Dental abscess rdiology interpretation
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
dental abscess periapical radiograph radiolucency
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
I now have comprehensive content. Let me compile a thorough, well-illustrated answer.
Dental Abscess — Radiology Interpretation
Pathogenesis & Radiological Background
A dental (odontogenic) abscess typically begins with bacterial invasion from dental caries → pulp → periapical tissues. The radiological changes reflect progressive bone destruction driven by infection.
Radiographic Modalities
| Modality | Role |
|---|---|
| Intraoral periapical (IOPA) | First-line; best detail of root apex and periapical bone |
| Bitewing | Detects interproximal caries and bone height; poor apex visualization |
| Panoramic (OPG/Panorex) | Surveys all teeth; poor sensitivity for early periapical disease |
| CBCT | Gold standard for 3D extent, cortical perforation, proximity to vital structures |
| CT (soft tissue) | Evaluates spread into deep fascial spaces (Ludwig's angina, cellulitis) |
A panorex is not typically useful for periradicular periodontitis but can be important in identifying other painful osseous pathology. — Tintinalli's Emergency Medicine
Stage-by-Stage Radiographic Features
1. Normal Anatomy (Reference)
Before recognizing pathology, understand the normal landmarks:
- Lamina dura: thin radiopaque line lining the tooth socket — intact, sharp, and continuous
- Periodontal ligament (PDL) space: thin, uniform radiolucent line (0.2–0.3 mm) around the root
- Trabecular bone: normal honeycomb pattern

2. Early Periradicular Periodontitis (Acute)
The earliest radiographic signs are subtle and may be absent in acute abscess (pus can form before bone is destroyed):
- Slight widening of the PDL space at the apex
- Thinning or loss of lamina dura at the root tip
- May appear completely normal in the first 48–72 hours
3. Established Periapical Abscess / Granuloma / Cyst
As infection progresses and becomes chronic, a well-defined lesion develops:
| Feature | Abscess | Granuloma | Radicular Cyst |
|---|---|---|---|
| Shape | Diffuse/irregular | Round/oval | Round, well-defined |
| Borders | Ill-defined, non-corticated | Well-defined | Corticated (white border) |
| Size | Variable | Usually <1 cm | Often >1 cm |
| Location | Root apex | Root apex | Root apex |
| Density | Radiolucent | Radiolucent | Radiolucent |
All three are radiographically indistinguishable in many cases — clinical context, symptoms, and histopathology are needed for definitive differentiation. — Tintinalli's Emergency Medicine
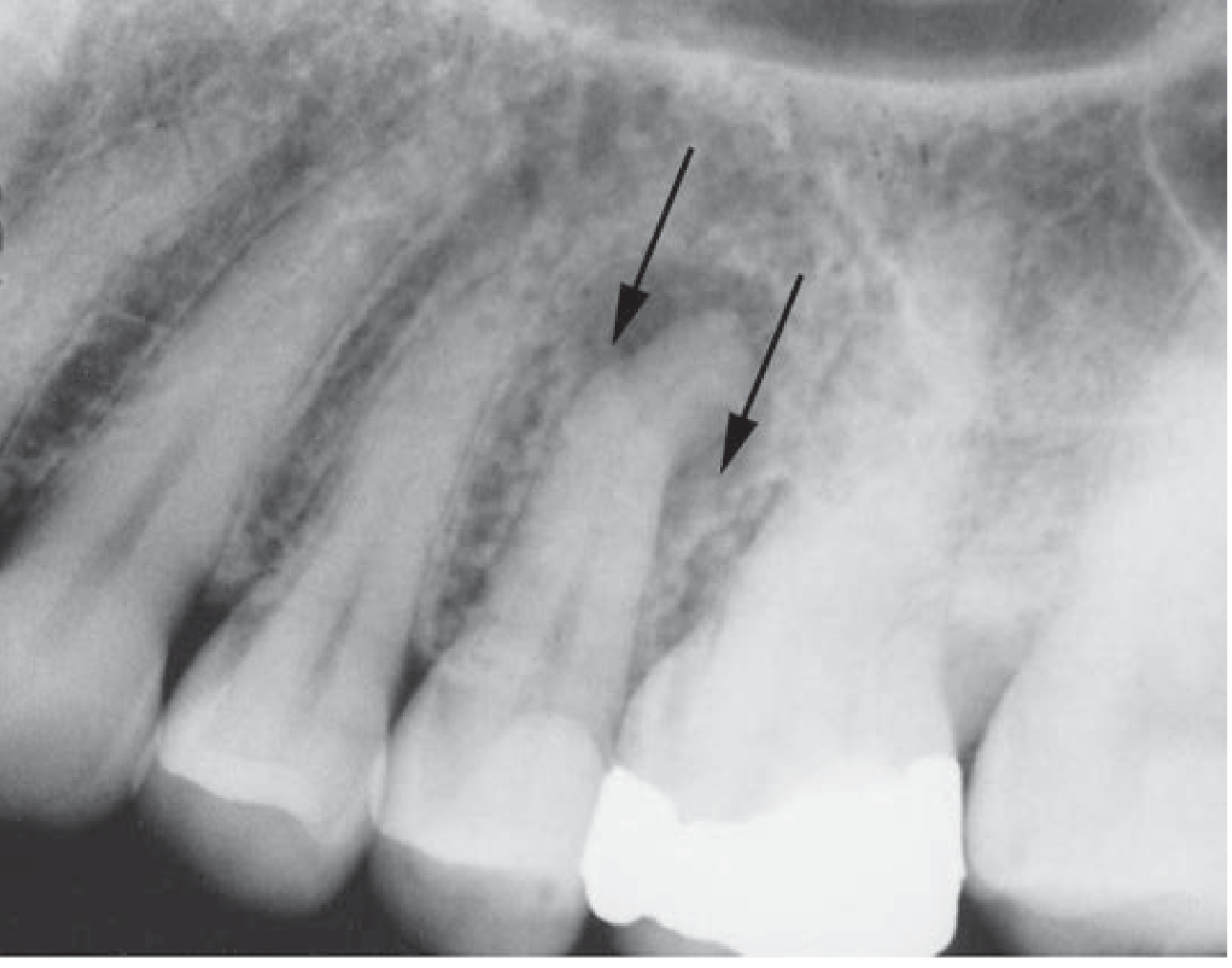
4. Example: Mandibular Molar with Periapical Pathology

