Anatomical Structure of Respiratory System with explanation. Functions of Respiratory System.
Reading File
search_medical_text
anatomical structure of the respiratory system
search_medical_text
functions of the respiratory system gas exchange ventilation
search_medical_image
anatomy of the respiratory system diagram
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive overview of the anatomical structure and functions of the respiratory system.
Respiratory System
Part 1: Anatomical Structure
The respiratory system is organized into two main divisions: the upper respiratory tract and the lower respiratory tract, supported by the thoracic cage and respiratory muscles.
Upper Respiratory Tract
| Structure | Description |
|---|---|
| Nose & Nasal Cavity | The entry point for air. Lined with mucous membrane and cilia that filter, warm, and humidify incoming air. The nasal septum divides it into two chambers. |
| Paranasal Sinuses | Air-filled cavities (frontal, maxillary, ethmoid, sphenoid) that lighten the skull, resonate voice, and produce mucus. |
| Pharynx | A muscular funnel-shaped tube (~13 cm long) shared by both the digestive and respiratory systems. Divided into: Nasopharynx (behind the nasal cavity), Oropharynx (behind the mouth), and Laryngopharynx (leading to the larynx and esophagus). |
| Larynx (Voice Box) | Connects the pharynx to the trachea. Contains the vocal cords (true and false) and the epiglottis — a cartilaginous flap that prevents food from entering the airway during swallowing. Supported by cartilages (thyroid, cricoid, arytenoids). |
Lower Respiratory Tract
| Structure | Description |
|---|---|
| Trachea (Windpipe) | A 10–12 cm tubular passage reinforced by 16–20 C-shaped cartilaginous rings. Extends from the larynx to the carina (at the level of T4–T5) where it bifurcates. |
| Primary (Main) Bronchi | Two branches from the carina — right and left. The right main bronchus is shorter, wider, and more vertical (making it more prone to foreign body aspiration). |
| Secondary (Lobar) Bronchi | Three on the right (for 3 lobes), two on the left (for 2 lobes). |
| Tertiary (Segmental) Bronchi | Supply the bronchopulmonary segments (10 per lung). |
| Bronchioles | Smaller airways (<1 mm diameter) lacking cartilage. Further branch into terminal bronchioles (last conducting zone segment). |
| Respiratory Bronchioles | Transitional zone — begin to have alveoli in their walls; part of the gas-exchange zone. |
| Alveolar Ducts & Alveolar Sacs | Open into clusters of alveoli. |
| Alveoli | Microscopic air sacs (~300 million in both lungs) forming the primary gas-exchange surface (~70 m²). Walls contain Type I pneumocytes (gas exchange), Type II pneumocytes (surfactant production), and pulmonary capillaries. |
This progressive branching from the trachea to alveoli is called the bronchial tree or tracheobronchial tree.
The Lungs
- Right Lung: 3 lobes (upper, middle, lower), divided by horizontal and oblique fissures.
- Left Lung: 2 lobes (upper, lower), divided by the oblique fissure. Has a cardiac notch to accommodate the heart.
- Each lung is enclosed in a double-layered pleura: the visceral pleura (covers lung surface) and the parietal pleura (lines thoracic wall), with a thin film of pleural fluid between them to reduce friction.
Chest Wall & Respiratory Muscles
According to Harrison's Principles of Internal Medicine (p. 7854), the respiratory system is best understood as three independently functioning components:
- The Lung (including its airways)
- The Neuromuscular System (the force-generating component)
- The Chest Wall (everything else — ribs, sternum, diaphragm, abdominal contents)
Key muscles involved:
- Diaphragm — primary muscle of inspiration; contracts and flattens downward to increase thoracic volume.
- External intercostals — elevate ribs during inspiration.
- Accessory muscles (sternocleidomastoid, scalenes) — active during forceful breathing or respiratory distress.
- Internal intercostals & abdominals — muscles of forced expiration.
