Oral pathology important questions bds
Reading File
Finding Sources
Searching the Web
BDS oral pathology important questions university exam topics
Reading Web Page
https://excelbds.com/question-bank/3rd-year/3rd-year-questio…
Searching the Web
BDS 3rd year oral pathology exam important long short questions ameloblastoma cysts OSCC
Here is a well-organized compilation of BDS Oral Pathology Important Questions covering all major exam topics, based on university question banks (including UHS, RGUHS, TNMGRMU, and other BDS boards):
BDS Oral Pathology - Important Questions
1. DEVELOPMENTAL DISTURBANCES
Long Essays (10 marks)
- Enumerate developmental disturbances of the tongue. Write in detail about geographic tongue.
- Enumerate developmental disturbances affecting the structure of teeth.
- Describe in detail Amelogenesis Imperfecta - types, clinical features, histopathology.
- Write in detail about developmental anomalies affecting the shape of teeth (taurodontism, dens invaginatus, dilaceration, fusion, gemination, concrescence).
- List developmental anomalies of teeth w.r.t. structure. Give a detailed account on Dentinogenesis Imperfecta.
- Enumerate environmental causes for enamel hypoplasia. Write in detail.
Short Essays (5 marks)
- Taurodontism
- Enamel hypoplasia
- Anodontia / hypodontia
- Macrodontia and microdontia
- Supernumerary teeth (mesiodens)
- Fluorosis
Short Answers (2 marks)
- Turner's tooth
- Natal and neonatal teeth
- Talon cusp
- Dens in dente
2. DENTAL CARIES
Long Essays
- Write in detail about the zones of enamel caries and dentinal caries.
- Write in detail the histopathology of dental caries.
- Discuss etiopathogenesis of dental caries (Keyes triad, acidogenic theory).
- Clinical types of dental caries.
Short Essays
- Arrested caries
- Rampant caries
- Nursing bottle caries
- Remineralization
- Microbiology of dental caries (Streptococcus mutans role)
Short Answers
- Sclerotic dentin
- Dead tracts
- Tertiary dentin
- Transparent zone of enamel caries
3. PULP AND PERIAPICAL PATHOLOGY
Long Essays
- Classify pulpitis. Write in detail acute and chronic pulpitis (clinical features, histopathology).
- Write in detail about pathogenesis, clinical features, radiographic features, and histopathology of apical periodontal (radicular) cyst.
- Compare and contrast acute and chronic periapical abscess.
Short Essays
- Pulp stones (denticles)
- Acute apical periodontitis
- Periapical granuloma
- Phoenix abscess
- Internal resorption
Short Answers
- Pulp polyp
- Cellulitis
- Osteomyelitis
4. PERIODONTAL PATHOLOGY
Long Essays
- Write in detail about the pathogenesis and histopathology of chronic periodontitis.
- Classify periodontal diseases. Describe juvenile periodontitis.
Short Essays
- Gingival fibromatosis
- Desquamative gingivitis
- ANUG (Acute Necrotizing Ulcerative Gingivitis)
- Gingival enlargement due to drugs (Phenytoin/Nifedipine/Cyclosporine)
Short Answers
- Junctional epithelium
- Periodontal pocket
- Gingival crevicular fluid
5. ORAL MUCOSAL LESIONS / POTENTIALLY MALIGNANT DISORDERS
Long Essays (Most Important)
- Define leukoplakia. Classify it. Discuss its malignant potential. Add a note on histopathology.
- Discuss in detail etiopathogenesis, clinical features, and histopathology of OSCC (Oral Squamous Cell Carcinoma).
- Write in detail about etiology, clinical features, and histopathology of Oral Submucous Fibrosis (OSMF).
- Write in detail clinical features and histopathology of SCC (non-odontogenic malignant epithelial neoplasm).
- Describe clinical features and histopathology of verrucous carcinoma.
Short Essays
- Erythroplakia
- Epithelial dysplasia (grades)
- Grading and staging of OSCC
- TNM staging of oral cancer
- Frictional keratosis
- Lichen planus - oral manifestations
- Aphthous ulcers (RAU) - types and management
Short Answers
- Speckled leukoplakia
- Nicotinic stomatitis
- Sanguinaria-associated keratosis
- Proliferative verrucous leukoplakia
6. ODONTOGENIC CYSTS (Very High Yield)
Long Essays
- Classify odontogenic cysts. Write in detail the clinical features, radiographic features, and histopathology of Dentigerous (Follicular) Cyst.
- Classify cysts of the orofacial region. Describe in detail OKC (Odontogenic Keratocyst). Add a note on causes of its recurrence.
- Classify odontogenic cysts. Describe pathogenesis, clinical features, radiographic features, and histopathology of Radicular (Apical Periodontal) Cyst.
- Describe Gorlin-Goltz Syndrome (Nevoid Basal Cell Carcinoma Syndrome) and its relation to OKC.
