Types pathogenesis features management of amenorrhea
Amenorrhea: Types, Pathogenesis, Features, and Management
Definition
- Primary amenorrhea: No menses by age 13 in the absence of secondary sexual characteristics, OR no menses by age 15 with normal secondary sexual characteristics.
- Secondary amenorrhea: Absence of menstruation for 3 months (or 6-9 months in women with oligomenorrhea) after previously established menses.
Normal Menstrual Physiology (Basis for Understanding Pathogenesis)
- Hypothalamus - pulsatile GnRH secretion
- Anterior pituitary - FSH and LH secretion in response to GnRH
- Ovaries - follicular development, ovulation, estrogen/progesterone production
- Uterus/Outflow tract - functioning endometrium and patent outflow
WHO Classification
| Group | Description | Hormonal Pattern |
|---|---|---|
| Group I | Hypogonadotropic hypogonadism | Low/normal FSH, low estrogen, normal PRL, no hypothalamic-pituitary lesion |
| Group II | Normogonadotropic anovulation (e.g., PCOS) | Normal FSH, evidence of estrogen production, normal PRL |
| Group III | Hypergonadotropic hypogonadism | Elevated FSH (gonadal insufficiency/failure) |
| Group IV (added later) | Hyperprolactinemic anovulation | Elevated prolactin causing anovulation |
Types and Pathogenesis
A. Outflow Tract / Uterine Causes (Anatomic)
| Condition | Mechanism |
|---|---|
| Imperforate hymen | Transverse blockage prevents blood from exiting; causes hematocolpos, cyclic pain |
| Transverse vaginal septum | Same as above |
| Cervical/vaginal agenesis | Obstructed outflow |
| MRKH Syndrome (Mayer-Rokitansky-Kuster-Hauser) | Mullerian agenesis; 46,XX karyotype; absent uterus/vagina; accounts for ~10-15% of primary amenorrhea |
| Asherman Syndrome | Intrauterine adhesions (synechiae) from D&C, postpartum curettage, or uterine infection/TB; endometrium destroyed - no response to hormones |
B. Ovarian (Gonadal) Causes
1. Hypergonadotropic Hypogonadism (High FSH)
- Accelerated follicular atresia in utero → streak ovaries by puberty
- No estrogen → absent secondary sexual characteristics
- Associated stigmata: short stature, webbed neck, shield chest, cubitus valgus, coarctation of aorta (30%), horseshoe kidney
- Gonadectomy if Y-cell line present (risk of gonadoblastoma)
- 46,XX gonadal dysgenesis, 46,XY (Swyer syndrome), mosaic karyotypes
- Partial deletions may allow some estrogen → secondary sexual characteristics then secondary amenorrhea
- Defined as FSH in menopausal range + amenorrhea ≥4 months in women <40 years
- Causes: autoimmune (20-40% of cases), chemotherapy, radiation, galactosemia, FMR1 premutation, idiopathic
- Mechanism: decreased follicular endowment, accelerated atresia, or follicle dysfunction
- 5-10% may still conceive spontaneously
2. Polycystic Ovary Syndrome (PCOS)
- Most common cause of secondary amenorrhea after pregnancy
- Pathophysiology: relatively low FSH with disproportionately high LH → multiple small follicles, androgen excess, chronic anovulation
- Insulin resistance plays a central role; high LH stimulates excess thecal androgen → peripheral aromatization to estrogen → chronic unopposed estrogen
- Rotterdam Criteria: 2 of 3 - hyperandrogenism, oligomenorrhea/amenorrhea, polycystic ovaries on US
- Clinical features: hirsutism (65%), infertility (50%), obesity (35%), amenorrhea (35%), oligomenorrhea (40%), acne (25%)
- Risk of endometrial hyperplasia/cancer from unopposed estrogen
C. Pituitary Causes
| Condition | Mechanism |
|---|---|
| Hyperprolactinemia (prolactinoma) | Elevated prolactin inhibits GnRH pulsatility → low FSH/LH → anovulation; dopamine normally suppresses PRL |
| Sheehan Syndrome | Postpartum pituitary necrosis from hemorrhage/hypotension; unable to lactate, lose pubic/axillary hair, no menses after delivery |
