Reflex arc physiology 8 marks refer mbbs textbook and answer pls
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive content from two authoritative MBBS physiology textbooks (Ganong's Review of Medical Physiology and Costanzo Physiology) along with excellent diagrams. Here is the complete 8-mark answer:
Reflex Arc - Physiology (8 Marks)
Definition of a Reflex
A reflex is a stereotyped, involuntary motor response to a specific sensory stimulus. It is rapid, predictable, and does not require conscious thought. Reflex activity is adaptable and can be modified by experience and descending inputs from higher brain regions.
Ganong's Review of Medical Physiology, 26th Edition
The Reflex Arc
The reflex arc is the basic unit of integrated reflex activity - the neuronal circuit that directs the motor response. It consists of five essential components:
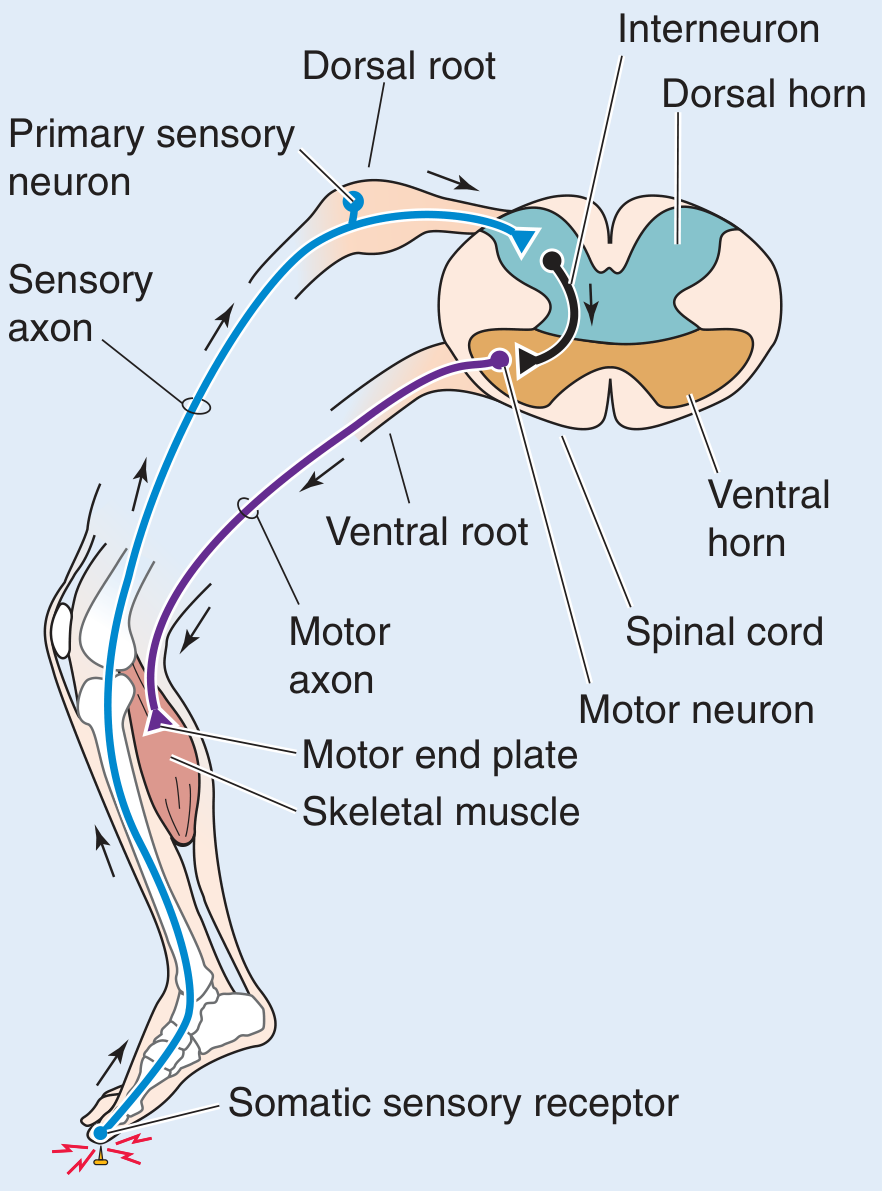
Five Components of the Reflex Arc
1. Receptor (Sense Organ)
- The site where a stimulus is detected and transduced into a nerve signal
- Produces a graded receptor (generator) potential proportional to the strength of the stimulus
- Examples: muscle spindles (detect stretch), Golgi tendon organs (detect tension), nociceptors (detect pain), Pacinian corpuscles (detect pressure)
2. Afferent (Sensory) Neuron
- Carries impulses from the receptor to the CNS
- Cell bodies lie in the dorsal root ganglion (for spinal reflexes) or in homologous cranial nerve ganglia
- Axons enter the spinal cord via the dorsal root