Short Essays
- Lateral periodontal cyst
- Nasopalatine duct cyst (Incisive canal cyst)
- Gingival cyst of newborn (Epstein's pearls / Bohn's nodules)
- Calcifying odontogenic cyst (COC / Gorlin cyst)
- Eruption cyst
- Nasolabial cyst
Short Answers
- Stellate reticulum-like epithelium (OKC lining)
- Ghost cells (COC)
- Rushton bodies
- Daughter cysts
7. ODONTOGENIC TUMORS (Most Important)
Long Essays
- Enumerate benign odontogenic tumours. Write in detail about clinical features, radiographic features, and histopathology of Follicular Ameloblastoma.
- Classify odontogenic tumours. Write in detail clinical features, radiographic features, and histopathology of Ameloblastoma (all types - follicular, plexiform, acanthomatous, granular cell, basal cell, desmoplastic).
- Describe Odontoma - types (compound and complex), clinical, radiographic, and histopathological features.
- Write in detail about Ameloblastic Fibroma and Ameloblastic Fibro-odontoma.
- Describe clinical and histopathological features of Adenomatoid Odontogenic Tumour (AOT).
- Write about Calcifying Epithelial Odontogenic Tumour (CEOT / Pindborg Tumour).
Short Essays
- Cementoblastoma
- Odontogenic myxoma
- Squamous odontogenic tumour
- Ameloblastic carcinoma
- CCOT (Clear Cell Odontogenic Tumour)
Short Answers
- Stellate reticulum in ameloblastoma
- Tombstone cells
- Liesegang rings (CEOT)
- Enamel matrix proteins
8. NON-ODONTOGENIC TUMORS & GIANT CELL LESIONS
Long Essays
- Enumerate giant cell lesions. Write in detail the pathogenesis and histopathology of Aneurysmal Bone Cyst (ABC).
- Describe clinical features and histopathology of Central Giant Cell Granuloma (CGCG).
- Enumerate benign connective tissue tumours. Write about Fibroma, Lipoma, Neurofibroma.
- Classify nerve tissue tumours. Write about Neurofibromatosis (von Recklinghausen's disease).
Short Essays
- Fibroma
- Pyogenic granuloma
- Peripheral giant cell granuloma
- Osteosarcoma
- Ewing's sarcoma
- Keratoacanthoma
- Nevus
- Reed-Sternberg cells (Hodgkin's lymphoma)
Short Answers
- Haemangioma
- Lymphangioma
- Ossifying fibroma
- Osteoma (Gardner syndrome)
9. SALIVARY GLAND PATHOLOGY (High Yield)
Long Essays
- Enumerate benign salivary gland tumours. Describe pathogenesis, clinical features, and histopathology of Pleomorphic Adenoma (Mixed Tumour).
- Enumerate malignant salivary gland tumours. Write in detail about Mucoepidermoid Carcinoma.
- Classify tumours of salivary glands. Write in detail about Adenoid Cystic Carcinoma (cribriform/cylindromatous/tubular patterns).
- Classify salivary gland tumours. Write about Warthin's Tumour (Papillary Cystadenoma Lymphomatosum).
Short Essays
- Mucous extravasation phenomenon (ranula, mucocele)
- Mucous retention cyst
- Sialolithiasis (salivary calculus)
- Sjogren's syndrome
- Xerostomia
- Histopathology of adenoid cystic carcinoma
- Histopathology of mucoepidermoid carcinoma
Short Answers
- Stensen's duct
- Epimyoepithelial islands (Sjogren's)
- Tyrosine crystals (pleomorphic adenoma)
10. INFECTIONS / MICROBIOLOGY IN ORAL PATHOLOGY
Long Essays
- Classify viral infections. Describe oral manifestations of Herpes simplex (HSV-1) infection.
- Write in detail about oral candidiasis - types, lab diagnosis, histopathology.
Short Essays
- Herpes zoster and Ramsay Hunt syndrome
- Oral manifestations of syphilis (primary, secondary, tertiary)
- Oral manifestations of HIV/AIDS
- Acute pseudomembranous candidiasis (Thrush)
- Types of oral candidiasis
- Paul-Bunnell test (infectious mononucleosis)
Short Answers
- Lipshutz bodies (herpetic vesicles)
- Ballooning degeneration
- Sulphur granules (actinomycosis)
- Tzanck cells
- Ray fungus (Actinomyces)
- Treponema pallidum
- Candida albicans identification
11. BLOOD DISORDERS & ORAL MANIFESTATIONS
Short Essays
- Oral and lab findings in iron deficiency anemia
- Oral manifestations of leukemia
- Oral manifestations of thrombocytopenia
- Polycythemia vera - oral features
Short Answers
- Plummer-Vinson syndrome
- Pernicious anemia (B12 deficiency)
- Sickle cell anemia - oral features
12. BONE PATHOLOGY
Long Essays
- Describe Paget's disease of bone - etiology, clinical, radiographic, lab, and histopathological features.
- Write about Fibrous Dysplasia (monostotic vs. polyostotic) - clinical, radiographic, histopathological features.