| Pituitary tumors (non-functioning) | Mass effect compresses normal pituitary; gonadotropin deficiency |
| Empty sella syndrome | Found in 4-16% of patients with amenorrhea + galactorrhea |
| Acromegaly / Cushing disease | Excess GH/ACTH inhibit GnRH pulse generator |
D. Hypothalamic Causes
| Trigger | Examples |
|---|---|
| Weight loss / malnutrition | Anorexia nervosa (↓↓ FSH, LH, estrogen), rapid weight loss, dieting |
| Exercise-induced | Athletes with negative energy balance ("female athlete triad") |
| Stress-induced | Psychological stress, chronic illness |
| Chronic disease | Diabetes, renal disease, liver disease, chronic infections |
| CNS lesions | Tumors, infiltrative disease (sarcoidosis, histiocytosis) |
- Deficiency of GnRH neurons (failed migration from olfactory placode)
- Characterized by: hypogonadotropic hypogonadism + anosmia
- Low FSH, LH, estrogen; lack of secondary sexual characteristics
E. Thyroid / Adrenal Causes
- Hypothyroidism: Elevated TRH stimulates prolactin → hyperprolactinemia → amenorrhea; treat hypothyroidism first
- Hyperthyroidism: Alters sex hormone binding globulin and estrogen metabolism
- Congenital adrenal hyperplasia (late-onset): Excess androgens suppress GnRH
- Cushing syndrome: Excess cortisol inhibits GnRH pulsatility
- Virilizing adrenal tumors: Androgen excess
F. Drug-Induced Amenorrhea
| Drug Class | Examples |
|---|---|
| Antipsychotics | Phenothiazines, haloperidol, risperidone, clozapine |
| Antidepressants | TCAs, MAOIs |
| Antihypertensives | Methyldopa, reserpine, calcium channel blockers |
| Drugs with estrogenic activity | Digitalis, marijuana, OCP |
| Ovarian toxins | Busulfan, chlorambucil, cisplatin, cyclophosphamide |
Diagnostic Evaluation - Decision Tree
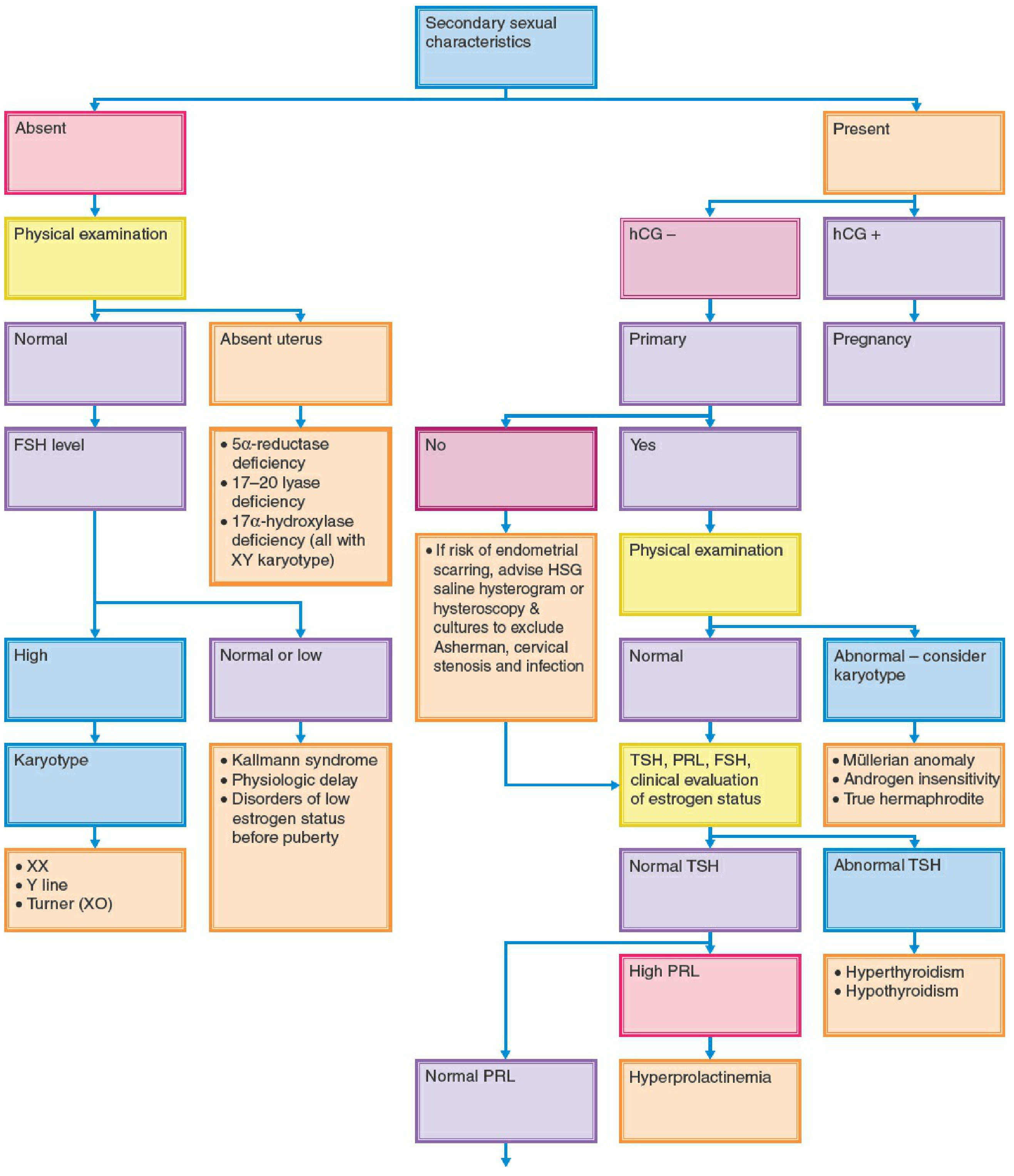
Key Investigations
- Serum/urine beta-hCG - exclude pregnancy first
- TSH - thyroid dysfunction
- Serum prolactin - hyperprolactinemia (fasting sample, early follicular phase)
- Serum FSH + estradiol - differentiate hypergonadotropic vs hypogonadotropic
- Karyotype - if primary amenorrhea with gonadal failure <25 years or height <5 ft
- Pelvic ultrasound - antral follicle count, uterine/ovarian morphology
- MRI pituitary - if elevated prolactin, hypothalamic amenorrhea, or CNS symptoms
- AMH - correlates with follicular pool; aids POI diagnosis
- DEXA scan - bone mineral density if long-term hypoestrogenism suspected
- Progestogen challenge test - limited utility (false positives/negatives common)
Hormone Pattern Summary in Secondary Amenorrhea
| Cause | FSH | LH | Estrogen | Withdrawal bleed |
|---|---|---|---|---|
| Hypothalamic dysfunction (stress/exercise) | ↓ or N | ↓ or N | ↓ or N | ± |
| Anorexia nervosa | ↓ | ↓ | ↓ | - |
| PCOS | N or ↓ | N or ↑ | N | + |
| Hyperprolactinemia | N or ↓ | N or ↓ | ↓ or N | ± |
| Primary ovarian insufficiency | ↑↑ | ↑↑ | ↓ | - |
| Asherman syndrome | N | N | N | - |
Management
Principle: Treat the underlying cause
1. Outflow Tract Obstruction
- Imperforate hymen / vaginal septum: Surgical incision/excision
- MRKH syndrome: Progressive vaginal dilation (Frank's method) or surgical neovaginoplasty; uterus absent so no fertility with own uterus (uterine transplant remains experimental)
- Asherman syndrome: Hysteroscopic lysis of adhesions; barrier (Foley catheter or IUD) + cyclic estrogen-progestin postoperatively
2. PCOS
- Not wanting pregnancy: Combined OCP to regulate cycles and protect endometrium from unopposed estrogen; cyclic progestogens (medroxyprogesterone acetate 10 mg for 12-14 days/month) as alternative
- Insulin resistance: Metformin; weight loss (even 5-10% improves cycles, reduces androgens)
