Uterine fibriods
Reading File
Finding Sources
Searching PubMed
"uterine fibroids"[MeSH Terms] AND management
Finding Sources
Searching PubMed
"leiomyoma"[MeSH Terms] AND treatment
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material to write a thorough response. Let me compile everything.
Uterine Fibroids (Leiomyomas)
Definition and Overview
Uterine fibroids (leiomyomas, myomas) are benign, monoclonal tumors of the smooth muscle cells of the myometrium, containing large aggregations of extracellular matrix composed of collagen, elastin, fibronectin, and proteoglycan. They are the most frequent indication for hysterectomy, accounting for nearly 240,000 such procedures annually in the United States alone, with inpatient surgery costing $2.1 billion per year.
Genetic studies confirm that leiomyosarcomas (LMSs) do not arise from malignant degeneration of fibroids - they have distinct genetic profiles with most genes downregulated in LMSs but not in fibroids or myometrium.
Incidence and Epidemiology
Fibroids are remarkably common. Fine serial sectioning of hysterectomy specimens found fibroids in 77% of all uteri, some as small as 2 mm.
- African American women: ~60% incidence by age 35, >80% by age 50
- White women: ~40% by age 35, ~70% by age 50
- Incidence rises sharply with age: 4.3 per 1,000 woman-years at ages 25-29, rising to 22.5 per 1,000 at ages 40-44
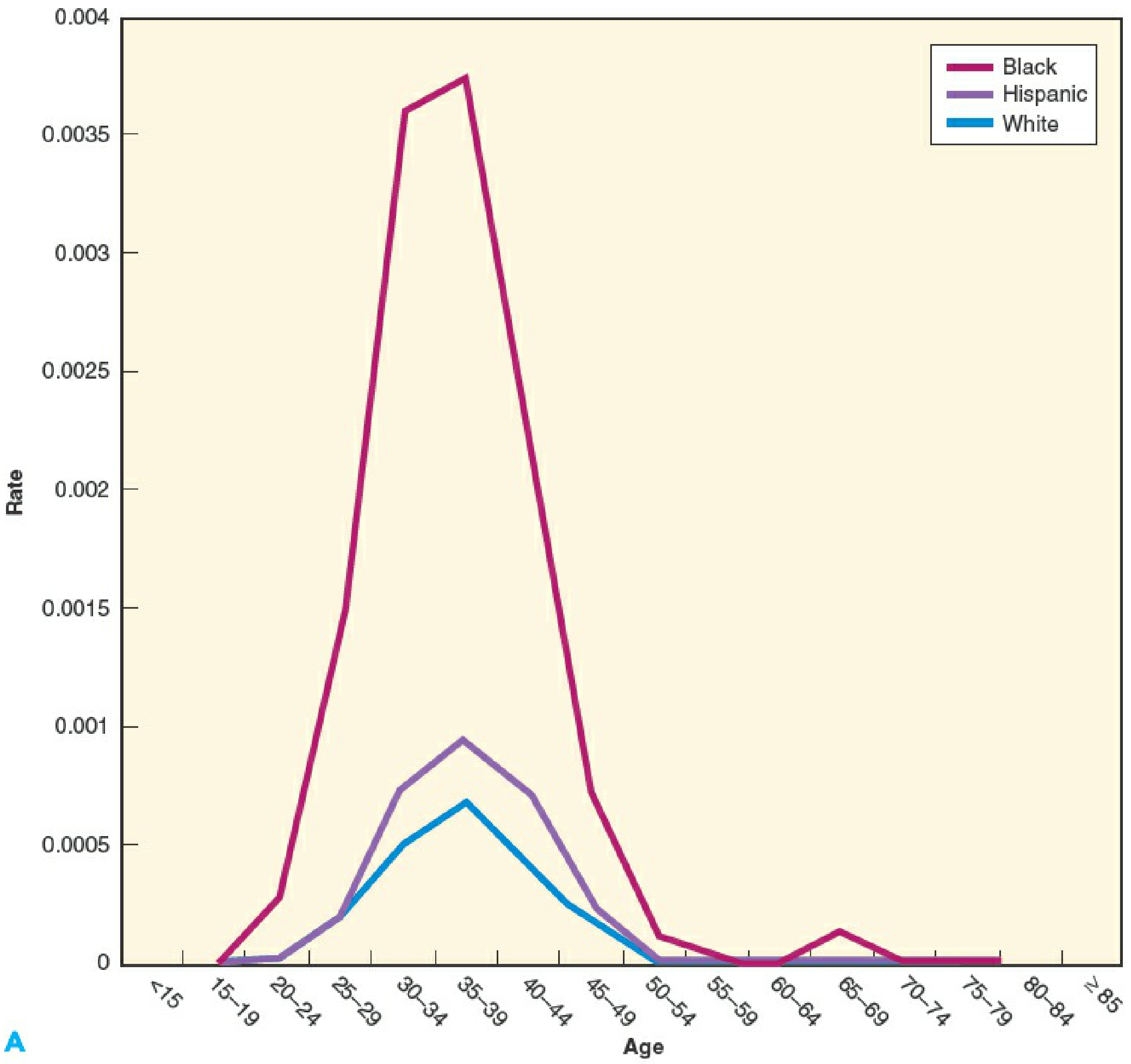
Figure: Age- and race-specific myomectomy rates - Black women are disproportionately affected at younger ages.
