Tell me about TKR surgery
Reading File
Finding Sources
Searching PubMed
"total knee arthroplasty"[MeSH Terms] AND outcomes
Searching the Web
total knee replacement surgery overview indications procedure complications 2025
Finding Sources
Searching PubMed
"knee arthroplasty"[MeSH Terms] AND "complications"[MeSH Terms]
Reading Web Page
https://www.orthoinfo.org/treatment/total-knee-replacement
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a thorough overview of Total Knee Replacement (TKR) surgery, drawing from Bailey & Love's Short Practice of Surgery (28th Ed), Campbell's Operative Orthopaedics (15th Ed 2026), and authoritative clinical sources.
Total Knee Replacement (TKR) Surgery
Also called Total Knee Arthroplasty (TKA), TKR is one of the most successful surgical interventions in modern medicine. It is a resurfacing procedure in which the diseased articular surfaces of the knee are replaced with metal and plastic implants. Over 700,000 are performed annually in the US alone.
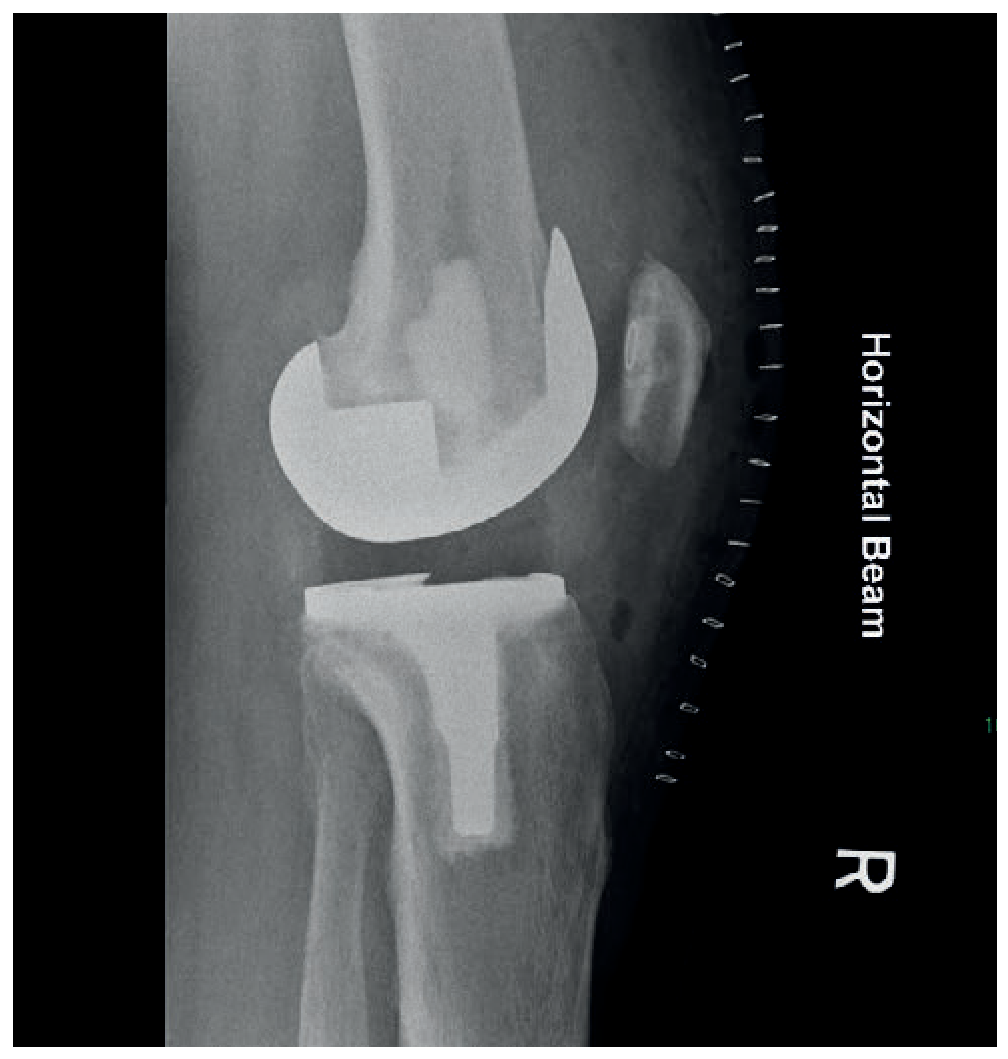
Lateral radiograph of a right total knee replacement - the femoral metal component and tibial baseplate with polyethylene insert are clearly visible:
Anatomy of the Knee Relevant to TKR
The knee has three compartments:
- Medial tibiofemoral
- Lateral tibiofemoral
- Patellofemoral
In 20-50% of cases, osteoarthritis (OA) affects only one compartment, making patients candidates for a unicompartmental knee replacement (UKR). When all three compartments are involved, a TKR is indicated.
