Give me a short note on Concept of lead time for PSM theory exam for 7 marks including Parks heading
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
I have everything needed. Here is the complete note:
Concept of Lead Time
(Park's Textbook of Preventive and Social Medicine)
Definition
"Lead time" is the advantage gained by screening - it is the period between diagnosis made by early detection (screening) and the diagnosis that would ordinarily have been made by other means (i.e., when symptoms appear).
In simple terms: Lead time = Time of diagnosis by screening - Time of diagnosis by conventional/symptomatic means.
Background - Why Lead Time Matters in Screening
The active search for disease among apparently healthy individuals is a fundamental aspect of prevention, embodied in the concept of screening. Screening is defined as "the search for unrecognized disease or defect by means of rapidly applied tests, examinations or other procedures in apparently healthy individuals."
Detection programmes are most valuable when there is a considerable time lag between disease onset and the usual time of diagnosis. During this interval, there are critical points that determine:
- The severity of the disease
- The success of treatment in reversing the disease process
The Model for Early Detection Programmes (Fig. 1)
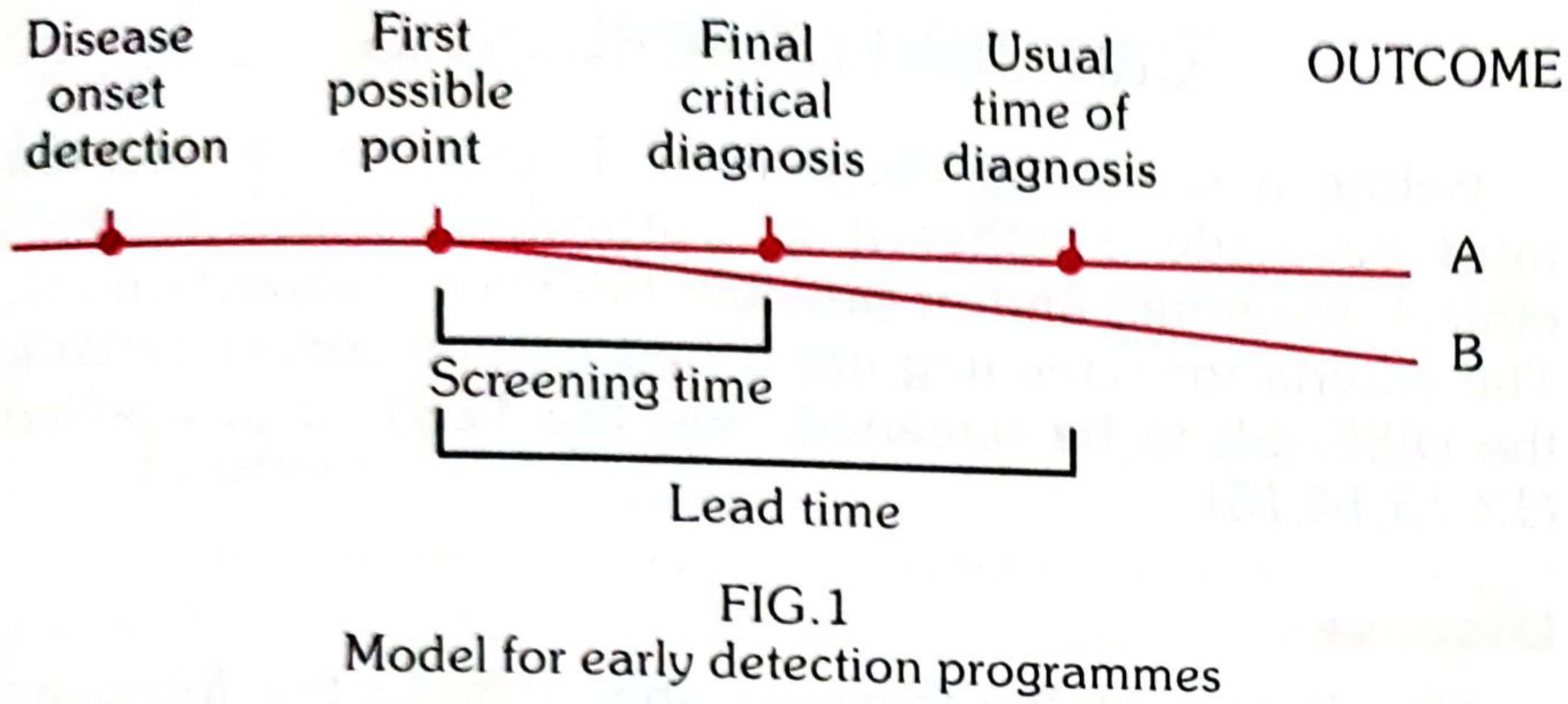
The figure shows the timeline of a disease process with the following key points:
| Point | Description |
|---|---|
| Disease onset/detection | Earliest biological onset of disease |
| First possible point | Earliest point at which the disease can be detected by screening |
| Final critical point (diagnosis) | The last point beyond which treatment will be unsuccessful or permanent damage is irreversible |
| Usual time of diagnosis | When disease is diagnosed based on symptoms (without screening) |
- Line A = Usual outcome without screening
- Line B = Outcome when disease is detected at the earliest possible moment by screening
- Benefit of screening = B - A (the difference in outcomes)
The screening time spans from the first possible detection point to the final critical diagnosis point.
