Atherosclerosis
Reading File
Finding Sources
Searching PubMed
"atherosclerosis"[MeSH Terms] AND "pathogenesis"[MeSH Terms]
Searching the Web
atherosclerosis pathophysiology mechanisms 2025 review
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have rich, comprehensive content from Robbins Pathologic Basis of Disease, Robbins Basic Pathology, and Guyton & Hall. Let me compile the full answer.
Atherosclerosis
Atherosclerosis is a chronic inflammatory disease of large and medium-sized arteries characterized by the formation of intimal lesions called atheromas (atherosclerotic plaques). It is the single leading cause of morbidity and mortality in the Western world, responsible for roughly half of all deaths, primarily through coronary artery disease, cerebral infarction, and peripheral vascular disease.
Definition and Core Concept
Atherosclerosis is best understood as the vascular response to endothelial injury. It involves the accumulation of lipids, inflammatory cells, smooth muscle cells (SMCs), and extracellular matrix within the intima of arterial walls, forming raised plaques that narrow lumens and may rupture catastrophically.
The term arteriosclerosis is broader - it refers to thickening and stiffening of blood vessels of all sizes; atherosclerosis is the most clinically important subtype.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 465
Epidemiology
-
Atherosclerosis-related ischemic heart disease is near-universal in high-resource nations, though risk reduction and improved therapies have reduced associated mortality over recent decades.
-
Adoption of Western diet/lifestyle has increased prevalence in lower-resource nations - death rates from coronary artery disease in Africa, India, and Southeast Asia now exceed those in the United States.
-
Eastern European countries have rates 3-5x higher than the US, and 7-12x higher than Japan.
-
Myocardial infarction accounts for nearly a quarter of all deaths in the United States.
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 465-466
Risk Factors
Non-modifiable (Constitutional)
| Factor | Notes |
|---|---|
| Genetics | Family history is the most important independent risk factor. Familial hypercholesterolemia (LDL receptor mutations) is a strong Mendelian association. Most familial predisposition is polygenic. |
| Age | Between ages 40-60, MI incidence increases fivefold. Aging is associated with clonal hematopoiesis of indeterminate potential (CHIP) - outgrowth of hematopoietic stem cells with mutations that confer a pro-inflammatory monocyte phenotype, exacerbating atherosclerosis. |
| Sex | Premenopausal females are relatively protected. After menopause, risk rises to equal or exceed men. Note: postmenopausal estrogen therapy does NOT provide benefit and may increase risk. |
Modifiable (Major)
| Factor | Mechanism |
|---|---|
| Hyperlipidemia / Hypercholesterolemia | Even alone, sufficient to initiate lesion development. LDL ("bad") is the key culprit. HDL ("good") mobilizes cholesterol to the liver - higher HDL correlates with reduced risk. Lp(a) (LDL + apo A) independently increases coronary and cerebrovascular risk. |
| Hypertension | Raises hemodynamic stress on endothelium; doubles risk even at borderline levels. |
| Cigarette smoking | Strongly associated, especially in men; cessation reduces risk. |
| Diabetes mellitus | Causes hypercholesterolemia and accelerated atherosclerosis; substantially increases risk of MI, stroke, and peripheral vascular disease. |
| Inflammation / CRP | C-reactive protein (CRP) adds independent prognostic information at all levels of traditional Framingham risk. Elevated CRP reflects systemic inflammation. |
| Hemostatic factors | Elevated plasminogen activator inhibitor 1 (PAI-1) predicts MI and stroke; platelet-derived factors and thrombin contribute locally. |
Additional Factors
-
Physical inactivity, obesity, hypertriglyceridemia, type A (hostile/competitive) personality, and diet all contribute.
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 466-468
Pathogenesis - The "Response to Injury" Hypothesis
The contemporary model integrates all risk factors into a unified framework: atherosclerosis is a chronic inflammatory and healing response of the arterial wall to endothelial injury.
Step-by-Step Sequence
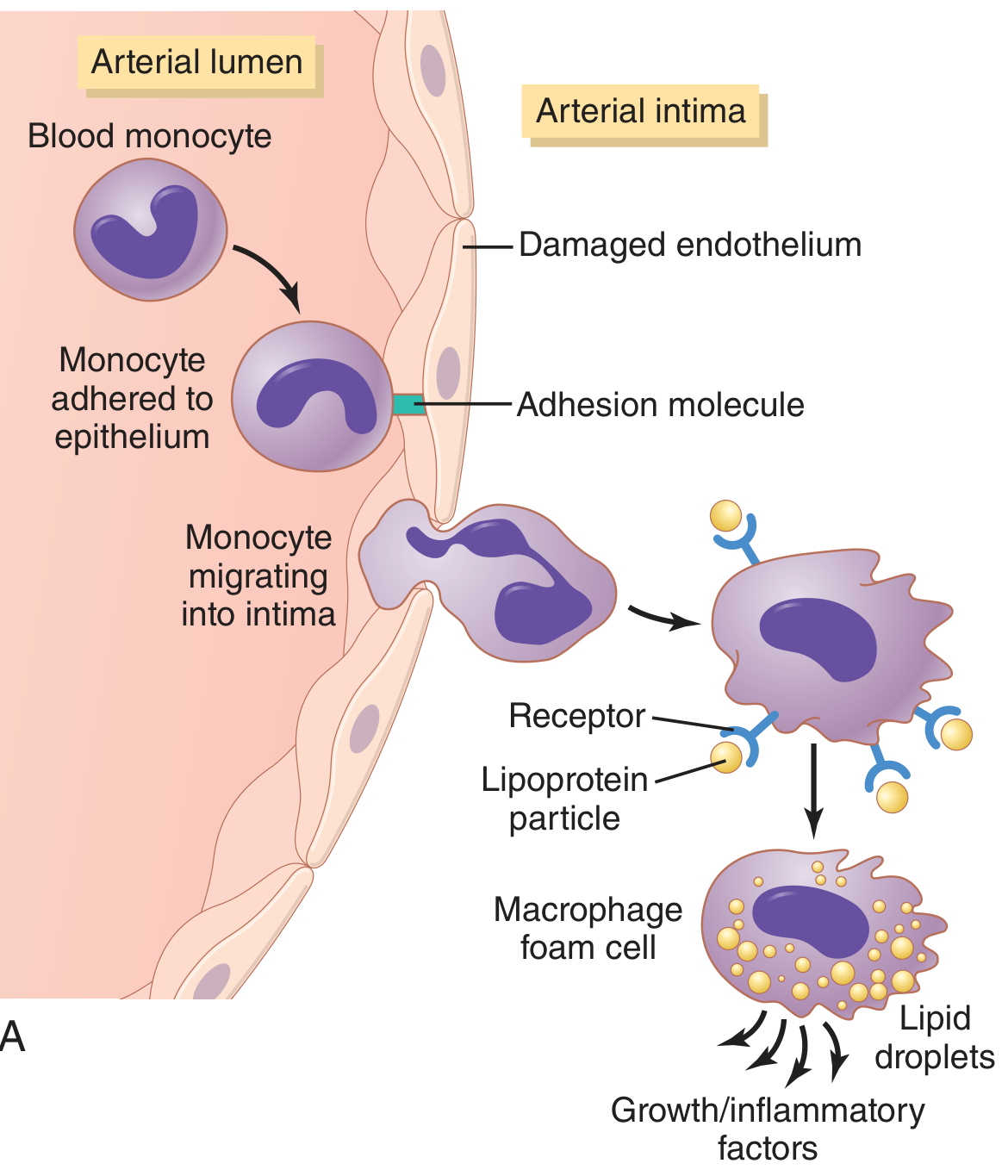
Fig. Development of atherosclerotic plaque - monocyte adhesion to damaged endothelium, migration into intima, and macrophage foam cell formation (Guyton & Hall)
1. Endothelial Injury and Dysfunction
- Triggers include: hemodynamic stress (turbulent flow at arterial branch points), hypercholesterolemia, hypertension, cigarette smoke toxins, inflammatory cytokines, immune complexes.