- Generates all-or-none action potentials; the number of action potentials is proportional to the size of the receptor potential
3. Nerve Centre (Integration Centre / Synapse in CNS)
- Located in the spinal cord (dorsal horn and anterior horn)
- Processing occurs here; responses are graded as EPSPs and IPSPs at synaptic junctions
- The number of synapses determines reflex complexity:
- Monosynaptic reflex - one synapse (e.g., stretch reflex)
- Polysynaptic reflex - two or more synapses (e.g., flexor-withdrawal reflex)
- Interneurons may be interposed and can influence other motor neurons (reciprocal inhibition, crossed extension)
4. Efferent (Motor) Neuron
- Carries impulses from the CNS to the effector
- Exits via the ventral root (for spinal reflexes)
- The alpha (α) motor neurons that supply extrafusal skeletal muscle fibers are the efferent side of most somatic reflex arcs
- Called the "final common pathway" - all neural influences on muscular contraction funnel through them; up to 10,000 synaptic knobs converge on a single motor neuron
5. Effector Organ
- The organ that carries out the response
- Usually skeletal muscle (somatic reflexes) or smooth muscle/gland (visceral/autonomic reflexes)
- At the neuromuscular junction, the efferent neuron produces a graded endplate potential, which then triggers an all-or-none action potential in the muscle fiber, producing contraction
Ganong's Review of Medical Physiology, 26th Edition, Chapter 12
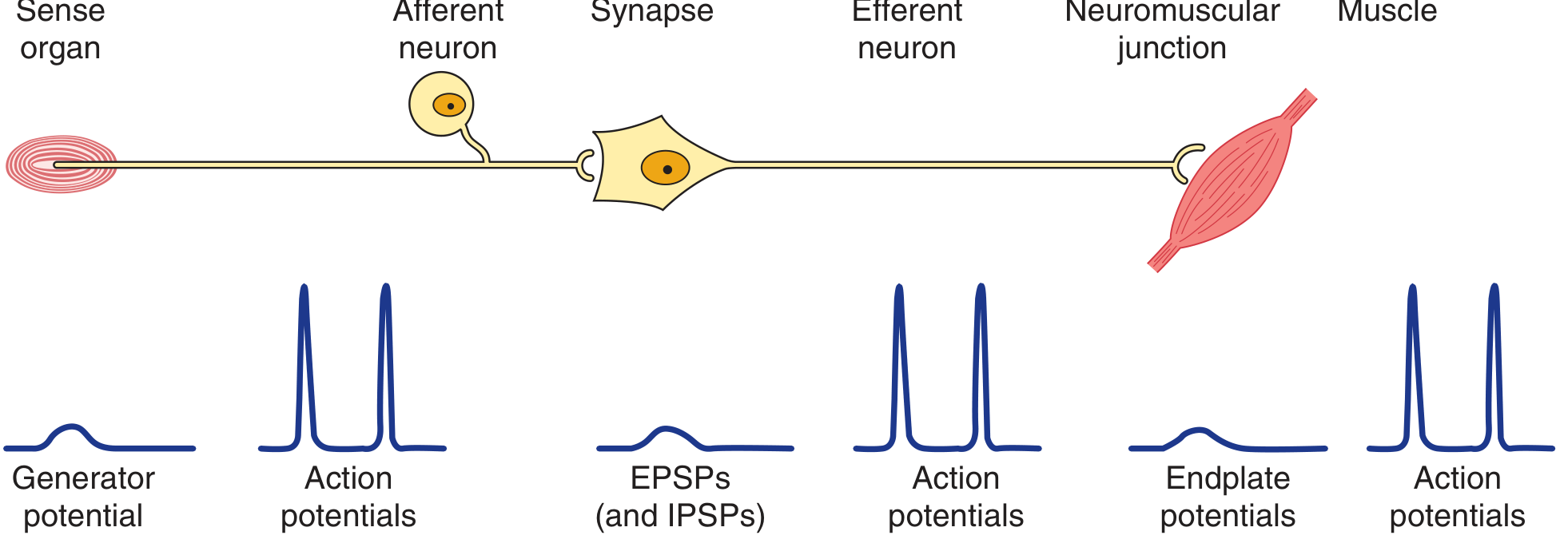
Electrical Events Along the Reflex Arc
| Component | Type of Potential |