The lead time spans from the first possible detection point to the usual time of (symptomatic) diagnosis.
Key Principles
-
Screening is worthwhile only if detection precedes the final critical point - there is little value in detecting a disease if the critical window for effective treatment has already passed.
-
Screening programmes should concentrate on diseases where the time lag between onset and the final critical point is sufficiently long to make population-wide screening feasible and beneficial.
-
There is nothing to be gained by screening for diseases whose onset is quite obvious or symptomatic from the start.
-
The benefits of any detection programme must be viewed against its complexities and costs. Lead time quantifies the potential benefit in terms of improved outcomes.
Lead-Time Bias
Lead-time bias is an important concept in evaluating screening programmes:
- Screening may appear to increase survival time after diagnosis merely because disease is diagnosed earlier, not because the disease course has actually been altered.
- For example: if a cancer is detected 2 years earlier by screening but the patient dies at the same time as they would have without screening, the apparent "survival" is longer but no real benefit has occurred.
- This bias must be accounted for when assessing screening programme outcomes - improvements in stage distribution and survival from diagnosis can be misleading without correcting for lead time.
Summary (Exam Point)
Lead time = the period between detection of disease by screening and detection by usual clinical means (symptoms). It represents the head start given by screening. A longer lead time means more opportunity for effective intervention - but the benefit is real only if that time is used to treat the disease before its final critical point is reached.
- Park's Textbook of Preventive and Social Medicine, p. 155
Give me a short note on Sreening test diagnostic criteria for PSM theory exam for 7 marks including Parks heading
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the content needed from Park's textbook. Here is the complete 7-mark note:
Criteria for Screening / Screening Test - Diagnostic Criteria
(Park's Textbook of Preventive and Social Medicine)
Introduction
Before a screening programme is initiated, a decision must be made whether it is worthwhile, which requires ethical, scientific, and financial justification. The criteria for screening are based on two broad considerations:
- The DISEASE to be screened
- The TEST to be applied
I. Criteria Related to the DISEASE
The disease to be screened should fulfil the following criteria:
- The condition should be an important health problem (prevalence should generally be high)
- There should be a recognizable latent or early asymptomatic stage
- The natural history of the condition, including progression from latent to declared disease, should be adequately understood
- There should be a test that can detect the disease prior to the onset of signs and symptoms
- Facilities should be available for confirmation of the diagnosis
- There should be an effective treatment available
- There should be an agreed-upon policy concerning whom to treat (e.g., borderline diabetes, lower ranges of blood pressure)
- There should be good evidence that early detection and treatment reduces morbidity and mortality
- The expected benefits (lives saved) should exceed the risks and costs
II. Criteria Related to the SCREENING TEST
The test must satisfy criteria of acceptability, repeatability and validity, besides yield, simplicity, safety, rapidity, ease of administration and cost. (Note: a test meeting one criterion may compromise another - the choice is often a compromise.)