Pathophysiology
Hormonal Influence
Estrogen and progesterone both promote fibroid development:
- Fibroids are rare before puberty, peak during reproductive years, and regress after menopause
- Increased aromatase activity within fibroids drives de novo estradiol production higher than in normal myometrium
- Fibroids have increased concentrations of progesterone receptors A and B vs. normal myometrium
- Highest mitotic counts occur at the peak of progesterone production
- GnRH agonists shrink fibroids, but concurrent progestin prevents size reduction
- RU486 (antiprogestin) blocks estradiol + progesterone-driven fibroid growth in animal models
Factors that increase risk (higher estrogen exposure):
- Obesity, early menarche (<10 years), African American ethnicity, nulliparity
Protective factors (decreased estrogen exposure):
- Smoking, regular exercise, increased parity
Growth Factors
Many growth factors are overexpressed in fibroids:
- TGF-β, bFGF - increase smooth muscle proliferation
- EGF, PDGF - increase DNA synthesis
- TGF-β - stimulates extracellular matrix synthesis
- TGF-β, EGF, IGF, prolactin - promote mitogenesis
- bFGF, VEGF - promote angiogenesis
Classification (FIGO System)
The FIGO classification categorizes fibroids by relationship to the endometrium and serosa:
| Type | Description |
|---|---|
| 0 | Pedunculated, entirely intracavitary (submucosal) |
| 1 | Submucosal, <50% intramural diameter |
| 2 | Submucosal, ≥50% intramural diameter |
| 3 | Abuts endometrium, 100% intramural (no cavity component) |
| 4 | Purely intramural |
| 5 | Subserosal, ≥50% intramural |
| 6 | Subserosal, <50% intramural |
| 7 | Subserosal, pedunculated |
| 8 | Other (cervical, broad ligament, parasitic) |
Transmural (hybrid) fibroids are categorized by both relationships (e.g., 2-5 = submucosal + subserosal).
Clinical Features and Symptoms
Heavy Menstrual Bleeding (Most Common)
- Submucosal fibroids are most closely associated with menorrhagia
- Enlargement of the uterine cavity and increased endometrial surface area contribute
- Anemia can result from chronic blood loss
Bulk/Pressure Symptoms
- Pelvic pressure, abdominal distension
- Urinary frequency and urgency (improved ~68% after UAE with 35% volume reduction)
- Constipation, hydronephrosis (rare, from ureteric compression)
Pelvic Pain
- Women with fibroids are only slightly more likely to experience pelvic pain than women without
- Fibroid degeneration (hyaline, cystic, calcific, hemorrhagic) can cause acute or subacute pain
- Torsion of a pedunculated subserosal fibroid causes acute pain requiring surgery
Rapid Growth
- In premenopausal women, "rapid uterine growth" almost never indicates sarcoma - only 1 sarcoma found in 371 women (0.26%) operated on for rapid growth
Natural History
- Most fibroids grow slowly: median growth rate ~9% over 12 months (by MRI)
- Multiple fibroids in the same patient can have highly variable growth rates
- After age 35, growth rates decline with age in White women but not in African American women
- ~7% of fibroids regress spontaneously
Investigations
Ultrasound (First-line)
- Most readily available and least costly
- Reliable for uterine volume <375 cc with ≤4 fibroids
- Appearance: symmetrical, well-defined, hypoechoic, heterogeneous masses
- Calcification/hemorrhage → hyperechoic; cystic degeneration → anechoic
- Saline infusion sonography (SIS) better delineates submucosal fibroids
MRI (Gold Standard for Mapping)
- Best for defining number, size, and precise location relative to endometrium and serosa
- Helps plan surgical approach (hysteroscopic vs. laparoscopic vs. open)
- Distinguishing sarcoma: LMSs show increased gadolinium enhancement (increased vascularity); degenerating fibroids show decreased enhancement
- LDH + LDH isoenzyme 3 + Gd-DTPA MRI: reported 100% specificity and diagnostic accuracy for LMS in one study
- Diffusion-weighted imaging (DWI): lower ADC in LMSs vs. degenerating fibroids (sensitivity 100%, specificity 90% in one study - needs further validation)
Fertility
- Submucosal fibroids decrease fertility; removal increases fertility (ongoing pregnancy/live birth rates reduced ~70% by submucosal fibroids distorting the cavity)
- Subserosal fibroids do not affect fertility; removal does not improve it
- Intramural fibroids may slightly decrease fertility; removal does not clearly improve it
Treatment
Treatment options: watchful waiting, medical therapy, hysteroscopic/laparoscopic/abdominal myomectomy, hysterectomy, uterine artery embolization (UAE), focused ultrasound.