- Wanting pregnancy: Ovulation induction with clomiphene citrate or letrozole (first-line); gonadotropins if clomiphene fails; laparoscopic ovarian drilling
- Screen periodically for diabetes and dyslipidemia
3. Hyperprolactinemia / Prolactinoma
- Dopamine agonists: Cabergoline (preferred) or bromocriptine - reduces prolactin, shrinks tumor, restores ovulation
- Treat hypothyroidism first if both elevated TSH and prolactin are present
- Surgical resection for large macroadenomas not responding to medical therapy
4. Hypothalamic / Functional Amenorrhea
- Exercise-induced: Reduce exercise intensity, increase caloric intake; if hypoestrogenism persists - hormone therapy; calcium 1200-1500 mg/day + Vitamin D 400-800 IU/day
- Anorexia nervosa: Multidisciplinary team; family-based therapy (first-line in adolescents); hospitalization for severe cases; target weight restoration
- Stress-induced: Psychotherapy, stress reduction
- Chronic disease / obesity / Cushing / acromegaly: Specific treatment of underlying disorder
- Note: Bisphosphonates are NOT recommended in amenorrheic athletes (mechanism is decreased bone formation, not increased resorption; also concern about teratogenicity)
5. Primary Ovarian Insufficiency (POI)
- Hormone replacement therapy: Estrogen + progestogen until natural age of menopause (~50 years); doses often higher than standard menopausal HRT
- Bone protection: HRT + calcium + Vitamin D
- Fertility: Oocyte donation is the most reliable option; spontaneous pregnancy possible in 5-10%
- Screen for autoimmune comorbidities: thyroid (TPO antibodies), adrenal (21-hydroxylase antibodies), and screen annually
6. Turner Syndrome
- Estrogen therapy from expected age of puberty (~12-13 years) to initiate secondary sexual characteristics, followed by cyclic estrogen-progestogen
- Growth hormone therapy for short stature
- Cardiac surveillance (coarctation of aorta, bicuspid aortic valve)
- Fertility via donor egg IVF
7. Hypopituitarism / Sheehan Syndrome
- Replace all deficient hormones: estrogen-progestogen, thyroid hormone, glucocorticoids, DDAVP as needed
- MRI pituitary to assess extent of damage
8. Kalllmann Syndrome (wanting pregnancy)
- Pulsatile GnRH therapy via infusion pump, OR
- Gonadotropin injections (FSH + hCG) for ovulation induction
9. Drug-Induced
- Discontinue or substitute offending drug where possible; amenorrhea typically resolves
Key Clinical Pearls
- Always exclude pregnancy before any workup
- When gonadal failure occurs with primary amenorrhea, there is a high incidence of abnormal karyotype - always karyotype
- Bone health must be addressed in all hypoestrogenic patients (osteoporosis risk)
- The distinction between primary and secondary amenorrhea can be misleading - the causes substantially overlap; do not overemphasize the distinction
- FSH >25-40 mIU/mL on two separate samples = hypergonadotropic amenorrhea
- In PCOS: protect endometrium from unopposed estrogen (risk of endometrial hyperplasia/cancer)
- In Asherman syndrome: the patient is hormonally normal but does not menstruate
Clinical Cases on Amenorrhea: Differential Diagnosis, Investigations & Management
Case 1 - 15-year-old girl: Primary amenorrhea + monthly lower abdominal pain
Clinical Interpretation
Most Likely Diagnosis
- Blood accumulates behind the obstruction: hematocolpos (in vagina) → hematometra (in uterus) → hemoperitoneum if reflux through tubes
- If longstanding, can cause endometriosis
Differential Diagnosis
| Diagnosis | Distinguishing feature |
|---|---|
| Imperforate hymen | Bulging bluish/purplish membrane at introitus; most common |
| Transverse vaginal septum | Higher up in vagina; no visible bulge at introitus |