1. Acceptability
- Since high cooperation is needed, the test must be acceptable to the target population
- Tests that are painful, discomforting or embarrassing (e.g., rectal or vaginal examinations) are less acceptable for mass campaigns
2. Repeatability (Reliability / Precision / Reproducibility)
The test must give consistent results when repeated on the same individual under the same conditions. Repeatability depends on three factors:
A. Observer Variation
- Intra-observer variation - variation between repeated observations by the same observer on the same subject at the same time
- Inter-observer variation - variation between different observers examining the same subject/material
B. Biological (Subject) Variation - natural fluctuations within the subject itself
C. Technical/Method Errors - errors related to laboratory or measurement methods
3. Validity (Accuracy)
Validity is the ability of a test to measure what it is intended to measure. It has two components:
a. Sensitivity
The ability of a test to identify correctly all those who have the disease ("true-positives")
- Formula: Sensitivity = a / (a + c) × 100
- A 90% sensitivity means 90% of diseased persons will give a true-positive result; 10% will give false-negatives
- A highly sensitive test has few false negatives
b. Specificity
The ability of a test to identify correctly those who do NOT have the disease ("true-negatives")
- Formula: Specificity = d / (b + d) × 100
- A 90% specificity means 90% of non-diseased persons will give true-negative results; 10% will be falsely classified as diseased
- A highly specific test has few false positives
Key relationship: Sensitivity and specificity are inversely related - increasing one reduces the other. An ideal test would be 100% sensitive and 100% specific, but this rarely occurs in practice.
The 2×2 Table
| Diseased | Not Diseased | Total | |
|---|---|---|---|
| Test Positive | a (True +ve) | b (False +ve) | a+b |
| Test Negative | c (False -ve) | d (True -ve) | c+d |
| Total | a+c | b+d | a+b+c+d |
4. Predictive Value
Reflects the diagnostic power of the test. It depends on sensitivity, specificity, and disease prevalence.
- Predictive value of a positive test = a / (a+b) × 100
- Probability that a person with a positive test actually has the disease
- Increases as disease prevalence increases; falls as prevalence declines
- Predictive value of a negative test = d / (c+d) × 100
5. False Negatives and False Positives
| Meaning | Consequence | |
|---|---|---|
| False-Negative | Diseased person told they are disease-free | "False reassurance" - patient may ignore symptoms, delay treatment |
| False-Positive | Healthy person told they have disease | Subjects them to further tests, anxiety, expense; burdens diagnostic facilities and brings discredit to screening programmes |
6. Yield
"Yield" is the amount of previously unrecognized disease diagnosed as a result of screening.
Yield depends on: sensitivity, specificity, disease prevalence, and participation rate. Yield can be increased by targeting high-risk populations (e.g., limiting diabetes screening to persons over 40 years).
7. Combination of Tests
Two or more tests can be combined to enhance sensitivity or specificity. Example: in syphilis screening, all are first tested by RPR (high sensitivity) followed by FTA-ABS (high specificity) for RPR-positives - ensuring only true positives are confirmed.
Summary
| Component | Key Criterion |
|---|---|
| Disease | Important, latent stage exists, effective treatment available |
| Acceptability | Acceptable to the population |
| Repeatability | Consistent results (intra/inter-observer, biological, technical variation) |
| Sensitivity | Detects true positives; low = many false negatives |
| Specificity | Detects true negatives; low = many false positives |
| Predictive Value | Depends on prevalence; falls as prevalence falls |
| Yield | Maximize by targeting high-risk groups |
- Park's Textbook of Preventive and Social Medicine, pp. 156-159
Give me a short note on Evaluation of screening test for PSM theory exam for 7 marks including Parks heading
Finding Sources
Reading File
Reading File
Reading File
I now have all the content needed. Here is the complete exam-ready note:
Evaluation of a Screening Test
(Park's Textbook of Preventive and Social Medicine)
Introduction
Evaluation of a screening test means determining how well a test separates those who have the disease from those who do not. The following measures are used to evaluate a screening test.
The 2×2 Table (Foundation of Evaluation)
| Diseased | Not Diseased | Total | |
|---|---|---|---|
| Test Positive | a (True-positive) | b (False-positive) | a+b |
| Test Negative | c (False-negative) | d (True-negative) | c+d |
| Total | a+c | b+d | a+b+c+d |
- a = True positives (diseased + test positive)
- b = False positives (not diseased + test positive)
- c = False negatives (diseased + test negative)
- d = True negatives (not diseased + test negative)
Measures of Evaluation
1. Sensitivity
The ability of a test to correctly identify all those who have the disease (true-positives).