Short Essays
- Cherubism
- Hyperparathyroidism (Brown tumor)
- Osteoporosis - oral implications
- Garré's osteomyelitis
- Ossifying fibroma
Short Answers
- Ground glass appearance (fibrous dysplasia)
- Cotton wool appearance (Paget's disease)
- Sun-ray appearance (osteosarcoma)
- Sunburst pattern
13. MISCELLANEOUS / SYNDROMES
Short Essays
- Gorlin-Goltz syndrome (multiple OKCs + basal cell carcinomas)
- Albright's syndrome (polyostotic fibrous dysplasia + McCune-Albright)
- Pierre Robin sequence
- James Ramsay Hunt syndrome
- Sjogren's syndrome
- Gardner's syndrome (intestinal polyps + osteomas)
- Marfan syndrome - oral features
- Down syndrome - oral features
14. DIAGNOSTIC TECHNIQUES
Short Essays
- Biopsy - types and procedure (incisional, excisional, punch, fine needle aspiration)
- Exfoliative cytology - procedure and interpretation
- Immunohistochemistry in oral pathology
- Flow cytometry
Short Answers
- Papanicolaou stain
- Toluidine blue staining
- PAS stain (for fungi)
QUICK REFERENCE: MOST REPEATED LONG ESSAY TOPICS
| Rank | Topic |
|---|---|
| ★★★ | Ameloblastoma (all types) |
| ★★★ | OKC - classification, features, recurrence |
| ★★★ | OSCC - etiopathogenesis, clinical, histopathology |
| ★★★ | Radicular cyst |
| ★★★ | Pleomorphic adenoma |
| ★★★ | Dental caries histopathology |
| ★★★ | OSMF |
| ★★★ | Dentigerous cyst |
| ★★ | Amelogenesis imperfecta / Dentinogenesis imperfecta |
| ★★ | Mucoepidermoid carcinoma |
| ★★ | Adenoid cystic carcinoma |
| ★★ | Chronic periodontitis |
| ★★ | Paget's disease / Fibrous dysplasia |
| ★★ | Oral candidiasis |
| ★★ | ABC / CGCG |
KEY ONE-LINERS TO REMEMBER
- Most common odontogenic cyst: Radicular cyst
- Most common odontogenic tumor: Ameloblastoma
- OKC is now called: Keratocystic Odontogenic Tumour (KCOT) by WHO 2005 (reverted back to OKC in WHO 2022 classification)
- Standard treatment of ameloblastoma: Resection with 1-1.5 cm margin
- Multiple bilateral dentigerous cysts: Gorlin-Goltz syndrome
- COC is also called: Gorlin cyst or Calcifying Ghost Cell Odontogenic Cyst
- Bimanual palpation positive for: Ranula, salivary gland swellings
- Liesegang rings: CEOT (Pindborg tumour)
- Cotton wool bone: Paget's disease
- Sun-ray/sunburst pattern: Osteosarcoma
This covers the full scope of BDS 3rd year Oral Pathology across all major Indian universities (RGUHS, UHS, TNMGRMU, MU, KU, etc.). Focus especially on the ★★★ topics for long essays, and know the histopathology of every major lesion - that is the most commonly asked angle in university exams.
Rguhs
Searching the Web
RGUHS BDS oral pathology previous year question papers 3rd year important questions
Searching the Web
RGUHS oral pathology BDS question bank long essays short notes repeated questions
Reading Web Page
https://www.studocu.com/in/document/rajiv-gandhi-university-…
Searching the Web
RGUHS BDS oral pathology microbiology 2022 2023 2024 question paper PDF
Reading Web Page
https://www.scribd.com/document/916983932/Bds-1188-Oral-Path…
Here is a comprehensive, RGUHS-specific Oral Pathology & Microbiology important questions list, compiled from actual RGUHS question papers (QP Code: 1188, III BDS) across multiple years (2019-2025):
RGUHS BDS - Oral Pathology & Microbiology (QP Code: 1188)
III BDS | Total Marks: 70 | Pattern: 2 Long Essays (10M each) + 8 Short Essays (5M each) + Short Answers (2M each)
EXAM PATTERN (RGUHS)
| Section | Questions | Marks |
|---|---|---|
| Long Essays | 2 × 10 = | 20 marks |
| Short Essays | 8 × 5 = | 40 marks |
| Short Answers | 5 × 2 = | 10 marks |
| Total | 70 marks |
LONG ESSAYS - MOST REPEATED (10 marks each)
These are the questions that appear repeatedly in RGUHS papers. Prepare ALL of them:
Odontogenic Tumors & Cysts (Most Frequently Asked)
- Classify odontogenic tumors. Write in detail about the clinical features, radiographic features, and histopathology of Ameloblastoma. (Appears almost every year)
- Classify odontogenic cysts. Describe in detail OKC (Odontogenic Keratocyst) - clinical features, radiographic features, histopathology, and causes of recurrence.
- Classify odontogenic cysts. Write in detail about pathogenesis, clinical features, radiographic features, and histopathology of Radicular (Apical Periodontal) Cyst.