| Cervical agenesis/stenosis | Rare; uterus present but cervix absent/atretic |
| MRKH syndrome | No cyclic pain (no functional uterus/endometrium) |
| Androgen insensitivity | No pain; absent uterus; 46,XY karyotype |
Investigations
- Physical examination - inspection of introitus: bluish bulging membrane at vaginal opening confirms imperforate hymen
- Pelvic ultrasound - hematocolpos (fluid-filled vagina), hematometra; normal ovaries
- MRI pelvis - gold standard for defining anatomy (level of obstruction, uterine/cervical anatomy)
- Beta-hCG - always rule out pregnancy
- Karyotype if anatomy unclear or uterus absent
Management
- Surgical: Cruciate incision of the hymen (hymenotomy) under general anaesthesia with drainage of retained blood (hematocolpos)
- Post-op: spontaneous menstruation establishes; fertility is preserved
- Monitor for endometriosis as a long-term sequela of retrograde menstruation
- Do NOT needle aspirate without surgical backup (risk of infection)
Case 2 - 16-year-old girl: No menarche attained (Primary amenorrhea, no other details given)
Clinical Interpretation
Differential Diagnosis
| Diagnosis | Key Feature |
|---|---|
| Turner syndrome (45,X) | Short stature, webbed neck, shield chest, streak ovaries, HIGH FSH |
| Kallmann syndrome | Anosmia + low FSH/LH + low estrogen |
| Gonadal dysgenesis (46,XX or 46,XY) | Streak gonads, elevated FSH |
| Hypopituitarism | Low FSH, LH, estrogen; may have midline defects |
| Constitutional delay | Diagnosis of exclusion; family history |
| Diagnosis | Key Feature |
|---|---|
| MRKH syndrome | Absent uterus/vagina; 46,XX; normal breasts/hair; normal hormones |
| Androgen Insensitivity (Complete - CAIS) | 46,XY; well-developed breasts; absent/sparse pubic hair; absent uterus |
| Transverse vaginal septum / imperforate hymen | With cyclic pain (see Case 1) |
| PCOS | May present as primary amenorrhea in some |
| Hypothyroidism | Weight gain, cold intolerance |
Investigations Algorithm
- Serum FSH, LH, estradiol
- High FSH → Karyotype (Turner, gonadal dysgenesis)
- Low FSH/LH + no uterus on US → Kallmann, physiologic delay
- Pelvic exam + ultrasound - uterus present or absent?
- Absent uterus → Karyotype (46,XX = MRKH; 46,XY = CAIS)
- Uterus present, no anatomic obstruction → TSH, prolactin, FSH
- If FSH elevated → karyotype, AMH, autoimmune screen (POI)
- If FSH low/normal + low estrogen → MRI brain (Kallmann, pituitary tumour)
- If FSH normal, estrogen normal → rule out PCOS (testosterone, LH:FSH ratio, pelvic US)
Management (depends on diagnosis)
- Turner syndrome: Estrogen therapy to induce puberty → combined HRT; GH therapy for stature; fertility via oocyte donation; cardiac surveillance
- MRKH: Vaginal dilators (Frank's method) or surgical neovaginoplasty; uterus absent so surrogacy
- CAIS: Gonadectomy (gonadoblastoma risk with intra-abdominal testes); estrogen replacement; vaginal dilation
- Kallmann: Pulsatile GnRH or gonadotropin therapy if pregnancy desired; HRT otherwise
- Constitutional delay: Watchful waiting; low-dose estrogen may be considered if distressing
Case 3 - 24-year-old married woman: 3 months absent menses, previously regular cycles
Clinical Interpretation
Differential Diagnosis (in order of probability)
| Diagnosis | Clues to look for |
|---|---|
| Pregnancy (most common) | Nausea, breast tenderness, positive beta-hCG |
| PCOS | Weight gain, hirsutism, acne, oligomenorrhea history |
| Hypothyroidism | Fatigue, weight gain, cold intolerance, constipation, dry skin |
| Hyperprolactinemia | Galactorrhea, headache, visual disturbance |
| Functional hypothalamic amenorrhea | Stress, weight loss, excessive exercise, eating disorder |