|---|---|
| Receptor | Graded generator potential |
| Afferent nerve | All-or-none action potentials |
| CNS synapse | Graded EPSPs / IPSPs |
| Efferent nerve | All-or-none action potentials |
| Neuromuscular junction | Graded endplate potential |
| Muscle | All-or-none action potentials → contraction |
Classification of Spinal Cord Reflexes
| Reflex | Synapses | Stimulus | Afferent Fiber | Response |
|---|---|---|---|---|
| Stretch (myotatic) reflex - e.g., knee jerk | One (monosynaptic) | Muscle stretch | Group Ia | Contraction of stretched muscle |
| Golgi tendon (inverse stretch) reflex | Two | Muscle contraction/tension | Group Ib | Relaxation of muscle (autogenic inhibition) |
| Flexor-withdrawal reflex | Many (polysynaptic) | Pain/temperature | Groups II, III, IV | Ipsilateral flexion + contralateral extension |
Costanzo Physiology, 7th Edition, Table 3.5
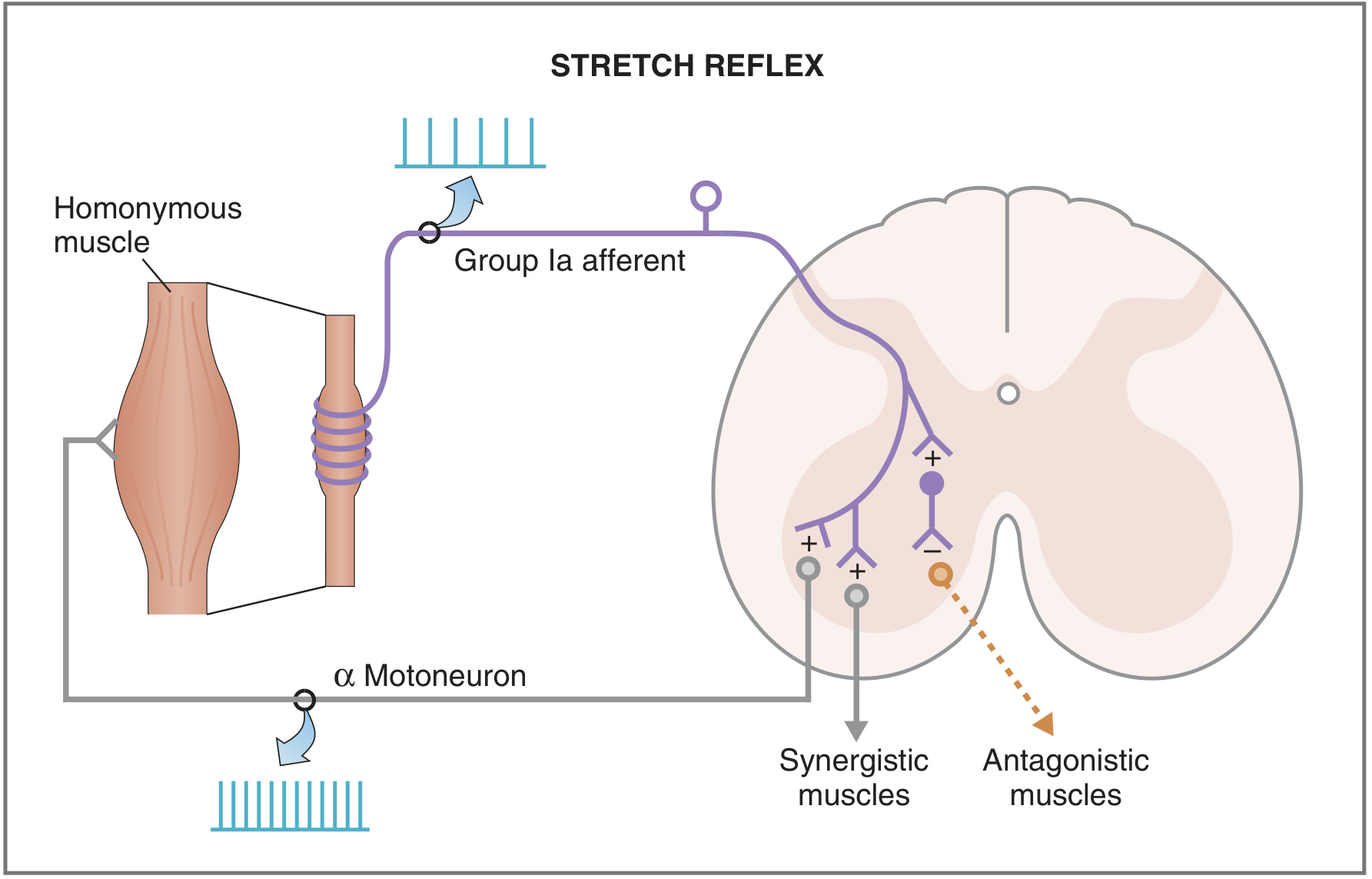
Stretch Reflex (Monosynaptic) - Detailed Example
The knee-jerk reflex is the classic example:
- Tapping the patellar tendon stretches the quadriceps muscle
- Group Ia afferent fibers in the muscle spindle are activated; their firing rate increases
- These Ia afferents enter the spinal cord and synapse directly on α motoneurons (monosynaptic)
- α Motoneurons are activated and cause contraction of the quadriceps (homonymous muscle)
- Simultaneously, inhibitory interneurons cause reciprocal inhibition of the antagonist (hamstrings)
- γ Motoneurons are co-activated with α motoneurons, keeping the muscle spindle sensitive to length changes throughout the contraction