Indications
The primary indication is significant, disabling pain from severe arthritis that is refractory to non-operative treatments. Specific conditions include:
- Osteoarthritis (most common) - end-stage tricompartmental disease
- Rheumatoid arthritis and other inflammatory arthropathies
- Post-traumatic arthritis
- Severe patellofemoral arthritis (when arthroplasty is superior to patellectomy)
- Deformity - significant flexion contracture, or varus/valgus laxity can itself become the principal indication even with moderate arthritis
Night pain is a particularly significant symptom justifying surgery. Significant reduction in quality of life is also factored in.
Contraindications
Absolute contraindications include:
- Active knee joint infection
- Absent or non-functional extensor mechanism
- Severe vascular disease
- Neuropathic joint (Charcot arthropathy) - relative
Relative contraindications include morbid obesity, medical comorbidities that substantially increase operative risk, and young age (concern for implant longevity).
Surgical Procedure
Anesthesia
TKR can be performed under regional (spinal/epidural) or general anesthesia. Cardiovascular outcomes, cognitive function, and mortality have not been shown to differ significantly between the two approaches.
The Four Operative Steps
- Prepare the bone - The surgeon removes damaged cartilage from the ends of the femur and tibia, along with a small amount of underlying bone.
- Position the metal implants - Metal components resurface the femoral condyles and tibial plateau. These may be cemented (using PMMA - polymethylmethacrylate, the current gold standard) or press-fit (uncemented, with bioactive surfaces like hydroxyapatite - showing promising midterm results).
- Resurface the patella - The undersurface of the kneecap is cut and resurfaced with a plastic button. Some surgeons omit this step depending on the case.
- Insert the spacer - A medical-grade polyethylene (plastic) spacer is inserted between the metal components to create a smooth gliding surface.
Implant Design Choices
| Design | Key Feature |
|---|---|
| Cruciate-retaining (CR) | Preserves the posterior cruciate ligament |
| Posterior-stabilized (PS) / cruciate-sacrificing | PCL is sacrificed; tibial post substitutes its function |
| Rotating platform | Mobile-bearing tibial insert - reduces wear |
| Constrained / hinged | Used for severe instability or deformity; higher loosening risk |
Constraint level is a key trade-off: more constrained implants transmit greater forces to the cement-bone interface, increasing the risk of aseptic loosening.
Alignment Goals (Surgical Aims)
- Correct deformity caused by arthritis
- Align the leg to the mechanical axis (or slightly undercorrected)
- Joint line perpendicular to the mechanical axis
- Balanced collateral ligaments
- Normal patellofemoral tracking
Modern philosophies include kinematic alignment (matching the patient's natural anatomy) using computer navigation or robotic-assisted surgery, though this requires additional technology.
Bearing Surfaces
To reduce wear, modern implants use:
- Cross-linked polyethylene
- Vitamin E-enriched polyethylene
- Ceramicised surface coatings
Recovery
- Hospital stay: 2-4 days for most patients; some are treated as day cases
- Early weight-bearing and mobilization are now standard
- Full recovery typically takes 1-3 months
- Activities permitted: walking, swimming, golf, cycling, light hiking, ballroom dancing
- Activities to avoid for life: running, jogging, jumping, high-impact sports (accelerate wear and risk loosening)
Complications
Intraoperative
- Implant malposition/malalignment (leading to instability, stiffness, or pain)
- Nerve or vessel injury (including tourniquet damage)
- Fracture
- Patellar tendon avulsion
- Fat embolism
Postoperative
| Complication | Notes |
|---|---|
| Infection | <2% of cases; most serious complication |
| DVT / Pulmonary embolism | Standard prophylaxis required |
| Pain / stiffness | A small number have persistent pain |
| Instability | Often from malalignment or soft-tissue imbalance |
| Osteolysis | Polyethylene wear particles trigger macrophage reaction |
| Component loosening | Aseptic loosening is the main late failure mode |
| Neurovascular injury | Rare |
Outcomes & Survivorship
TKR has excellent long-term survivorship:
- >95% implant survival at 10-15 years
- 82% lasting over 20 years
- Revision rate <5% at 15 years
The large majority of patients experience significant pain relief and improved mobility. Patient satisfaction, however, is generally somewhat lower than hip replacement - roughly 15-20% of TKR patients report dissatisfaction, often related to residual stiffness or unmet pain expectations.
Revision TKR
Early revisions (within the first few years) are most often due to infection and non-infective causes like instability and malalignment. Beyond 10 years, the dominant cause is aseptic loosening from polyethylene wear and polyethylene-induced osteolysis. Revision surgery is technically more demanding, requires more complex (and expensive) implants, and carries a higher complication rate than primary TKR. A two-stage revision is used when infection is confirmed.
UKR vs TKR - Key Comparison
| Feature | UKR | TKR |
|---|---|---|
| Disease extent | Single compartment | All three compartments |
| Infection rate | Lower | Higher |
| Recovery | Faster | Slower |
| Kinematics | More preserved | Altered |
| 10-year revision rate | 6-12% (registry data) | 2-6% |
| Eligibility | Intact ligaments, <15° fixed deformity | Broader |
Source: Bailey and Love's Short Practice of Surgery, 28th Ed; Campbell's Operative Orthopaedics 15th Ed 2026; AAOS OrthoInfo
This is a shared conversation. Sign in to Orris to start your own chat.