| Asherman syndrome | Prior D&C, postpartum curettage, uterine infection |
| Primary ovarian insufficiency | Hot flashes, vaginal dryness (premature but possible at 24) |
| Thyroid/adrenal disorders | Cushing features, virilization |
Investigations Algorithm
- TSH - hypothyroidism/hyperthyroidism
- Serum prolactin (fasting, early morning)
- Serum FSH + estradiol
| Finding | Next Step |
|---|---|
| High TSH | Treat hypothyroidism → cycles usually resume |
| High prolactin | MRI pituitary (prolactinoma?) |
| High FSH (>25-40 mIU/mL x2) | Karyotype, FMR1 premutation, autoimmune screen (POI) |
| Low FSH/LH, low estrogen | MRI brain; assess for FHA (stress, exercise, eating) |
| Normal FSH, normal estrogen | Pelvic US (PCOS?), testosterone, DHEA-S; progesterone challenge |
- Progestogen challenge (medroxyprogesterone 10 mg x 5-10 days)
- Withdrawal bleed = adequate estrogen, patent outflow (likely anovulation/PCOS)
- No withdrawal bleed = either hypoestrogenic state OR outflow tract problem (Asherman)
- If no bleed: give estrogen + progestogen - if still no bleed → outflow problem → hysteroscopy
- Testosterone, DHEA-S (PCOS, adrenal causes)
- Pelvic ultrasound (PCOS morphology, ovarian follicle count)
- Saline infusion sonography or hysteroscopy (Asherman suspected)
Management
- Pregnancy: Obstetric care; contraception counselling
- Hypothyroidism: Levothyroxine → cycles resume
- PCOS: OCP for cycle regulation + endometrial protection; metformin for insulin resistance; weight loss; clomiphene/letrozole if fertility desired
- FHA (stress/weight): Address underlying cause; nutrition, psychological support; HRT if hypoestrogenic
- Asherman syndrome: Hysteroscopic adhesiolysis + postoperative estrogen
- POI: HRT (estrogen-progestogen) until age 50; oocyte donation for fertility
Case 4 - 30-year-old woman: Amenorrhea 7 months + galactorrhea + headache
Clinical Interpretation
Pathophysiology
- Prolactinoma secretes excess prolactin
- Prolactin inhibits pulsatile GnRH secretion → reduced FSH/LH → anovulation → amenorrhea
- Prolactin stimulates breast tissue → galactorrhea (even without pregnancy/breastfeeding)
- Tumor mass effect → headache (compression of surrounding structures); if large → bitemporal hemianopia (compression of optic chiasm)
Differential Diagnosis
| Diagnosis | Distinguishing Feature |
|---|---|
| Prolactinoma (most likely) | High prolactin; MRI shows pituitary adenoma |
| Stalk compression from non-functioning pituitary tumor | High prolactin but adenoma does not stain for PRL on histology |
| Drug-induced hyperprolactinemia | Antipsychotics, metoclopramide, methyldopa, TCAs - must take drug history |
| Hypothyroidism | TRH elevates → stimulates prolactin; check TSH |
| Craniopharyngioma | Calcification on imaging; younger patients typically |
| Empty sella syndrome | MRI shows CSF in enlarged sella |
| Chest wall stimulation / renal failure | Rare; exclude clinically |
Investigations
- Serum prolactin (fasting, no recent breast stimulation) - levels >200 ng/mL are virtually diagnostic of prolactinoma; 100-200 ng/mL highly suggestive; 25-100 ng/mL: drug-induced or small microadenoma
- TSH - exclude hypothyroidism as cause of elevated prolactin (treat thyroid first if both abnormal)
- Beta-hCG - rule out pregnancy (physiological hyperprolactinemia)
- MRI pituitary with contrast - gold standard to visualize adenoma, determine size (micro vs macro), assess suprasellar/cavernous extension
- Visual field testing (Goldman perimetry) - if macroadenoma suspected; bitemporal hemianopia suggests optic chiasm compression
- FSH, LH, estradiol, testosterone - assess degree of hypogonadism
- Full pituitary screen - GH, IGF-1, ACTH, cortisol, free T4 if mass is large (panhypopituitarism?)