1. Watchful Waiting
- Appropriate for asymptomatic or mildly symptomatic women
- Average fibroid volume increases ~9%/year (range: -25% to +138%)
- 77% of women in one study had no significant change in symptoms at 1 year
- Particularly appropriate as women approach menopause (limited time for new symptoms; fibroids shrink post-menopause)
2. Medical Therapy
| Drug | Mechanism | Effect |
|---|---|---|
| NSAIDs | Prostaglandin inhibition | NOT effective for fibroid-related HMB (unlike idiopathic HMB) |
| Tranexamic acid (1.3 g TID x 3-5 days) | Antifibrinolytic | Significantly reduces menstrual blood loss; headache (55%), nausea (15%) |
| GnRH agonists | Hypogonadal state | Reduces fibroid volume ~30%, uterine volume ~35% in 6 months; rebound to pretreatment size 4-6 months after stopping; side effects in 95% (hot flushes 78%); bone loss limits long-term use |
| GnRH antagonists (e.g., elagolix, relugolix) | Rapid GnRH receptor blockade | Faster effect, no flare-up phenomenon |
| Progestins/levonorgestrel IUD | Endometrial atrophy | Reduces bleeding; may not reduce fibroid size |
| Ulipristal acetate (selective PR modulator) | Modulates progesterone receptors | Reduces bleeding and fibroid size; hepatotoxicity concerns have limited use |
| Aromatase inhibitors | Block estrogen synthesis | Investigational |
GnRH agonists are also used preoperatively to reduce fibroid/uterine size, correct anemia, and reduce surgical blood loss.
3. Surgical Options
Myomectomy (uterus-preserving):
- Indicated for women wishing to preserve fertility or retain uterus
- Safe alternative to hysterectomy even for large fibroids
- Approaches: hysteroscopic (Type 0-2), laparoscopic, robotic, abdominal (open)
- Submucosal fibroids are often removed hysteroscopically
- Uterine rupture risk after myomectomy: ~0.47% (similar to trial of labor after C-section)
- Laparoscopic myomectomy requires meticulous multilayered closure to reduce rupture risk
Hysterectomy (definitive):
- Definitive cure; no risk of recurrence
- ~240,000/year in the US for fibroids
- Appropriate when fertility preservation is not desired and symptoms are severe
4. Uterine Artery Embolization (UAE)
- Effective for selected women; occludes arterial supply to fibroids causing ischemic necrosis
- Reduces uterine volume ~35%, significantly improves bleeding and urinary symptoms
- Effects on fertility and early ovarian failure remain unclear - caution in women desiring pregnancy
5. Focused Ultrasound (MRgFUS)
- Non-invasive thermal ablation guided by MRI
- Emerging option for selected symptomatic fibroids
Key Points Summary
- Fibroids are the most common benign pelvic tumor in women of reproductive age
- Both estrogen and progesterone drive growth - hence regression after menopause
- The FIGO 0-8 classification guides treatment decisions
- Heavy menstrual bleeding + submucosal location = strongest treatment indication
- Rapid growth does not indicate sarcoma in premenopausal women
- MRI + LDH isoenzyme 3 can distinguish sarcoma from degenerating fibroid pre-operatively
- Submucosal fibroids impair fertility; their removal improves outcomes
- Treatment must be individualized: fertility wishes, symptom severity, fibroid location/size, proximity to menopause
Sources: Berek & Novak's Gynecology (Chapter 11); Robbins & Kumar Basic Pathology; recent reviews: Marsh et al. JAMA 2024, Vannuccini et al. Fertil Steril 2024, Donnez et al. Fertil Steril 2024.
This is a shared conversation. Sign in to Orris to start your own chat.