- Injured endothelium shows: increased permeability, upregulation of adhesion molecules (VCAM-1, ICAM-1, E-selectin), impaired nitric oxide (NO) production, and a pro-thrombotic/pro-inflammatory state.
2. Lipoprotein Accumulation
- LDL and oxidized LDL (oxLDL) accumulate in the subintimal space.
- OxLDL is particularly harmful: it stimulates further endothelial activation, is toxic to SMCs, and is phagocytosed by macrophages via scavenger receptors (bypassing normal LDL receptor feedback).
3. Monocyte Recruitment and Foam Cell Formation
- Circulating monocytes adhere to activated endothelium, migrate into the intima, and differentiate into macrophages.
- Macrophages ingest oxLDL via scavenger receptors, becoming foam cells - the hallmark of early atherosclerosis.
- Foam cells aggregate to form fatty streaks (the earliest grossly visible lesion), visible as yellow intimal streaks.
4. Smooth Muscle Cell (SMC) Recruitment and Proliferation
- Growth factors (PDGF, FGF) and cytokines from platelets, macrophages, and ECs drive SMC migration from media to intima.
- Intimal SMCs proliferate and synthesize extracellular matrix (collagen, proteoglycans), forming the fibrous cap of the mature plaque.
5. T Lymphocyte Recruitment
- T cells are recruited and, upon recognizing antigens (e.g., oxLDL-protein complexes), secrete cytokines (IFN-γ) that further activate macrophages and inhibit SMC collagen synthesis - destabilizing the plaque.
6. Lipid Accumulation and Necrotic Core Formation
-
Foam cells die and release their lipid content, forming the soft, grumous lipid (necrotic) core.
-
Extracellular cholesterol crystals accumulate; calcification may follow.
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 468-470
Morphology of the Atherosclerotic Plaque
Gross Appearance
- Fatty streak: earliest lesion - flat yellow intimal streak composed of lipid-laden foam cells. Present even in aortas of children.
- Fibrolipid (atheromatous) plaque: raised, white-yellow firm lesion with:
- A fibrous cap (SMCs + dense collagen + proteoglycans)
- A lipid/necrotic core (cholesterol, cholesterol esters, foam cell debris, necrotic material)
- Inflammatory infiltrate (macrophages, T cells, mast cells) at the shoulder regions
- Variable calcification ("hardening of the arteries")
Microscopic Appearance
- Fibrous cap: SMCs and ECM
- Core: extracellular lipid, cholesterol clefts, necrotic debris, foam cells
- Base/shoulders: rich in macrophages, lymphocytes, and new blood vessels
Distribution
- Most severe in the abdominal aorta > coronary arteries > popliteal arteries > internal carotid > circle of Willis
- Predilection for branch points, bifurcations, and vessel curves - areas of disturbed (turbulent/oscillatory) flow and low shear stress
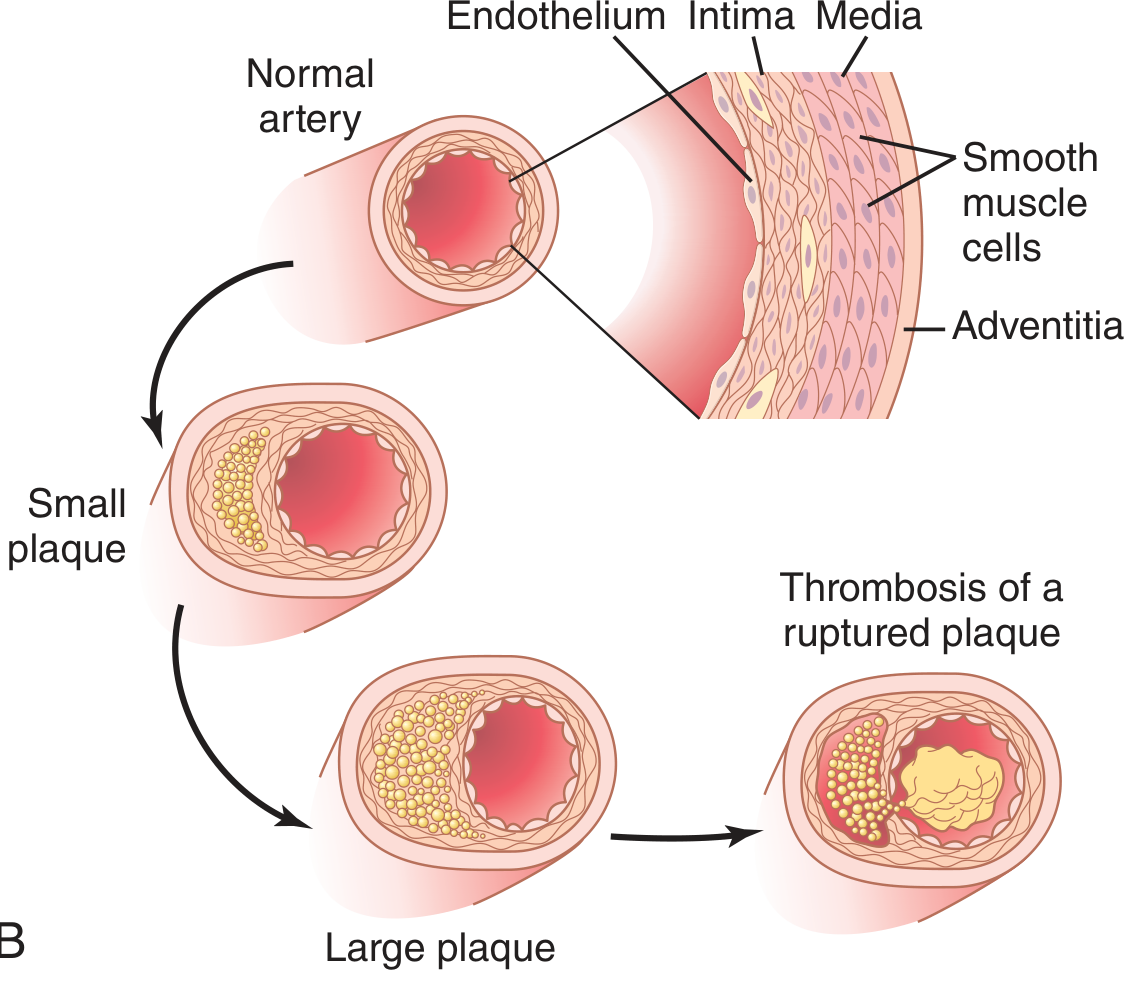
Fig. Progression of atherosclerotic plaque: normal artery → small plaque → large plaque → ruptured plaque with thrombosis (Guyton & Hall)
- Robbins Basic Pathology, p. 314-315; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 470-472
Stable vs. Vulnerable (Unstable) Plaques
| Feature | Stable Plaque | Vulnerable ("High-Risk") Plaque |
|---|---|---|
| Fibrous cap | Thick, dense | Thin, weak |
| Lipid core | Small | Large |
| Inflammation | Minimal | Dense macrophage/T-cell infiltrate |
| SMCs | Abundant | Sparse (MMP degradation) |
| Calcification | Often prominent | Variable |
| Risk of rupture | Low | High |
Vulnerable plaque rupture exposes the thrombogenic lipid core to circulating blood, triggering rapid platelet aggregation and thrombus formation - the mechanism underlying most acute MI and many strokes.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 472-473
Clinical Consequences
