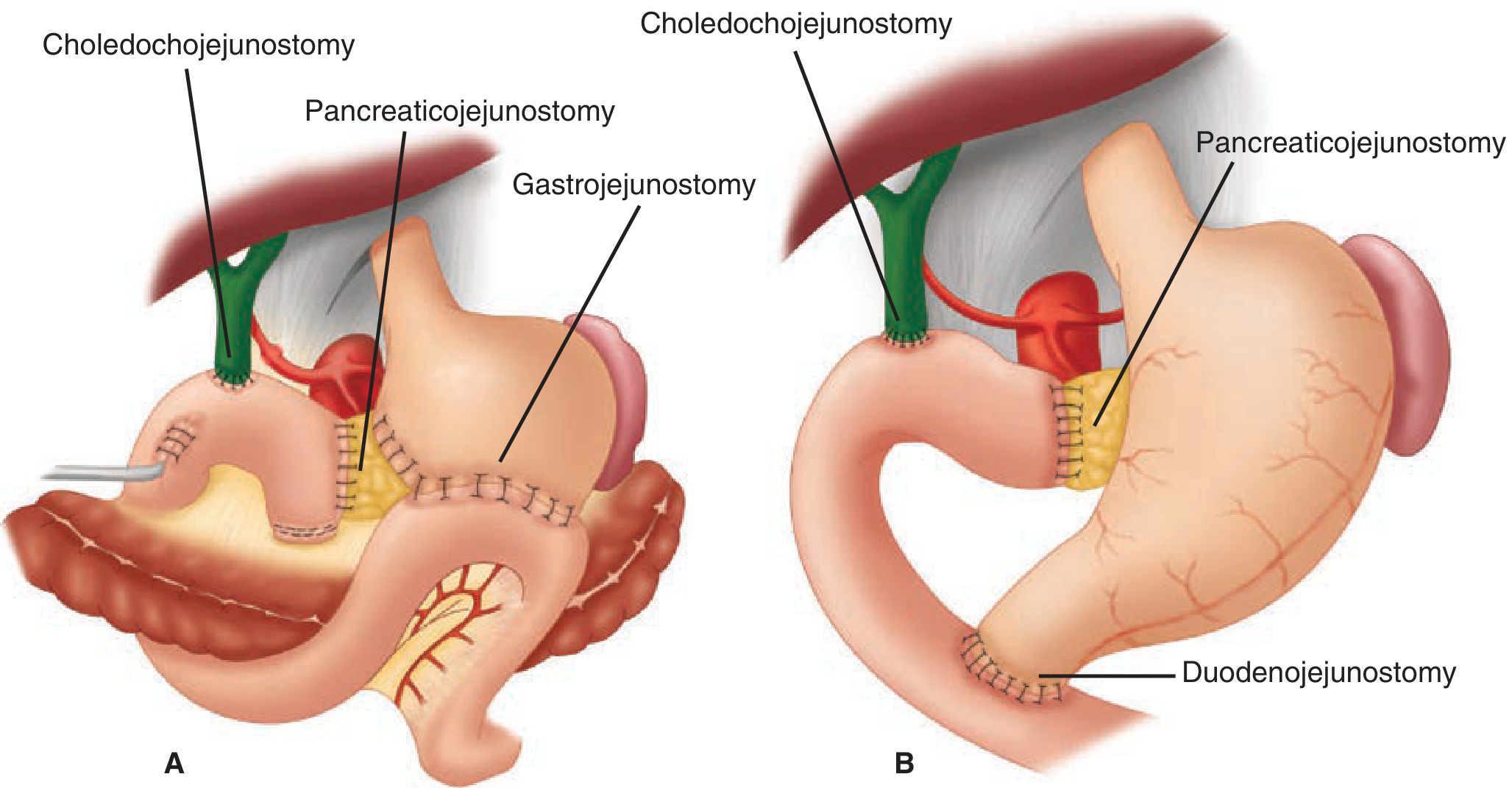
Standard Whipple (A) with gastrojejunostomy vs. pylorus-preserving (B) with duodenojejunostomy. Both share pancreaticojejunostomy and choledochojejunostomy. - Schwartz's Principles of Surgery, 11e
- Pancreaticojejunostomy (PJ) - most proximal; most technically demanding; either end-to-side duct-to-mucosa or invagination technique
- Hepaticojejunostomy (HJ) / Choledochojejunostomy - bile duct to jejunum, ~10-15 cm downstream
- Gastrojejunostomy or Duodenojejunostomy - most distal; antecolic placement preferred over retrocolic (lower delayed gastric emptying rates)
Major Complications
Complication rates overall: ~40-41% in large series; operative mortality at experienced centers: <2-3%. - Maingot's Abdominal Operations; Schwartz's 11e
| Complication | Incidence | Key Management |
|---|---|---|
| Postoperative Pancreatic Fistula (POPF) | 10-30% | Drainage (surgical/IR); octreotide may reduce rate; NPO + nutrition support |
| Delayed Gastric Emptying (DGE) | 10-19% | NG decompression, prokinetics (erythromycin, metoclopramide); antecolic GJ reduces risk; usually self-limiting |
| Postpancreatectomy Hemorrhage (PPH) | ~5% | Highest mortality (10-16%); early = technical failure → reoperation; late (day 7-14) = pseudoaneurysm (often GDA) or marginal ulcer → IR embolization/stenting |
| Biliary leak | <5% | Wide drainage; PTBD for dilated ducts; avoid endoscopy in first 6 weeks |
| Wound infection | ~10% | Standard wound care |
DGE and POPF are most common; PPH is most feared. - Sabiston Textbook of Surgery; Current Surgical Therapy 14e
Risk factors for POPF: soft pancreatic texture, non-dilated pancreatic duct (<3 mm), normal preoperative serum amylase, small tumor size - these together constitute a "high-risk" anastomosis.
Pylorus-Preserving vs. Standard Whipple
- Pylorus-preserving PD (PPPD) - avoids antrectomy, theoretically better nutrition/dumping outcomes; rates of DGE are not significantly different from classic PD in RCTs
- Classic Whipple - includes antrectomy; preferred for bulky tumors, involved duodenum, or post-radiation cases
- Oncologic outcomes are equivalent between the two approaches
Minimally Invasive / Robotic Approaches
Robotic PD (RPD) and laparoscopic PD are increasingly performed at high-volume centers. A 2024 meta-analysis (PMID 39153714) comparing open vs. robotic PD found comparable long-term oncologic outcomes with potential benefits in perioperative recovery for the robotic approach.
Outcomes
- Pain relief in chronic pancreatitis: 71-89% at 4-6 years, but 25-48% develop new-onset diabetes postoperatively (Schwartz's 11e)
- 5-year survival for pancreatic ductal adenocarcinoma after R0 resection: 15-25% with adjuvant chemotherapy
- For periampullary cancers (ampullary, duodenal, distal CBD): significantly better - 5-year survival 40-60%
- High-volume centers (>20 PDs/year) have significantly lower mortality and morbidity
This is a shared conversation. Sign in to Orris to start your own chat.