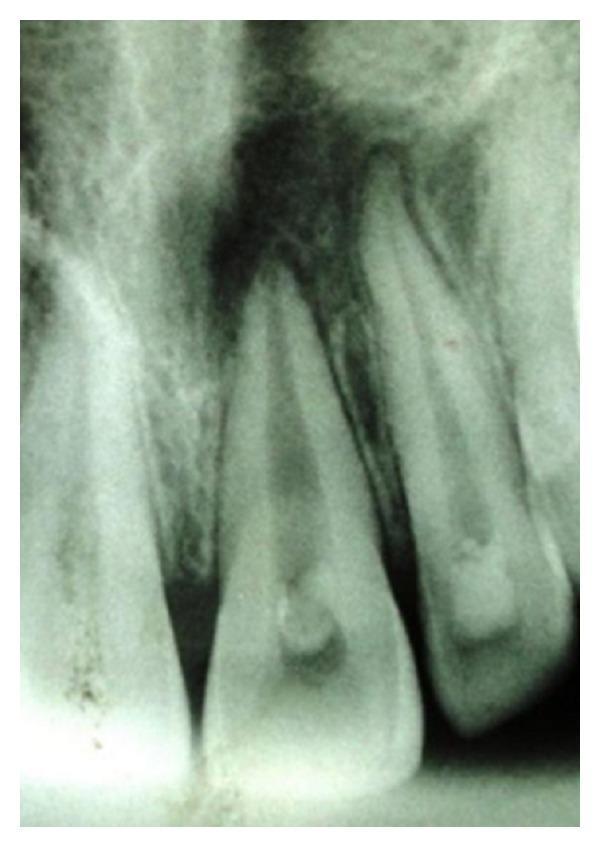
5. Example: Anterior Teeth — Chronic Periapical Abscess
6. Sinus Tract (Parulis) — Pathognomonic Sign
A gutta-percha point inserted into a sinus tract and then radiographed traces the tract directly to the offending root apex — this is a pathognomonic finding confirming the source tooth.

Key Radiographic Signs — Summary
| Sign | Significance |
|---|---|
| Widened PDL space at apex | Earliest indicator of periapical disease |
| Loss/interruption of lamina dura | Bone resorption at socket wall |
| Periapical radiolucency | Established periapical pathology (abscess, granuloma, or cyst) |
| Ill-defined radiolucency | Favors active/acute abscess |
| Well-corticated radiolucency | Favors cyst (chronic process) |
| Furcation radiolucency | Advanced infection; pulp floor perforation |
| Cortical bone destruction | Spreading abscess; may indicate osteomyelitis |
| Gutta-percha tracing to apex | Confirms source tooth via sinus tract |
Complications to Look For on Radiographs
As stated in Harrison's Principles of Internal Medicine 22E: "A periapical abscess can erode into the alveolar bone, producing osteomyelitis; penetrate and drain through the gingivae, producing a parulis (gum-boil); or track along deep fascial planes, producing virulent cellulitis (Ludwig's angina)."
On radiograph/CT look for:
- Diffuse bone destruction or "moth-eaten" pattern → osteomyelitis
- Cortical perforation → soft tissue extension (best seen on CBCT or CT)
- Maxillary sinus haziness/mucosal thickening → odontogenic sinusitis (upper premolars/molars)
- Mandibular canal proximity → inferior alveolar nerve involvement
Practical Tip: Acute vs. Chronic
- Acute abscess: May show no radiographic changes or only minimal PDL widening. Clinical signs (pain, swelling, fever) drive diagnosis.
- Chronic abscess/granuloma: Well-established periapical radiolucency; patient may be asymptomatic (incidental finding on routine radiograph).
Sources: Tintinalli's Emergency Medicine, Ch. 245; Harrison's Principles of Internal Medicine 22E, Ch. 304.
This is a shared conversation. Sign in to Orris to start your own chat.