| Complication | Mechanism |
|---|---|
| Chronic stable ischemia (angina, claudication) | Progressive luminal stenosis reducing blood flow, especially during increased demand |
| Acute MI | Plaque rupture/erosion → thrombosis → acute vessel occlusion |
| Cerebral infarction (stroke) | Carotid/cerebral plaque rupture or embolization |
| Aortic aneurysm | Plaque ischemia weakens the medial wall → aneurysmal dilation, risk of rupture |
| Peripheral arterial disease | Limb ischemia, gangrene |
| Renal artery stenosis | Renovascular hypertension |
The summary from Robbins:
"Major consequences of atherosclerotic diseases include myocardial infarction, cerebral infarction, aortic aneurysms, and peripheral vascular diseases."
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 474
Calcification
Late plaques often undergo calcification - calcium salts precipitate with cholesterol and lipids, making arteries into rigid, bony-hard tubes. This "hardening of the arteries" impairs compliance and predisposes to rupture.
- Guyton and Hall Textbook of Medical Physiology, p. 851
Key Molecular Players Summary
| Component | Role |
|---|---|
| LDL / oxLDL | Primary lipid driver; oxLDL stimulates inflammation and is toxic |
| Scavenger receptors (SR-A, CD36) | Macrophage uptake of oxLDL → foam cells |
| VCAM-1, ICAM-1 | Monocyte/T-cell adhesion to damaged endothelium |
| MCP-1 (CCL2) | Chemokine driving monocyte recruitment into intima |
| PDGF, FGF | Growth factors driving SMC migration/proliferation |
| MMP (matrix metalloproteinases) | Cap degradation → plaque vulnerability |
| IFN-γ | T-cell cytokine inhibiting SMC collagen synthesis |
| NO (nitric oxide) | Endothelial-protective; reduced in dysfunction |
| CRP | Biomarker of systemic inflammation; independent predictor |
Sources
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10e), Chapter 11, pp. 465-474
- Robbins & Kumar Basic Pathology (11e), Chapter 8, pp. 313-316
- Guyton and Hall Textbook of Medical Physiology (14e), Chapter 69, p. 851
From srb surgery tb
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Unfortunately, SRB's Manual of Surgery (by Sriram Bhat) is not available in the library. The library contains Sabiston, Bailey & Love, Schwartz's, and a few others - but not SRB.
The closest surgical textbook match for atherosclerosis in the library is Sabiston Textbook of Surgery. Would you like me to pull the atherosclerosis content from that instead, or from any of the other available surgery books listed below?
Available surgery textbooks in the library:
- Bailey and Love's Short Practice of Surgery (28th Ed)
- Sabiston Textbook of Surgery
- Schwartz's Principles of Surgery (11th Ed)
- Fischer's Mastery of Surgery (8th Ed)
- Mulholland & Greenfield's Surgery (7th Ed)
- Current Surgical Therapy (14th Ed)
- S Das - A Manual on Clinical Surgery (13th Ed)
Let me know which one you'd like, or I can pull from all relevant surgery books on atherosclerosis.
Bailey and Iove
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have the complete atherosclerosis content from Bailey and Love. Here it is:
Atherosclerosis
Bailey and Love's Short Practice of Surgery (28th Edition)
Chapter 59 - Ischaemic Heart Disease
Definition / Overview
Atherosclerosis is the process underlying the formation of focal obstructions or plaques in large- and medium-sized arteries. It is a chronic inflammatory process resulting from interactions between:
- Plasma lipoproteins
- Leukocytes (monocytes/macrophages, T lymphocytes)
- Vascular endothelial cells
- Smooth muscle cells
It is the underlying pathology in ischaemic heart disease (IHD), which is a major cause of morbidity and mortality in resource-rich countries.