- Drug history - rule out iatrogenic hyperprolactinemia
Management
First-line: Dopamine Agonist Therapy
- Cabergoline (preferred): 0.25-0.5 mg twice weekly; better tolerated, more effective at normalizing prolactin and shrinking tumor
- Bromocriptine: 1.25-2.5 mg daily, titrated up; cheaper; more side effects (nausea, dizziness, orthostatic hypotension); crosses placenta - historically used in pregnancy
- Both normalize prolactin in ~80-90% of patients, restore ovulation, and cause tumor shrinkage
- If TSH also elevated: treat hypothyroidism first - prolactin often normalizes
If wanting pregnancy:
- Dopamine agonist (usually switched to bromocriptine in pregnancy if needed) → ovulation restored
- Cabergoline/bromocriptine generally discontinued once pregnancy confirmed (for microadenomas)
- Macroadenomas: continued monitoring with visual fields; reinstate dopamine agonist if tumor expansion occurs
Second-line: Transsphenoidal surgery
- Indications: resistance/intolerance to dopamine agonists, rapid visual deterioration, apoplexy (sudden tumor hemorrhage/infarction)
- Cure rates ~70-80% for microadenomas, lower for macroadenomas
Radiotherapy
- Third-line; for residual tumor after surgery or when medical/surgical options fail
Monitoring
- Prolactin levels at 1-3 months after starting therapy
- Repeat MRI at 6-12 months
- Visual fields if macroadenoma
Summary Table
| Case | Age | Key Presentation | Most Likely Diagnosis | First Investigation | First-line Treatment |
|---|---|---|---|---|---|
| 1 | 15 yrs | Primary amenorrhea + cyclic pain | Imperforate hymen | Pelvic exam + ultrasound | Surgical hymenotomy |
| 2 | 16 yrs | No menarche ever | Turner / MRKH / CAIS (depends on exam) | Secondary sexual characteristics + hCG + FSH + karyotype | Depends on cause; HRT / dilation / gonadectomy |
| 3 | 24 yrs married | Secondary amenorrhea x3 months | Pregnancy (most common) / PCOS / FHA | Beta-hCG | Treat underlying cause |
| 4 | 30 yrs | Amenorrhea + galactorrhea + headache | Prolactinoma | Serum prolactin + TSH + MRI pituitary | Cabergoline (dopamine agonist) |
A 16-year-old girl presents to the gynecology outpatient department with absence of menstruation. She is accompanied by her mother, who is concerned that all her classmates have attained menarche. She has normal breast development since the age of 12 years but has very little pubic and axillary hair. She denies cyclic abdominal pain. She has no significant medical illness and has achieved normal developmental milestones. History Age: 16 years Chief complaint: Primary amenorrhea No cyclical abdominal pain No history of chronic illness, excessive exercise, eating disorder, or weight loss No galactorrhea, headaches, or visual disturbances No previous surgeries Family history: Mother attained menarche at 13 years
Clinical Case Analysis: 16-year-old with Primary Amenorrhea
Clinching the Diagnosis from the History Alone
| Feature | Significance |
|---|---|
| Primary amenorrhea at 16 | Never menstruated |
| Normal breast development since age 12 | Estrogen exposure is adequate - breast tissue responds to estrogen |
| Very little pubic and axillary hair | Androgen receptor is non-functional - hair in these areas requires androgen action |
| No cyclic abdominal pain | No functional uterus / endometrium (no retrograde blood accumulation) |
| No chronic illness, exercise disorder, eating disorder | Rules out functional hypothalamic amenorrhea |
| No galactorrhea, headache, visual disturbance | Rules out prolactinoma |