Formula: Sensitivity = a / (a + c) × 100
- A 90% sensitivity means 90% of diseased persons will give a true-positive result; the remaining 10% give a false-negative result
- A highly sensitive test has few false negatives
- Sensitivity is low → large number of false negatives
2. Specificity
The ability of a test to correctly identify those who do NOT have the disease (true-negatives).
Formula: Specificity = d / (b + d) × 100
- A 90% specificity means 90% of non-diseased persons will give a true-negative result; 10% will be falsely classified as diseased
- A highly specific test has few false positives
- Specificity is low → large number of false positives
Key principle: Sensitivity and specificity are inversely related - increasing one reduces the other. An ideal test is 100% sensitive AND 100% specific; in practice, this rarely occurs.
3. Predictive Accuracy (Predictive Value)
Reflects the diagnostic power of the test. Depends on sensitivity, specificity, AND disease prevalence.
(a) Predictive value of a positive test = a / (a + b) × 100
- Probability that a person with a positive test actually has the disease
- Increases as disease prevalence increases; falls as prevalence declines
- Example: Gram-stained cervical smear for gonorrhoea - predictive value was 21%, 47%, and 63% at prevalences of 5%, 15%, and 25% respectively
(b) Predictive value of a negative test = d / (c + d) × 100
- Probability that a person with a negative test truly does not have the disease
4. False Negatives and False Positives
| Meaning | Consequence | |
|---|---|---|
| False-Negative | Diseased person told they are normal | "False reassurance" - patient may ignore symptoms, delay treatment; potentially detrimental for serious diseases |
| False-Positive | Healthy person told they have disease | Subjected to further diagnostic tests, anxiety, discomfort and expense; burdens diagnostic facilities; brings discredit to screening programmes |
- Epidemiologist thinks in terms of sensitivity and specificity
- Clinician thinks in terms of false negatives and false positives
5. Percentage of False Negatives and Positives
- % False negatives = c / (a + c) × 100
- % False positives = b / (b + d) × 100
Cut-off Point and Decision Making
When a screening test measures a quantitative variable (e.g., blood glucose, blood pressure), the distributions of diseased and non-diseased persons overlap, creating a zone of false positives and false negatives. A cut-off point must be chosen.
Factors determining the cut-off point:
- Disease prevalence - When prevalence is high, set the cut-off lower to increase sensitivity
- Nature of the disease:
- For lethal diseases (e.g., cervical cancer, breast cancer) where early detection dramatically improves prognosis → higher sensitivity is preferred, even at expense of specificity (false positives are tolerable, false negatives are not)
- For prevalent diseases where treatment does not markedly alter outcome (e.g., diabetes) → higher specificity is needed (false positives must be limited to avoid overburdening the health system)
Example - Blood glucose cut-off for diabetes (2-hr post-prandial):
| Cut-off (mg/100 ml) | Sensitivity | Specificity |
|---|---|---|
| 80 | 100% | 1.2% |
| 130 | 81.4% | 82.4% |
| 180 | 50% | 99.8% |
| 200 | 37.1% | 100% |
This clearly shows the inverse relationship between sensitivity and specificity.
6. Yield
"Yield" = the amount of previously unrecognized disease diagnosed as a result of screening effort.
Depends on: sensitivity, specificity, disease prevalence, and participation rate.
Yield is increased by targeting high-risk populations (e.g., diabetes screening in persons over 40 years).
7. Combination of Tests
Two or more tests used together can enhance sensitivity or specificity:
- Sequential/serial testing: All screened by a high-sensitivity test first (e.g., RPR for syphilis), then positives retested by a high-specificity test (e.g., FTA-ABS) → final positives are true cases
- Parallel testing: Multiple tests done simultaneously; improves sensitivity
Summary Table
| Measure | Formula | What It Tells You |
|---|---|---|
| Sensitivity | a/(a+c) ×100 | How well test finds true cases |
| Specificity | d/(b+d) ×100 | How well test excludes non-cases |
| PV of positive test | a/(a+b) ×100 | Probability positive = truly diseased |
| PV of negative test | d/(c+d) ×100 | Probability negative = truly normal |
| % False negative | c/(a+c) ×100 | Missed cases |
| % False positive | b/(b+d) ×100 | Over-diagnosis |
- Park's Textbook of Preventive and Social Medicine, pp. 157-161
This is a shared conversation. Sign in to Orris to start your own chat.