Progressive Stages of Atherosclerosis
Bailey and Love describes three distinct, progressive stages:
1. The Fatty Streak
- The first evidence of atherosclerosis can be found in children aged 10-14 years
- Appears as a yellow streak running along the major arteries
- Consists of:
- Smooth muscle cells filled with cholesterol
- Foam cells (lipid-laden macrophages)
2. Fibrous Plaque
- Consists of large numbers of smooth muscle cells, foam cells, and leukocytes
- As the fibrous plaque grows, it projects into the vessel lumen, causing narrowing
- This narrowing leads to ischaemia or infarction
3. Complicated Lesion
- Occurs when the fibrous plaque ruptures
- Provokes activation of the coagulation cascade and formation of thrombus
- End result: a calcified, ulcerated plaque with areas of haemorrhage and thrombus
Clinical Manifestations (IHD due to Atherosclerosis)
Principal symptoms include:
- Chest pain / angina (most characteristic)
- Breathlessness
- Fatigue
- Peripheral oedema
- Palpitations
- Syncope
Clinical examination may be normal, but may reveal murmurs, signs of heart failure, or stigmata of associated disease (diabetes, peripheral vascular disease).
Risk Factors for IHD (Summary Box 59.4)
| Modifiable | Non-modifiable |
|---|---|
| Smoking | Advancing age |
| Diabetes mellitus | Male gender |
| Hyperlipidaemia | Family history of IHD |
| Hypertension | - |
| Obesity | - |
| Reduced physical activity | - |
Investigations
Non-Invasive
| Test | Notes |
|---|---|
| Resting ECG (12-lead) | Baseline; may be normal even in severe multivessel disease. Q waves = old MI; ST depression = angina |
| Troponin / Cardiac enzymes | Useful in ACS (STEMI, non-STEMI, unstable angina). Creatine kinase-MB, LDH also used |
| Exercise Tolerance Test (ETT) | Valuable for diagnosing myocardial ischaemia and assessing severity |
| Echocardiography | Assesses LV function, wall motion abnormalities, valvular lesions |
| Radionuclide studies (Thallium-201 scan) | Myocardial perfusion scanning - assesses significance of coronary disease and myocardial viability |
| Cardiac MRI | Evaluates ischaemic burden (with pharmacological stress); gadolinium for tissue viability; useful for cardiac tumours, pericarditis |
| PET scan | Myocardial perfusion, metabolism and cell membrane function; identifies viable but injured myocardium salvageable by revascularisation |
| CT (ECG-gated, multislice) | Coronary calcium score; alternative to angiography for proximal CAD; useful in difficult anatomy |
Invasive
| Test | Notes |
|---|---|
| Coronary angiography | Gold standard for diagnosis of the presence and extent of CAD; remains definitive despite availability of newer modalities |
Bailey and Love's Short Practice of Surgery, 28th Ed., Chapter 59, pp. 969-970
Vascular disorders from Bailey and Iove
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is the complete Vascular Disorders chapter from Bailey and Love's Short Practice of Surgery (28th Edition), Chapter 61:
Vascular Disorders
Bailey and Love's Short Practice of Surgery, 28th Edition - Chapter 61
Introduction
Arterial disorders represent the most common cause of morbidity and early death in western societies. Much of this results from atheromatous plaque build-up (atherosclerosis) causing stenoses in arteries supplying the:
- Heart (coronary thrombosis and MI)
- Brain (stroke)
- Peripheral arterial system (limb ischaemia)
I. ARTERIAL STENOSIS AND OCCLUSION
Cause and Effect
- Predominantly caused by atherosclerosis and/or thromboembolic disease; also trauma
- Symptoms relate to the organ supplied:
- Lower limb: claudication, rest pain, gangrene
- Brain: TIAs and stroke
- Myocardium: angina and MI
- Intestine: abdominal pain and infarction
- Severity depends on:
- Size of vessel occluded
- Whether occlusion is acute (sudden, in a previously normal artery) or chronic (gradual, with collateral development)
- In chronic stenosis, a collateral circulation may develop as an alternative - albeit less effective - route for blood supply
II. CHRONIC LOWER LIMB ISCHAEMIA
Symptoms
Intermittent Claudication
- Cramping pain in the calf (most common), thigh or buttock on walking - relieved by rest
- Typical of femoral/popliteal disease (calf claudication) or aortoiliac disease (buttock/thigh)
- Fontaine classification describes severity of PAD
Chronic Limb-Threatening Ischaemia (CLTI)
- Rest pain (worse at night, relieved by hanging leg down)
- Tissue loss: ulceration or gangrene
Clinical Examination
Colour, Temperature, Sensation, Movement
- Acute ischaemia: cold, white, paralysed, insensate
- Chronic ischaemia: equilibrates with surroundings; no paralysis; sensation usually intact
- Sunset foot sign (dependent rubor): on elevation - venous guttering + pallor; on dependency - red/purple discolouration; indicates severe ischaemia
- Capillary refill: normally 2-3 seconds; may be prolonged to 10 seconds in severe ischaemia
Arterial Pulses
- Examine: femoral, popliteal, posterior tibial, dorsalis pedis
- Always examine abdomen for aortic aneurysm (may coexist)
- Pulsation distal to occlusion is usually absent
- After exercise (walking to claudication), pulse at iliac stenosis may disappear as vasodilation reduces pulse pressure
- Arterial bruit = turbulent flow = suggests stenosis (but tight stenoses may have no bruit)
III. INVESTIGATIONS
Non-Invasive
Ankle-Brachial Pressure Index (ABI)
- Ratio of systolic ankle pressure to ipsilateral brachial systolic pressure
- Highest pressure among dorsalis pedis, posterior tibial, or peroneal artery used as numerator