| Normal developmental milestones, normal height | Distinguishes from Turner syndrome |
| Mother's menarche at 13 | Rules out constitutional/familial delay |
Diagnosis: Complete Androgen Insensitivity Syndrome (CAIS)
Genetics and Pathophysiology
- Karyotype: 46,XY (genetically male)
- Mutation in the androgen receptor (AR) gene located on the X chromosome - X-linked recessive inheritance
- Defects include complete absence of the AR gene, or mutations disrupting binding domains of the receptor
- The AR is entirely non-functional, so androgens cannot exert any biological effect at the cellular level
Embryological Mechanism
| Structure | What happens | Why |
|---|---|---|
| Gonads (testes) | Develop normally (testes present, not ovaries) | SRY gene on Y chromosome → testicular differentiation |
| Müllerian structures (uterus, tubes, upper vagina) | Absent (regressed) | Testes produce Müllerian Inhibiting Substance (MIS/AMH) → normal regression |
| Wolffian structures (vas deferens, seminal vesicles) | Absent | Require functional androgen receptor to develop - AR is non-functional |
| External genitalia | Female phenotype | Androgen receptor non-functional → no virilization of genital tubercle/labioscrotal folds → default female phenotype |
| Pubic/axillary hair | Absent/sparse | Androgen-dependent secondary hair requires functional AR |
| Breasts | Well developed | Peripheral aromatase converts testosterone (which is in male-range) → estradiol → stimulates breast development |
| Vagina | Blind vaginal pouch (shortened, no uterus beyond it) | Müllerian structures absent |
Clinical Features
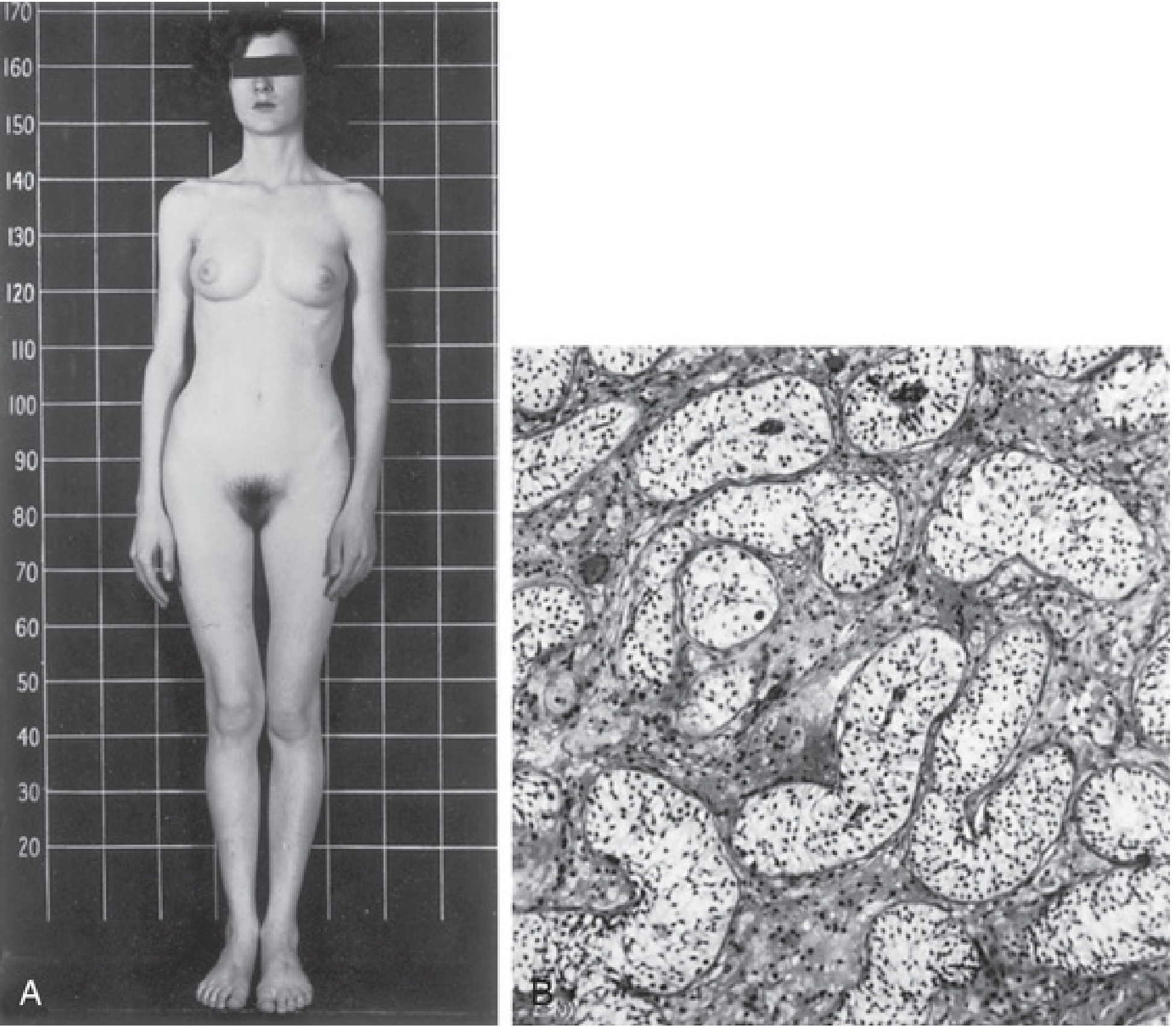
- Female external genitalia - unambiguous female appearance
- Well-developed breasts - but with pale areolae and immature nipples
- Absent/very sparse pubic and axillary hair - pathognomonic
- Blind vaginal pouch - vagina present but shortened, ends blindly
- No uterus, no fallopian tubes (müllerian structures absent)
- Testes - located in abdomen, inguinal canal, or labia majora (may be palpable as inguinal lumps; ~1% of all prepubertal girls with inguinal hernia have CAIS)
- Tall stature with eunuchoidal body proportions (long limbs, big hands and feet)
- Serum testosterone in male range - but biologically inert
Differential Diagnosis
| Diagnosis | Rules In | Rules Out in This Case |
|---|---|---|
| CAIS | Breasts present, absent pubic/axillary hair, no cyclic pain | - |
| MRKH syndrome | Primary amenorrhea, no uterus, no cyclic pain | Pubic/axillary hair normal in MRKH (46,XX); hair here is sparse |
| Turner syndrome (45,X) | Primary amenorrhea, gonadal failure | Normal breast development, normal height and milestones, no stigmata |
| Imperforate hymen | Primary amenorrhea | Cyclic pain present; breasts and hair both normal |
| Functional hypothalamic amenorrhea | No menses | No history of exercise, stress, weight loss; breasts present |
| Prolactinoma | Primary/secondary amenorrhea | No galactorrhea, no headache, no visual symptoms |
| Kallmann syndrome | Primary amenorrhea, hypogonadotropic | Absent secondary sexual characteristics (no breasts); anosmia |
Investigations Algorithm
Step 1 - Exclude pregnancy
- Beta-hCG (urine or serum) - negative in CAIS (blind vaginal pouch, no uterus)
Step 2 - Confirm secondary sexual characteristics
- Physical examination:
- Breast development (Tanner stage)
- Pubic/axillary hair (Tanner stage)
- Genital examination: blind vaginal pouch, absent cervix, absent uterus
- Inguinal examination: palpable gonads?