- Classify odontogenic cysts. Write in detail about clinical features, radiographic features, and histopathology of Dentigerous (Follicular) Cyst.
Salivary Gland Tumors
- Classify salivary gland neoplasms. Write in detail about the clinical features and histopathology of Pleomorphic Adenoma.
- Classify salivary gland tumors. Write in detail about Adenoid Cystic Carcinoma (cribriform, tubular, solid patterns; perineural invasion; prognosis).
- Classify salivary gland tumors. Write in detail about Mucoepidermoid Carcinoma (grading - low/intermediate/high; histopathology).
Oral Cancer / Mucosal Lesions
- Classify non-odontogenic epithelial tumors. Write in detail about clinical features and histopathology of Oral Squamous Cell Carcinoma (OSCC). (2025 paper confirmed)
- Enumerate various dermatological disorders affecting the oral mucosa. Describe clinical features and histopathology. (2024 paper confirmed)
- Define leukoplakia. Classify it. Write in detail about etiopathogenesis, clinical features, histopathology, and malignant potential.
- Write in detail about etiology, clinical features, and histopathology of Oral Submucous Fibrosis (OSMF).
Dental Caries & Pulp
- Write in detail about histopathology of dental caries (enamel caries zones - translucent, dark, body of lesion, surface zone; dentinal caries zones).
- Classify pulpitis. Describe clinical features and histopathology of acute and chronic pulpitis.
Bone Pathology / Giant Cell Lesions
- Enumerate giant cell lesions of the jaws. Write in detail about pathogenesis and histopathology of Aneurysmal Bone Cyst (ABC).
- Write in detail about clinical features, radiographic features, laboratory findings, and histopathology of Paget's disease of bone.
- Describe clinical features, radiographic features, and histopathology of Fibrous Dysplasia.
Developmental Disturbances
- Enumerate developmental disturbances affecting the structure of teeth. Write in detail about Amelogenesis Imperfecta.
- List developmental anomalies of teeth. Write in detail about Dentinogenesis Imperfecta.
SHORT ESSAYS - FREQUENTLY ASKED (5 marks each)
Prepare these as 1-page answers with a labeled diagram wherever applicable:
Oral Pathology Topics
| Topic | Frequency |
|---|---|
| Histopathology of Ameloblastoma (follicular type) | ★★★ Very High |
| Odontogenic Keratocyst (OKC) features | ★★★ Very High |
| Erythroplakia | ★★★ Very High |
| Epithelial dysplasia (grades) | ★★★ Very High |
| Pulp stones (denticles) | ★★ High |
| Warthin's tumour | ★★ High |
| Mucoepidermoid carcinoma | ★★ High |
| Pyogenic granuloma | ★★ High |
| Peripheral giant cell granuloma | ★★ High |
| Calcifying Epithelial Odontogenic Tumour (CEOT/Pindborg) | ★★ High |
| Adenomatoid Odontogenic Tumour (AOT) | ★★ High |
| Sialolithiasis | ★★ High |
| Sjogren's syndrome | ★★ High |
| Mucous extravasation phenomenon (Mucocele/Ranula) | ★★ High |
| Cleidocranial dysplasia | ★★ High |
| Cherubism | ★★ High |
| Central giant cell granuloma | ★★ High |
| Cementoblastoma | ★★ High |
| Oral candidiasis (types) | ★★ High |
| Oral manifestations of HIV/AIDS | ★★ High |
| Lichen planus (oral) | ★★ High |
| Geographic tongue | ★★ High |
| Supernumerary teeth | ★★ High |
| Ludwig's angina | ★★ High |
| Nasopalatine duct cyst | ★ Moderate |
| Fibroma | ★ Moderate |
| Nevus | ★ Moderate |
| Keratoacanthoma | ★ Moderate |
| TNM staging of OSCC | ★ Moderate |
| Grading & staging of OSCC | ★ Moderate |
| Verrucous carcinoma | ★ Moderate |
Oral Microbiology Topics (Part of Same Paper in RGUHS)
| Topic | Frequency |
|---|---|
| Normal flora of the oral cavity | ★★★ Very High |
| Role of Streptococcus mutans in dental caries | ★★★ Very High |
| Oral manifestations of acquired syphilis | ★★ High |
| Herpes simplex - oral manifestations | ★★ High |
| Lab diagnosis of oral candidiasis | ★★ High |
| Actinomycosis | ★★ High |
| Erythema multiforme | ★★ High |
| Bacteremia and focal infection | ★ Moderate |
| Sterilization and disinfection (dental) | ★ Moderate |
SHORT ANSWERS - COMMONLY ASKED (2 marks each)
Know the definition/one key fact for each:
Oral Pathology:
- Rushton bodies (hyaline bodies in radicular cyst epithelium)
- Ghost cells (COC - Calcifying Odontogenic Cyst)
- Liesegang rings (CEOT - Pindborg tumour)
- Stellate reticulum (ameloblastoma)
- Tombstone appearance (ameloblastoma)
- Ground glass appearance (fibrous dysplasia)
- Cotton wool pattern (Paget's disease)
- Sunburst/sun-ray pattern (osteosarcoma)
- Soap bubble appearance (ameloblastoma / giant cell tumour)
- Compound and complex odontoma
- Aneurysmal bone cyst
- Nasolabial cyst
- Gorlin-Goltz syndrome (multiple OKCs)
- Cleidocranial dysplasia
- Gardner syndrome
Oral Microbiology:
- Tzanck cells
- Ballooning degeneration
- Lipshutz bodies
- Sulphur granules (actinomycosis)
- Paul-Bunnell test
- Koplik's spots
- Candida albicans
- ANUG causative organisms (Borrelia vincenti + Fusobacterium)
RGUHS CONFIRMED QUESTIONS (from actual papers)
2025 (March) - QP 1188
- Long Essay: Enumerate non-odontogenic epithelial tumors. Write in detail about clinical and histopathological features of one malignant tumor.