| ABI Value | Interpretation |
|---|---|
| 0.9 - 1.4 | Normal |
| < 0.9 | Haemodynamically significant arterial lesion |
| < 0.4 | Suggests CLTI |
| > 1.4 | Falsely elevated - media sclerosis/calcification (common in diabetes) |
- Drop of >20% in ABI after exercise = flow-limiting arterial disease
- In diabetics: Toe-Brachial Index (TBI) preferred (toe arteries rarely calcify); TBI <0.6 = significant lesion
- Absolute toe pressure <50 mmHg = severe ischaemia likely to prevent ulcer healing
Duplex Doppler Ultrasound (DUS)
- B-mode ultrasound imaging combined with Doppler flow analysis
- Colour coding visualises flow direction, velocity, turbulence
- As accurate as angiography in experienced hands; non-invasive and cost-effective
- Limitation: aortoiliac segment can be difficult to image (bowel gas)
Other Imaging
- CT Angiography (CTA): detailed anatomical imaging of entire arterial tree
- MR Angiography (MRA): no radiation; good for distal vessels
- Duplex surveillance for graft monitoring
Invasive
Catheter Angiography
- Gold standard for anatomy; used when intervention planned
- Usually via common femoral artery (CFA) approach
IV. MANAGEMENT
Risk Factor Modification
- Modifiable risk factors for PAD mirror those for CAD: smoking, diabetes, hypertension, hyperlipidaemia
- 50% of claudicants die within 10 years from MI or stroke
- Decrease in ABI of 0.1 below 0.9 = 10% increase in relative risk of major cardiovascular event
Non-Surgical Management
- Structured exercise programme: minimum 2 hours/week for 3 months - improves claudication distance and reduces cardiovascular risk
- Smoking cessation: most important modifiable factor
- Diabetes control + weight loss in obese patients
Drug Treatment
- Statins (HMG-CoA reductase inhibitors): prescribed even with normal lipids - stabilise atherosclerotic plaques and protect against cardiac death independently of lipid levels
- Antiplatelet therapy: Clopidogrel 75 mg/day (first line) OR Aspirin 75 mg/day
- Antihypertensives: caution with β-blockers (may exacerbate claudication)
- Vasodilators: unlikely to provide significant or sustained benefit
Transluminal Angioplasty and Stenting
- Percutaneous transluminal angioplasty (PTA): balloon inflation to dilate stenosis
- Stenting to maintain lumen patency after vessel recoil
- Best results for: short segment iliac stenoses (>90% patency at 3 years), femoral/popliteal lesions (variable)
Bypass Surgery
- Aortobifemoral bypass: for aortoiliac occlusive disease; midline abdominal incision; Dacron or PTFE graft; tunnelled retroperitoneally to groins
- Femoropopliteal bypass: for SFA/popliteal disease; autologous long saphenous vein preferred conduit (minimum 3 mm diameter); PTFE used if no suitable vein
- Femorodistal bypass: for tibial/crural disease; high early failure rate (~30% at 30 days); only for limb salvage
V. GANGRENE
- Death of macroscopic tissue - turns black (haemoglobin breakdown → iron sulphide formation)
- Usually affects most distal part of limb due to arterial obstruction
| Type | Cause | Features |
|---|---|---|
| Dry gangrene | Gradual arterial occlusion (typically atherosclerotic) | Desiccated, mummified; clear line of demarcation; minimal infection |
| Wet gangrene | Superadded infection and putrefaction | Oedematous, sloughy; spreads proximally; surgical emergency |
| Gas gangrene | Gas-forming organisms (common in diabetic foot) | Crepitus on palpation; urgent debridement or amputation |
Zone of Demarcation
- Granulation tissue forms between dead and living parts
- In dry gangrene: line forms in days if proximal supply adequate
- In wet gangrene: infection spreads proximally - demarcation more proximal
VI. ACUTE ARTERIAL OCCLUSION
- Usually caused by an embolus; also from thrombosis on atherosclerotic plaque (less dramatic - collaterals usually present)
Sources of Embolus
- Left atrium in atrial fibrillation (most common)
- Left ventricular mural thrombus after MI
- Vegetations on heart valves (infective endocarditis)
- Thrombi in aneurysms or on atherosclerotic plaques
The 6 Ps of Acute Limb Ischaemia (ALI)
Pain, Pallor, Paraesthesia, Paralysis, Pulselessness, Perishing cold
(Bailey and Love states the 5 Ps; paraesthesia/anaesthesia noted as 5th P)
Embolus vs. Thrombosis
| Feature | Embolus | Thrombosis on Atheroma |
|---|---|---|
| Onset | Sudden, dramatic | Less sudden |
| Previous history | Often none / AF, MI | Pre-existing claudication |
| Collaterals | Absent | Usually present |
| Contralateral pulses | Normal | Often abnormal |
| Severity | More severe | Less severe |
Management of ALI
- Immediate IV heparin (5000 U bolus)
- Embolectomy: via Fogarty balloon catheter through arteriotomy in CFA - catheter passed proximal and distal, balloon inflated, withdrawn with clot; repeated until backbleeding
- Thrombolysis: intra-arterial tissue plasminogen activator (tPA) if ischaemia not immediately limb-threatening; catheter embedded in clot via CFA approach; serial angiograms to monitor lysis
- Post-procedure: heparin → warfarin (long-term anticoagulation) to prevent re-embolism
VII. AMPUTATION
Indications (The 3 Ds)
Dead limb: Gangrene - occlusion irreversible; arterial, embolic, diabetic small vessel disease, Buerger's, Raynaud's
Deadly limb: Wet gangrene with spreading cellulitis/toxaemia; gas gangrene; arteriovenous fistula; malignancy
Dead loss limb: Severe rest pain with unreconstructable CLTI; paralysis; contracture; major trauma
Levels of Amputation
- Distal/toe: small vessel disease with good proximal supply (diabetes)