Step 3 - Imaging
- Pelvic ultrasound (first-line): absent uterus, absent ovaries; may visualize intra-abdominal or inguinal testes
- MRI pelvis (gold standard): confirms absent Müllerian structures, localizes gonads precisely
Step 4 - Hormonal profile
| Test | Expected result in CAIS |
|---|---|
| FSH | Low or normal (testes suppress FSH via inhibin) |
| LH | Elevated (no androgen feedback due to non-functional AR) |
| Testosterone | Male range (300-1000 ng/dL) |
| Estradiol | Normal female range (from aromatization of testosterone) |
| AMH | Elevated (testes actively producing AMH/MIS) |
| Prolactin | Normal |
| TSH | Normal |
Step 5 - Definitive diagnosis
- Karyotype: 46,XY - confirms the diagnosis
- AR gene sequencing - identifies the specific mutation (not always needed clinically but confirms diagnosis)
Step 6 - Associated evaluation
- Bone mineral density (DEXA scan) - baseline before gonadectomy
- Renal ultrasound - usually normal in CAIS (unlike MRKH)
- Psychological assessment - essential before disclosure of karyotype
Management
1. Psychological Support and Counselling (FIRST PRIORITY)
- Sensitive, age-appropriate communication
- Ideally a multidisciplinary team: gynecologist, endocrinologist, psychologist/psychiatrist, social worker
- The patient identifies entirely as female and should be treated accordingly
- Long-term psychological support and peer support groups
2. Gonadectomy (Surgical Removal of Testes)
- ~2-5% lifetime risk of testicular malignancy (gonadoblastoma, dysgerminoma) - most commonly seminomatous germ cell tumors
- Malignant transformation generally does not occur until after puberty
- Therefore, gonadectomy is recommended after pubertal development is complete (to allow testosterone → estradiol conversion to complete breast development naturally)
- Timing debate: Some advocate deferring until adulthood to allow the patient to be fully involved in the decision; recent evidence supports this approach given the low pre-pubertal malignancy risk
- Method: Bilateral laparoscopic gonadectomy (preferred, especially for intra-abdominal testes)
3. Hormone Replacement Therapy (HRT) - Post-Gonadectomy
- Estrogen replacement: Conjugated estrogen or transdermal estradiol, continued until the usual age of menopause (~50 years)
- Maintains secondary sexual characteristics (breasts, skin, vaginal health)
- Prevents osteoporosis (bone protection)
- Cardiovascular and metabolic benefits
- No progestogen needed - uterus is absent, so endometrial protection is not required
- Bone mineral density monitoring with DEXA scan
4. Vaginal Management
- Vagina may be short or inadequate in length
- Progressive vaginal dilation (Frank's method): first-line; self-dilation with progressively larger dilators
- If dilation fails: surgical vaginal lengthening:
- McIndoe procedure (split-thickness skin graft neovaginoplasty)
- Vecchietti procedure
- Intestinal vaginoplasty
- Goal: functional vagina for sexual activity
5. Fertility Counselling
- CAIS patients are sterile (no uterus, no ovaries, intra-abdominal testes produce abnormal sperm if any)
- Cannot carry a pregnancy
- Adoption and surrogacy can be discussed in the future
- Genetic counselling for family members (X-linked recessive - mother may be a carrier)
Summary Flowchart for This Case
16-year-old: Primary amenorrhea
↓
Secondary sexual characteristics?
Breasts: PRESENT (Tanner IV-V)
Pubic/axillary hair: ABSENT/SPARSE
No cyclic pain
↓
Uterus absent on ultrasound
↓
Karyotype → 46,XY
Testosterone → Male range
LH → Elevated
AMH → Elevated
↓
DIAGNOSIS: Complete Androgen Insensitivity Syndrome (CAIS)
↓
Management:
1. Psychological counselling (immediate)
2. Reassure female gender identity
3. Gonadectomy (after puberty is complete / when patient consents)
4. Estrogen HRT (post-gonadectomy, lifelong)
5. Vaginal dilation if needed
6. Long-term follow-up: bone density, psychological support
Key Teaching Points
- Breast development = estrogen exposure. In CAIS, testosterone is aromatized peripherally to estradiol → normal breasts despite 46,XY karyotype
- Absent pubic/axillary hair = non-functional androgen receptor. This is the single most distinguishing feature from MRKH (where hair is normal)
- No uterus = no cyclic pain. Müllerian structures are absent because testes secrete MIS/AMH normally
- Testosterone is in the male range - but biologically inactive due to non-functional AR
- The gonads are testes, not ovaries - located in abdomen/inguinal canal/labia
- AMH is elevated - the most sensitive biochemical marker (active testicular Sertoli cell function)
- This is an X-linked recessive condition - mother is a carrier; 1 in 2 of her 46,XY offspring will be affected