- Long Essay: Classify cysts of the orofacial region. Describe in detail one odontogenic cyst.
- Short Essays: (included topics from the dermatological disorders + salivary gland questions)
2024 (October) - QP 1188
- Long Essay 1: Enumerate various dermatologic disorders affecting the oral mucosa.
- Long Essay 2: Classify salivary gland neoplasms. Describe clinical and histopathological features.
- Short Essay: Histopathology of ameloblastoma
- Short Essay: Pulp polyp
2021 - RGUHS
- Long Essay 1: Classify odontogenic tumors. Write in detail about Ameloblastoma.
- Long Essay 2: Classify salivary gland tumors. Write in detail about Adenoid Cystic Carcinoma.
- Short Essays: Supernumerary teeth, Sialolithiasis, OKC features, Erythema multiforme, Ludwig's angina, Normal oral flora, Cleidocranial dysplasia, Oral manifestations of acquired syphilis.
STRATEGY FOR RGUHS ORAL PATHOLOGY
Must-prepare Long Essays (can appear any year):
- Ameloblastoma
- OKC / Radicular cyst / Dentigerous cyst
- Pleomorphic adenoma / Adenoid cystic carcinoma / Mucoepidermoid carcinoma
- OSCC / Leukoplakia / OSMF
- Dental caries histopathology
- ABC / CGCG / Paget's disease / Fibrous dysplasia
- Amelogenesis imperfecta / Dentinogenesis imperfecta
- Dermatological disorders of oral mucosa (Pemphigus, Pemphigoid, Lichen planus, Erythema multiforme)
Golden Rule for RGUHS: Every answer must have:
- A classification if asked
- Clinical features (age, sex, site, presenting complaint)
- Radiographic features (shape, margins, cortication, effect on teeth)
- Histopathology (cell types, patterns, special features)
- A labeled diagram
Good luck for your RGUHS exams! The Ameloblastoma + OKC/Radicular cyst + Pleomorphic adenoma trio is the most consistent combination across years - never skip those three.
Answers according to standard textbooks
Asking for Preferences
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Here is the complete, textbook-based answer for Ameloblastoma - structured exactly as RGUHS expects (Classification → Clinical → Radiographic → Histopathology → Treatment):
AMELOBLASTOMA
(Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery | Cummings Otolaryngology | KJ Lee's Essential Otolaryngology)
DEFINITION
Ameloblastoma is a benign but locally aggressive odontogenic neoplasm arising from the epithelial elements of the tooth-forming apparatus (rests of dental lamina, reduced enamel epithelium, epithelial lining of odontogenic cysts). Though histologically benign, it is locally invasive and has a high recurrence rate if inadequately treated.