- Transmetatarsal: several toes affected but proximal circulation adequate
- Below-knee (BKA): preserves knee joint; better rehabilitation
- Above-knee (AKA): poorer stump healing; worse rehabilitation
VIII. ANEURYSMAL DISEASE
Definition and Classification
- Aneurysm: abnormal localised dilatation >50% of normal vessel diameter (below 50% = ectatic)
- True aneurysm: all three layers of arterial wall (intima, media, adventitia) in sac
- False (pseudo)aneurysm: single layer of fibrous tissue (e.g. post-trauma, post-puncture)
By shape: Fusiform (commonest) or Saccular
By aetiology: Atheromatous (majority), traumatic, mycotic (bacterial infection - a misnomer; not fungal), congenital
Sites: Aorta, iliac, femoral, popliteal, subclavian, axillary, carotid, cerebral, mesenteric, splenic, renal arteries
Abdominal Aortic Aneurysm (AAA)
Definition: Aortic diameter >3 cm (normal ~2 cm); aneurysmal when >3 cm; most require repair at ≥5.5 cm (rupture risk exceeds operative risk)
Clinical Features
- Majority asymptomatic - found incidentally on USS or CT
- Symptomatic: pulsatile abdominal mass, back/loin pain (expansion), abdominal pain
- Thrombus within sac may give false impression of diameter on angiography
Investigations
- USS: screening; monitors size; cannot diagnose rupture
- CT: definitive; measures size accurately; detects rupture; guides EVAR planning
Repair indications
- Diameter ≥5.5 cm
- Rapid expansion (>1 cm/year)
- Symptomatic aneurysm
- Ruptured aneurysm (emergency)
Open Surgical Repair
- Midline or transverse abdominal incision (avoid transverse - divides inferior epigastric collateral vessels)
- Small bowel retracted right; posterior peritoneum opened; aorta exposed below renal arteries
- Heparin 5000 U IV; clamps above and below lesion
- Dacron inlay graft anastomosed end-to-end proximally; distally to aortic bifurcation or iliac arteries
Endovascular Aneurysm Repair (EVAR)
- Stent-graft deployed via femoral arteries under radiological guidance
- Less invasive; faster recovery; lower short-term mortality
- NICE 2020 (UK): recommends open repair unless contraindicated; EVAR for high-risk patients
- ESC 2019: EVAR as first-line; open for patients with long life expectancy
- EVAR first-line for anatomically suitable ruptured AAA
Ruptured AAA - Emergency Management
- Classic triad: severe abdominal/back pain + hypotension + pulsatile abdominal mass
- Rupture: 80% posterolateral (retroperitoneal) - may be temporarily tamponaded; 20% anterior (free peritoneal) - rapidly fatal
- Less than 50% survive to reach hospital; operative mortality ~50%; overall mortality 80-90%
- Management: IV access; permissive hypotension (systolic <100 mmHg - just enough to maintain consciousness); CT to confirm; immediate transfer to theatre; EVAR if anatomically suitable
Popliteal Aneurysm
- Most common peripheral aneurysm
- Over 50% bilateral; associated with AAA in 30-40%
- Complications: distal embolisation (causing foot ischaemia), thrombosis, rarely rupture
- Chronic embolisation occludes run-off vessels → eventual thrombosis → ischaemic foot
- Elective repair: bypass with vein graft via medial approach (preferred over posterior approach for better exposure)
- Acute thrombosis: poor prognosis; limb loss rate ~50%
Femoral Aneurysm
- True femoral aneurysm: uncommon; complications <3%; conservative unless large
- Always look for associated AAA or popliteal aneurysm (>50% association)
- False femoral aneurysm: 2% after arterial surgery; or post-puncture
- ≤3 cm: thrombin injection under USS guidance
-
3 cm: open surgical repair
Iliac Aneurysm
- Usually associated with AAA; rarely isolated
- ~50% present already ruptured when isolated
- Treatment: inlay graft or endovascular repair
IX. ARTERIOVENOUS FISTULA
- Communication between artery and vein
- Congenital malformation or acquired (trauma)
- Surgically created AV fistulae used for haemodialysis access
X. VASOSPASTIC DISORDERS
Raynaud's Disease (Primary)
- Episodic digital vasospasm triggered by cold or emotion
- Triphasic colour change: white (pallor) → blue (cyanosis) → red (reactive hyperaemia)
- No underlying cause identified
- Management: keep warm; calcium channel blockers (nifedipine); sympathectomy in severe cases
Raynaud's Syndrome (Secondary)
- Peripheral arterial manifestation of underlying collagen disease (SLE, rheumatoid arthritis)
- Also caused by vibrating tools ("vibration white finger" - recognised industrial disease)
- More aggressive; may lead to digital necrosis and multiple amputations
- Treatment: directed at underlying condition; nifedipine, steroids, vasospastic antagonists
- Sympathectomy: disappointing results; not recommended
Bailey and Love's Short Practice of Surgery, 28th Ed., Chapter 61, pp. 1019-1045
Note: The sections on varicose veins, deep vein thrombosis, and lymphatic disorders are covered separately in Bailey and Love (Chapters 62-63). Reply with "continue" if you'd like those sections covered with a fresh budget.
Continue also explain buergers disease
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is the continuation - Chapter 62 (Venous Disorders) plus the Arteritis and Vasospastic conditions including Buerger's disease in full detail:
Vascular Disorders (Continued)
Bailey and Love's Short Practice of Surgery, 28th Edition
XI. ARTERITIS AND VASOSPASTIC CONDITIONS
Buerger's Disease (Thromboangiitis Obliterans)
Definition: A non-atherosclerotic, segmental, inflammatory disease affecting small and medium-sized arteries and veins of the extremities.