- The neurotransmitter at the central synapse is glutamate
Properties of Reflexes
- Stereotyped - a particular stimulus always produces a particular, predictable response
- Involuntary - do not require conscious initiation
- Rapid - due to short neural pathways
- Adaptable - can be modified by descending inputs from higher centers and by learning/experience
- Ipsilateral or contralateral - most somatic reflexes act on the same side, but the crossed-extension reflex acts on the opposite limb
Clinical Significance
- Absent reflexes (hyporeflexia/areflexia) indicate damage anywhere in the reflex arc - the receptor, afferent nerve, or motor neuron. Most common cause is peripheral neuropathy (e.g., diabetes, alcoholism)
- Exaggerated reflexes (hyperreflexia) suggest interruption of descending corticospinal pathways that normally suppress reflex arc activity (upper motor neuron lesion)
- Deep tendon reflexes (DTRs) are graded 0-5+:
- 0 = absent; 2+ = normal; 4-5+ = hyperactive with clonus
- Spinal cord levels tested: biceps (C5, C6), triceps (C7), patellar (L4), Achilles (S1)
Ganong's Review of Medical Physiology, 26th Ed, Clinical Box 12-1
Sources:
- Ganong's Review of Medical Physiology, 26th Edition - Chapter 12 (Reflex Arc, Monosynaptic Reflexes)
- Costanzo Physiology, 7th Edition - Chapter 3 (Spinal Cord Reflexes, Table 3.5)
- Medical Physiology (Boron & Boulpaep) - Chapter 10 (Spinal Reflex Arc diagram)
This is a shared conversation. Sign in to Orris to start your own chat.