- Scott-Brown's Otorhinolaryngology
CLASSIFICATION (WHO 2022)
| Type | Key Features |
|---|---|
| 1. Conventional (Solid/Multicystic) Ameloblastoma | Most common; locally invasive; high recurrence |
| 2. Unicystic Ameloblastoma (UA) | Unilocular cystic; younger age group; better prognosis |
| 3. Peripheral (Extra-osseous) Ameloblastoma | Arises in soft tissue of gingiva; does not invade bone |
| 4. Metastasizing Ameloblastoma | Histologically benign but distant metastasis occurs - retrospective diagnosis |
| Malignant variant | Ameloblastic carcinoma - cellular atypia present |
Histological subtypes of Conventional type: Follicular, Plexiform, Acanthomatous, Granular cell, Desmoplastic, Basal cell
- KJ Lee's Essential Otolaryngology
1. CONVENTIONAL (SOLID/MULTICYSTIC) AMELOBLASTOMA
A. CLINICAL FEATURES
- Age: All age groups affected; mean age ~37 years; most common in 3rd-5th decade
- Sex: Male:Female ratio = 1.2:1 (slight male predilection)
- Site: Mandible in ~85% of cases; mandibular molar-ramus region is the most common site. Mandible:Maxilla ratio = 5:1
- Presentation:
- Slow, painless expansion of the jaw - the hallmark
- In early stages - few clinical signs (centrally located within bone)
- Later: increasing facial deformity, loosening of teeth
- Eggshell crackling on palpation (thinned cortical bone)
- Bone perforation and spontaneous jaw fracture in advanced cases
- Occasional root resorption of adjacent teeth
- Genetics: Mutations in the MAPK pathway (especially BRAF V600E mutation) observed in ~90% of all lesions
- Scott-Brown's Otorhinolaryngology; Cummings Otolaryngology
B. RADIOGRAPHIC FEATURES
- Radiolucent lesion (bone destruction)
- Multilocular appearance - described as:
- "Soap bubble" appearance - large, rounded locules
- "Honeycomb" appearance - small, numerous locules
- Well-demarcated with scalloped margins - margins may be corticated or non-corticated
- Root resorption of adjacent teeth is common
- Some lesions are unilocular (especially unicystic type)
- May be in dentigerous relationship with an unerupted tooth
- Cortical bone expansion and perforation in large lesions
- Scott-Brown's Otorhinolaryngology
C. HISTOPATHOLOGICAL FEATURES
Classic Features (Vickers and Gorlin Criteria):
As described in all standard texts, the defining microscopic features of ameloblastoma are:
- Columnar basal cells (ameloblast-like) at the periphery of tumor islands
- Palisading of basal cells - peripheral cells arranged in a row like a picket fence
- Reverse/Reversed nuclear polarization - nuclei displaced away from the basement membrane (toward the stellate reticulum), opposite to normal ameloblasts
- Hyperchromatism of basal cell nuclei
- Sub-nuclear vacuolization of basal cell cytoplasm (Vickers-Gorlin feature)
- Above the basal layer: loosely aggregated stellate reticulum-like cells - resemble the stellate reticulum of the developing enamel organ
- Cummings Otolaryngology (Vickers and Gorlin criteria)
Histological Subtypes:
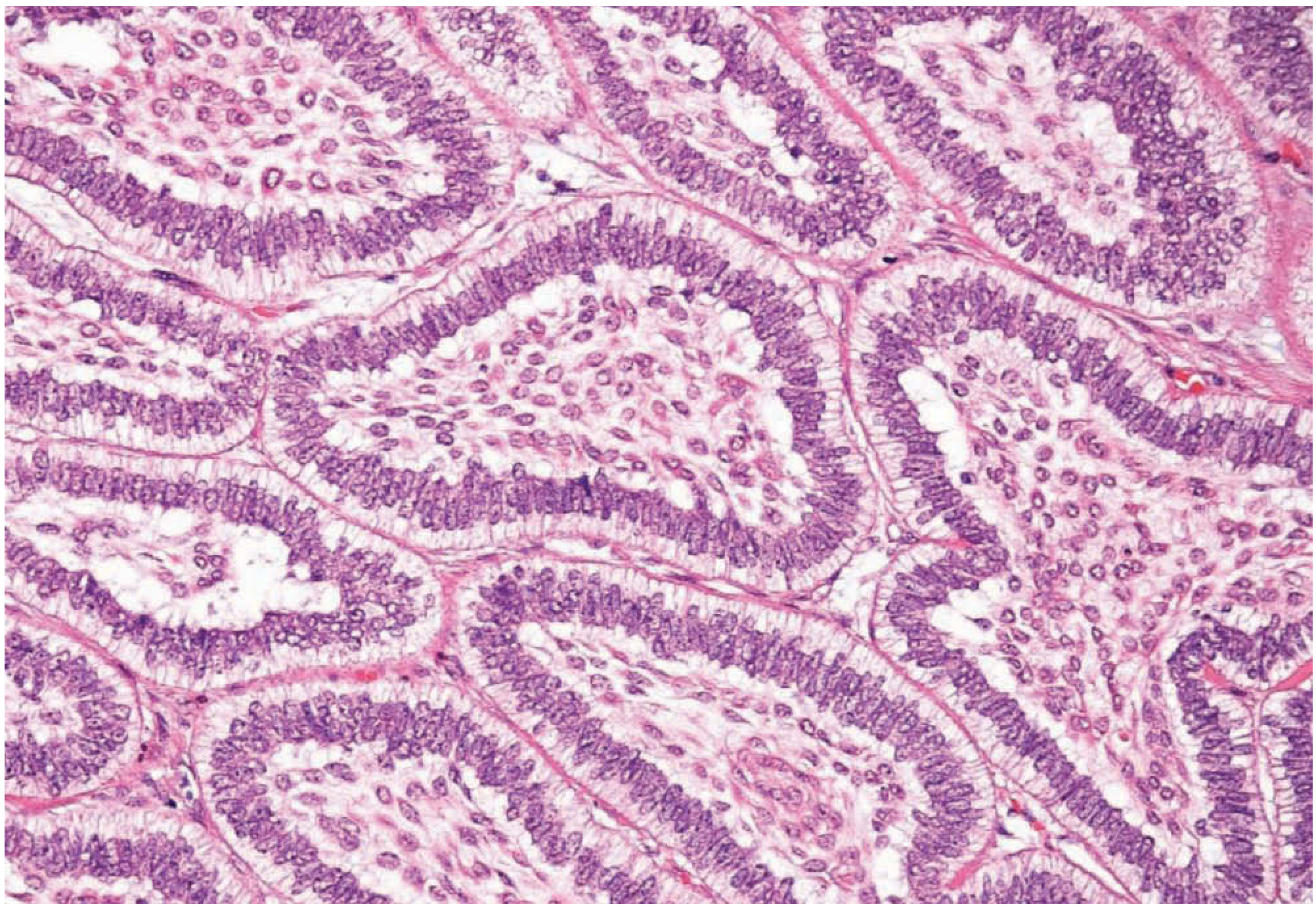
1. Follicular Pattern (most common)
- Discrete islands of odontogenic epithelium in a fibrous stroma
- Each island has peripheral columnar ameloblast-like cells with reversed nuclear polarization
- Central stellate reticulum-like cells
- Cystic spaces commonly develop within the stellate cells (follicular cystic degeneration)
- The follicular pattern most closely mimics the enamel organ
2. Plexiform Pattern
- Odontogenic epithelium arranged in anastomosing cords and strands (interlacing network/plexus)
- Peripheral columnar cells with reversed polarity
- Stellate reticulum less prominent; cysts tend to form within the stroma (not within the epithelial islands)
3. Acanthomatous Pattern
- Central stellate cells undergo squamous metaplasia (acanthomatous change)
- Keratin pearls may be seen centrally within follicles
- Peripheral palisading still present
4. Granular Cell Pattern
- Central stellate cells are replaced by cells with abundant eosinophilic granular cytoplasm (granular cell change)
- Peripheral columnar cells maintain palisading
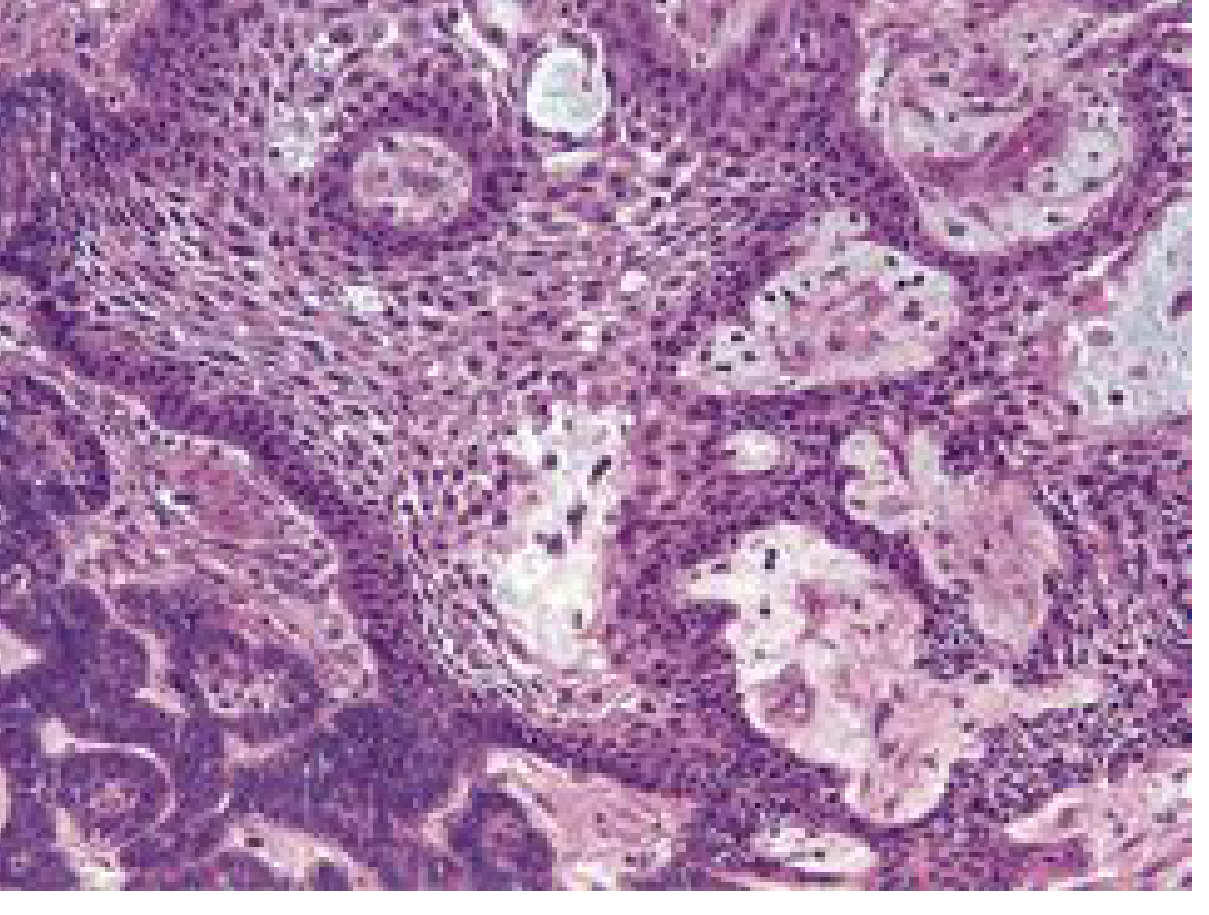
5. Desmoplastic Pattern
- Odontogenic epithelium compressed into small islands within a dense fibrous (desmoplastic) stroma
- Commonly seen in anterior maxilla and mandible
- Radiographically may mimic fibro-osseous lesions
6. Basal Cell Pattern
- Resembles basal cell carcinoma of skin
- Small dark basaloid cells arranged in nests
- Least common variant
Note: Many lesions contain a mix of follicular and plexiform patterns. The histological subtype does NOT affect prognosis or treatment - all are managed the same way.