Characteristics (Bailey and Love):
- Occlusive disease of small and medium-sized limb arteries
- Thrombophlebitis of superficial or deep veins
- Raynaud's syndrome (vasospastic component)
- Occurs almost exclusively in young male smokers
- Histology: inflammatory changes in the walls of both arteries and veins leading to thrombosis
Key Features:
- Affects upper and lower limbs (unlike atherosclerosis, which predominantly affects lower limbs)
- Common in Middle East, Asia, Eastern Europe - less common in Western Europe
- No other atherosclerotic risk factors needed - smoking is the dominant and essential factor
- Thrombophlebitis migrans: flitting thrombophlebitis affecting different veins at different times; seen in Buerger's disease and malignancy (especially pancreatic)
Clinical Features:
- Rest pain and digital ischaemia in young men (<45 years) who smoke
- Ulceration and gangrene of digits (fingers and toes)
- Superficial thrombophlebitis (nodular tender cord along a vein)
- Raynaud's phenomenon
- Absent distal pulses with relatively preserved proximal pulses
Treatment:
- Total abstinence from smoking - the only effective treatment; arrests but does NOT reverse the disease
- Established arterial occlusions managed as for atheromatous disease (angioplasty, bypass if possible)
- Amputation may eventually be required (digits or limbs if gangrene develops)
- Sympathectomy may provide temporary relief
"Treatment is total abstinence from smoking, which arrests, but does not reverse, the disease." - Bailey and Love, Ch. 61
Other Forms of Arteritis
Temporal Arteritis (Giant Cell Arteritis)
- Localised infiltration with inflammatory and giant cells → arterial occlusion
- Features: ischaemic headache, tender + palpable + pulseless (thrombosed) temporal arteries
- Emergency: irreversible blindness if ophthalmic artery occluded
- Surgeon's role: temporal artery biopsy (confirms diagnosis) - but must NOT delay immediate steroid therapy
- Steroids arrest and reverse the process before ophthalmic artery involvement
Takayasu's Disease
- Arteritis obstructing major arteries, particularly large vessels off the aortic arch
- Usually pursues a relentless course
- Young women; also called "pulseless disease"
Cystic Myxomatous (Adventitial Cystic) Degeneration
- Accumulation of clear jelly (like a synovial ganglion) in the outer layers of a main artery, especially the popliteal artery
- Narrows the vessel → claudication in young patients without risk factors
- Investigation: Duplex scan (choice)
- Treatment: decompression by removal of myxomatous material; sometimes requires excision of diseased artery
XII. CHAPTER 62 - VENOUS DISORDERS
Venous Anatomy of the Lower Limb
Deep Venous System (beneath deep fascia):
- Three pairs of venae comitantes alongside anterior tibial, posterior tibial and peroneal arteries
- Converge in popliteal fossa → popliteal vein (also receives soleal and gastrocnemius veins)
- Popliteal vein → through adductor hiatus → femoral vein (receives profunda femoris vein in femoral triangle) → external iliac vein → common iliac vein → inferior vena cava
Superficial Venous System (within superficial fascia):
- Great Saphenous Vein (GSV): longest vein in the body; ascends medially; joins femoral vein at saphenofemoral junction (SFJ) in the groin
- Small Saphenous Vein (SSV): runs posterolaterally; joins popliteal vein at saphenopopliteal junction (SPJ) in popliteal fossa
Perforating (communicating) veins: Connect superficial to deep system through fascia; valves normally allow flow only from superficial → deep.
Calf Muscle Pump Physiology
- Venous pressure in foot on standing ≈ 100 mmHg (hydrostatic column to heart)
- Blood returns against gravity via:
- Inspiration → decreased intrathoracic pressure creates suction
- Calf muscle pump: compression of deep veins raises pressure to 200-300 mmHg during contraction; one-way valves direct flow toward heart
- Calf pump reduces superficial venous pressure to ≈30 mmHg (two-thirds reduction)
- Venous hypertension occurs when: valves incompetent, deep veins obstructed, or pump failure
XIII. VARICOSE VEINS
Definition
Dilated, tortuous, elongated superficial veins due to valve incompetence and venous hypertension.
Prevalence
- 30-50% of the adult population
- More common in women; increases with age; Edinburgh Vein Study prevalence rose from 11.5% (age 18-24) to 55.7% (age 55-64)
- Risk factors: female sex, increasing age, pregnancy, family history, obesity, tall stature
Pathophysiology
- Primary failure of venous valves → retrograde blood flow (reflux) → venous hypertension
- Raised pressure → vein wall weakening via matrix metalloproteinases → loss of compliance, dilatation, elongation, further valvular dysfunction
- Secondary varicose veins: arise post-DVT (post-thrombotic limb) or in congenital abnormalities (e.g. Klippel-Trénaunay syndrome)
CEAP Classification (Clinical features)
| Feature | Description |
|---|---|
| Telangiectasia (thread veins) | Intradermal venules <1 mm |
| Reticular veins | Subdermal bluish 1-2.9 mm veins |
| Varicose veins | Tortuous dilated subcutaneous veins |
| Corona phlebectatica | Fan-shaped telangiectasia at ankle - early sign of advanced disease |
| Saphena varix | Dilated vein at SFJ - painless groin swelling on standing, disappears lying |
| Oedema | Pitting oedema; starts distally |
| Eczema | Erythematous dermatitis; may itch |
| Pigmentation (haemosiderosis) | Brownish discolouration at ankle |
| Lipodermatosclerosis (LDS) | Chronic inflammation/fibrosis; 'woody' contracted leg; Achilles contracture |
| Atrophie blanche | Localised atrophic white skin patches |
| Venous ulceration | Full-thickness skin loss in 'gaiter area' |
Symptoms
- Aching, heaviness, throbbing, burning, bursting sensation
- Worse throughout the day and with prolonged standing
- Relieved by elevation or compression hosiery
- Itching, ankle swelling
- Symptoms independent of degree of incompetence
Investigation
- Duplex ultrasound: mandatory for ALL patients; assesses:
- Site and source of reflux
- Deep vein patency (obstruction)
- Suitability of veins for treatment (diameter, tortuosity, thrombus)
- Pelvic source of reflux
- Reflux defined: retrograde flow ≥0.5 seconds in superficial veins (≥1 second in proximal deep veins)
- Hand-held Doppler and tourniquet tests have been abandoned
Treatment
Conservative
- Compression hosiery (graduated elastic stockings)
- Suitable for patients unfit for intervention or who decline treatment
Endovenous Thermal Ablation (First-line per NICE guidelines)