Anatomical Diagram — Respiratory Tract
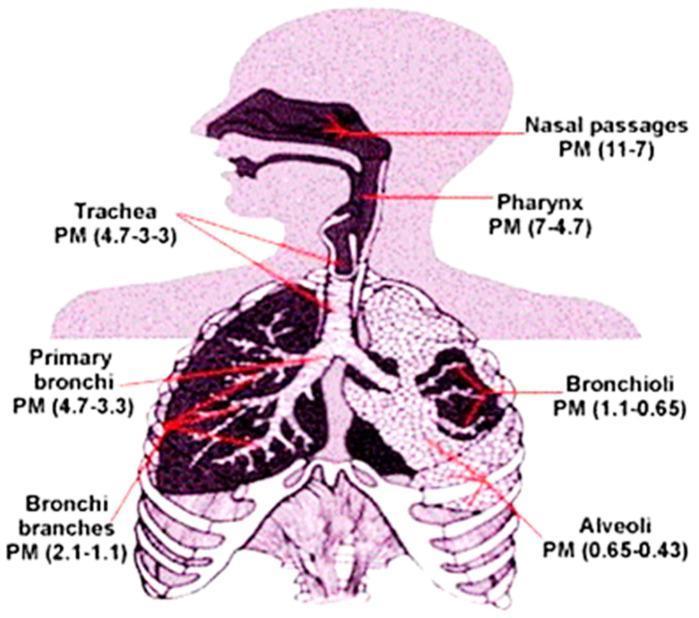
Illustration showing the anatomical regions of the respiratory system from nasal passages through to alveoli, along with particulate matter deposition by region.
Part 2: Functions of the Respiratory System
According to Harrison's Principles of Internal Medicine (p. 7853), the respiratory system performs the following core and accessory functions:
1. Gas Exchange (Primary Function)
The most critical function. Oxygen (O₂) from inhaled air diffuses across the alveolar membrane into pulmonary capillary blood, while carbon dioxide (CO₂) moves in the opposite direction and is exhaled. This occurs across an ultrathin membrane of flattened endothelial and epithelial cells in the alveolar walls. The enormous surface area (~70 m²) packed into the thoracic cavity enables efficient diffusion.
2. Pulmonary Ventilation
The mechanical process of moving air in and out of the lungs:
- Inspiration: Diaphragm contracts → thoracic volume increases → intrapulmonary pressure drops below atmospheric → air flows in.
- Expiration: Diaphragm relaxes → thoracic volume decreases → pressure rises → air flows out. Quiet expiration is passive; forced expiration is active.
3. External Respiration
Exchange of gases between alveolar air and pulmonary capillary blood (O₂ in, CO₂ out) via diffusion down partial pressure gradients.
4. Internal (Tissue) Respiration
Exchange of gases between systemic capillary blood and body tissues — O₂ is delivered to cells and CO₂ produced by cellular metabolism is picked up for transport back to the lungs.
5. Acid-Base Regulation (pH Balance)
By controlling the rate and depth of breathing, the lungs regulate CO₂ levels in the blood. Since CO₂ + H₂O ⇌ H₂CO₃ ⇌ H⁺ + HCO₃⁻, altering CO₂ levels directly influences blood pH — a rapid buffering mechanism complementing the kidneys.
6. Phonation (Voice Production)
Exhaled air passes over the vocal cords in the larynx, causing vibration and producing sound. Pitch is controlled by tension on the vocal cords; volume by airflow.
7. Olfaction (Sense of Smell)
Inhaled air carries odorant molecules to olfactory receptors in the roof of the nasal cavity, enabling the sense of smell.
8. Filtration, Warming & Humidification
- Nasal hairs and cilia trap large particles.
- Mucus traps pathogens and fine particles; the mucociliary escalator moves debris upward for swallowing or expectoration.
- Inspired air is warmed to 37°C and humidified to ~100% relative humidity before reaching the alveoli, protecting delicate alveolar surfaces.
9. Immune Defence
- Alveolar macrophages phagocytose pathogens and foreign particles.
- Secretory IgA in mucus neutralizes microbes in the upper airways.
- The cough and sneeze reflex expel foreign material forcefully.
10. Surfactant Production
Type II pneumocytes in alveolar walls secrete surfactant (dipalmitoylphosphatidylcholine), which reduces surface tension within alveoli, prevents alveolar collapse (atelectasis) at end-expiration, and reduces the work of breathing.
Summary Table
| Function | Anatomical Site | Key Mechanism |
|---|---|---|
| Gas exchange | Alveoli | Diffusion across alveolar membrane |
| Ventilation | Lungs + diaphragm + chest wall | Pressure gradients |
| pH regulation | Lungs (CO₂ control) | Alveolar ventilation rate |
| Voice production | Larynx | Vocal cord vibration |
| Olfaction | Nasal cavity | Olfactory receptors |
| Filtration/humidification | Nose, trachea, bronchi | Mucus, cilia, mucociliary escalator |
| Immune defence | Upper airways, alveoli | Macrophages, IgA, cough reflex |
| Surfactant production | Alveoli (Type II pneumocytes) | Reduces alveolar surface tension |
References:
- Harrison's Principles of Internal Medicine, 21st Edition, p. 7853–7854
This is a shared conversation. Sign in to Orris to start your own chat.