- Cummings Otolaryngology; Scott-Brown's
2. UNICYSTIC AMELOBLASTOMA (UA)
Clinical Features
- Accounts for 5-15% of all ameloblastomas
- Predominantly in teens and young adults (2nd-3rd decade) - younger than conventional type
- Posterior mandible is the most common site (maxilla:mandible ratio = 1:5)
- Usually presents as a painless swelling
- Often in dentigerous relationship with an unerupted tooth
Radiographic Features
- Well-defined, unilocular radiolucency - resembles a dentigerous cyst
- Root resorption common
- Corticated margins
Histopathology
Vickers and Gorlin criteria applied to the cyst lining:
- Columnar basal cells with palisading
- Reversed nuclear polarization
- Hyperchromatism of basal cell nuclei
- Sub-nuclear vacuolization
- Stellate reticulum-like cells above the basal layer
Subtypes (Ackerman classification):
- Type I - Luminal UA: Ameloblastomatous epithelium confined to the luminal surface only
- Type II - Intraluminal UA: Polypoid/pedunculated masses project into the lumen from the cyst wall
- Type III - Intramural UA (Mural): Ameloblastomatous islands invade the fibrous cyst wall - behaves like conventional ameloblastoma; highest recurrence risk
Treatment
- Types I & II: Conservative enucleation and curettage
- Type III (Mural): Resection with clear margins (managed as conventional ameloblastoma)
- Scott-Brown's Otorhinolaryngology; Cummings Otolaryngology
3. PERIPHERAL (EXTRA-OSSEOUS) AMELOBLASTOMA
- Comprises 2-10% of all ameloblastomas
- Arises in the soft tissue of the gingiva or alveolar mucosa - does NOT invade underlying bone
- Presents as a sessile, painless, firm gingival swelling - may be mistaken for epulis
- Histology: Identical to conventional ameloblastoma but within the connective tissue of the gingiva
- Treatment: Local surgical excision - excellent prognosis, rarely recurs
- Scott-Brown's Otorhinolaryngology
TREATMENT SUMMARY
| Type | Treatment |
|---|---|
| Conventional (SMA) - Mandible | En bloc resection with 1-1.5 cm clear margin beyond radiographic extent |
| Conventional (SMA) - Maxilla | Radical resection (all maxillary lesions - consequences of recurrence near skull base severe; mortality up to 60% with recurrence) |
| Unicystic Types I & II | Enucleation + curettage |
| Unicystic Type III | Resection (as per conventional) |
| Peripheral | Local excision |
| Recurrent / BRAF-mutated | BRAF-targeted therapy (e.g., Vemurafenib) being investigated |
Why simple enucleation fails: Ameloblastoma infiltrates the trabeculae of cancellous bone, and tumor extension frequently goes beyond the radiographic margin. This is the key reason for high recurrence after enucleation alone.
- Cummings Otolaryngology
PROGNOSIS & RECURRENCE
- Conventional ameloblastoma: Good prognosis with adequate resection + regular surveillance
- Unicystic ameloblastoma: 10-20% recurrence even after adequate treatment
- Peripheral ameloblastoma: Rarely recurs - best prognosis of all types
- Malignant transformation (ameloblastic carcinoma): Rare but documented
- KJ Lee's Essential Otolaryngology; Cummings Otolaryngology
EXAM ANSWER FRAMEWORK (RGUHS Format)
For a 10-mark RGUHS long essay:
- Definition (2-3 lines)
- Classification (WHO types + histological subtypes of conventional)
- Clinical features (age, sex, site, presenting features)
- Radiographic features (soap bubble / honeycomb, margins, root resorption)
- Histopathology (Vickers-Gorlin criteria + description of follicular and plexiform types in detail)
- Treatment (resection with 1-1.5 cm margin; unicystic types separately)
- Labeled diagram of follicular ameloblastoma histology (peripheral columnar cells + stellate reticulum + cystic spaces in center)
This is the full textbook answer for Ameloblastoma. Which topic do you want next - OKC/Radicular/Dentigerous Cyst, Pleomorphic Adenoma, OSCC, or Dental Caries Histopathology?
This is a shared conversation. Sign in to Orris to start your own chat.