- Endovenous Laser Ablation (EVLA): laser fibre inserted percutaneously; tumescent local anaesthetic surrounds vein; thermal energy destroys vein permanently; wavelength typically 1470 nm
- Radiofrequency Ablation (RFA): similar principle using radiofrequency energy; may have marginally less post-procedure pain
- Both preceded by tumescent anaesthesia injection around vein (compresses vein, dissects nerve, acts as heat sink)
- RFA preferred for veins <15 mm; EVLA better for very large veins (>15 mm) and cheaper consumables
Non-endothermal, Non-tumescent (NTNT) Techniques
- Ultrasound-guided foam sclerotherapy (UGFS): sclerosing agent (sodium tetradecyl sulphate) foamed and injected into vein; causes endothelial destruction, thrombosis, fibrosis, obliteration; blood deactivates agent so foam used to maximise contact
- Mechanochemical ablation (MOCA): combined mechanical disruption + sclerosant
- Cyanoacrylate (glue) ablation: no tumescent anaesthetic needed
Surgical Treatment
- Saphenofemoral junction (SFJ) ligation + GSV stripping (Trendelenburg operation)
- Saphenopopliteal junction (SPJ) ligation + SSV stripping (prone position; preoperative duplex mapping mandatory)
- Phlebectomy: stab avulsion of varicosities through small incisions using mosquito forceps/phlebectomy hooks; performed concomitant or sequentially; can be done under local anaesthetic
- Perforator ligation: subfascial endoscopic perforator surgery (SEPS) if indicated
Complications of Varicose Veins
- Thrombophlebitis (superficial vein thrombosis)
- Bleeding (from varicosity - usually minor but alarming; elevate limb and apply pressure)
- Venous eczema
- Lipodermatosclerosis
- Venous ulceration
XIV. DEEP VEIN THROMBOSIS (DVT) AND VENOUS THROMBOEMBOLISM (VTE)
Pathophysiology (Virchow's Triad)
- Venous stasis (immobility, surgery, long travel)
- Endothelial damage (trauma, surgery, inflammation)
- Hypercoagulability (thrombophilia, malignancy, OCP)
Thrombus begins as platelet aggregate → fibrin and red cell mesh forms → lumen occludes → coralline thrombus propagates proximally (clot tail is loose and prone to embolisation)
Risk Factors (Table 62.2)
| Patient Factors | Disease/Surgical Factors |
|---|---|
| Age | Pelvic/hip/lower limb surgery or trauma |
| Obesity | Malignancy (especially pelvic, abdominal, metastatic) |
| Varicose veins | Heart failure |
| Immobility | Recent MI |
| Pregnancy / puerperium | Paralysis of lower limb |
| High-dose oestrogen therapy | Infection; IBD; nephrotic syndrome |
| Previous DVT/PE | Polycythaemia; paraproteinaemia |
| Thrombophilia | Homocystinaemia |
Thrombophilia (Table 62.3)
- Antithrombin deficiency
- Protein C or protein S deficiency
- Factor V Leiden (activated protein C deficiency) - most common; present in 6-7% of white populations
- Prothrombin gene mutation
- Antiphospholipid syndrome
- Screen when: VTE with family history, no provoking factor, recurrent VTE, or young age
Clinical Features of DVT
- Calf pain, swelling, tenderness, erythema, warmth
- Homan's sign (calf pain on dorsiflexion of foot) - non-specific; should NOT be routinely elicited
- Tenderness in 75% - but also in 50% without DVT
- Clinical signs of PE in ~10% of confirmed DVT: cyanosis, dyspnoea, raised JVP, fixed split S2, pleural rub
Investigation - Modified Wells Score (Table 62.4)
| Variable | Score |
|---|---|
| Lower limb trauma/surgery/plaster cast | +1 |
| Bedridden >3 days or surgery within 4 weeks | +1 |
| Tenderness along femoral or popliteal veins | +1 |
| Entire limb swollen | +1 |
| Calf >3 cm larger than opposite side (10 cm below tibial tuberosity) | +1 |
| Pitting oedema | +1 |
| Dilated collateral superficial veins (not varicosities) | +1 |
| Previous DVT | +1 |
| Malignancy (including treatment in last 6 months) | +1 |
| IV drug abuse | +3 |
| Alternative diagnosis more likely than DVT | -2 |
- Score -2 to 0: Low probability (5%)
- Score 1-2: Moderate probability (17%)
- Score >2: High probability (17-53%)
Imaging:
- Venous Duplex Ultrasound: first-line; compression ultrasound - veins normally compress completely; in DVT, they do not
- CT Pulmonary Angiogram (CTPA): definitive for pulmonary embolism - shows filling defects in pulmonary arteries
- Pulmonary angiography: rarely required unless thrombolysis being considered
Differential diagnoses of DVT: ruptured Baker's cyst, calf muscle haematoma, ruptured plantaris, thrombosed popliteal aneurysm, arterial ischaemia
Prophylaxis
Mechanical:
- Graduated elastic compression stockings
- External pneumatic compression (intermittent pneumatic compression - IPC)
- Avoid in peripheral vascular disease (can worsen ischaemia)
- Electronic nerve stimulators - insufficient evidence
Pharmacological (more effective than mechanical):
- LMWH (low-molecular-weight heparin): once daily subcutaneous; no monitoring; lower bleeding risk; preferred in most patients
- Unfractionated heparin (UFH): IV or subcutaneous; used in renal impairment
- Risk stratification: low/medium/high risk for PE - medium and high risk groups should receive pharmacological prophylaxis
Treatment
DVT:
- Rapid anticoagulation: treatment-dose LMWH subcutaneously
- Renal impairment: IV unfractionated heparin
- Heparin-induced thrombocytopenia (HIT): fondaparinux (factor Xa inhibitor) or bivalirudin (direct thrombin inhibitor)
- Oral anticoagulation for minimum 3 months (longer if persistent risk factors or recurrent DVT):
- NOACs (preferred): rivaroxaban or apixaban (direct factor Xa inhibitors) or dabigatran (direct thrombin inhibitor)
- Equally effective as warfarin; fewer major bleeding complications
- Warfarin (VKA) if NOACs contraindicated
- IVC filter: if anticoagulation contraindicated (bleeding risk); temporary/retrievable preferred
- Endovascular surgery (selected patients, e.g. iliofemoral DVT): thrombus removal, thrombolysis, stenting - reduces risk of post-thrombotic syndrome
Pulmonary Embolism:
- Most: anticoagulation + observation
- Severe (right heart strain, haemodynamic compromise): systemic thrombolysis or catheter-directed embolectomy
Superficial Vein Thrombosis (Thrombophlebitis)
- Previously called thrombophlebitis
- Abnormal endothelium is more common precipitant than in DVT
- Causes: trauma to varicose veins, IV cannula (>24-48 hours), infusions of hyperosmolar solutions, Buerger's disease, malignancy (pancreatic cancer → thrombophlebitis migrans)
- Surface vein: solid, tender, overlying skin erythematous early → turns brown
- Management: anti-inflammatory drugs, compression, consider anticoagulation if near SFJ (risk of propagation to deep system)
Bailey and Love's Short Practice of Surgery, 28th Ed., Chapters 61-62, pp. 1019-1070
This is a shared conversation. Sign in to Orris to start your own chat.